

CHAPTER 4: WRIST AND HAND
A. LIGAMENT/INSTABILITY TESTS
* Piano key test
* Radial collateral ligament stress test
* Ulnar collateral ligament stress test
* Scaphoid shift test
* Lunotriquetral shear test
* Capitate apprehension test
B. TRIANGULAR FIBROCARTILAGE COMPLEX (TFCC) TESTS
* TFCC load test
C. THUMB TESTS
* Axial compression test
* Finkelstein’s test
* Ulnar collateral ligament laxity test
D. CARPAL TUNNEL TESTS
* Phalen’s test
* Tinel’s test
* Carpal compression test
A. LIGAMENT/INSTABILITY TESTS
Piano Key Test
Purpose
To detect the presence of instability at the inferior radio-ulnar joint (IRUJ).
Technique
*
Patient position:
Sitting with the forearm fully pronated and supported on a table.
*
Clinician position:
Sitting facing the patient, one hand stabilizes the patient’s hand in a neutral position while, approaching from the radial aspect, the index and middle fingers of the other hand are placed over the head of the ulna with the thumb providing some counterpressure under the base of the radius.
*
Action:
Downward pressure is applied by the fingers on the distal ulna, mimicking the action of pressing down a piano key.
*
Positive test:
Pain accompanied by excess movement and a loss of the normal ligamentous end-feel is noted.

FIG 4.1: Piano key test.
Clinical context
Isolated involvement of the IRUJ is rare and is usually associated with more significant injury at the wrist (i.e. fracture or dislocation). Minor disruption may cause pain as the primary sign and this would be well localized with tenderness easily elicited by palpation. Pain at the end of passive pronation and supination would also be provocative. Where ligament disruption has occurred, excess movement will be accompanied by apprehension during certain activities, particularly in weight-bearing positions where its lack of stability is more seriously tested.
The IRUJ is often involved in inflammatory arthritis and in more severe cases, the synovitis afflicting the joint causes a destructive process resulting in pronounced loss of rotation, dorsal prominence and instability of the ulna, as well as localized swelling and loss of the normal function of the adjacent extensor carpi ulnaris, a condition known as caput ulnae syndrome (Brown & Neumann 2004). Given the associated joint stiffness, despite the instability at the IRUJ, the piano key test may not yield a positive result.
**Clinical tip:** The joint line is easily palpable on the dorsum of the lower forearm. The width of the wrist dorsally can be divided into three equal portions, making the joint line the marker between the most medial and middle sections. If the result of this test is ambiguous, further accessory testing of the IRUJ can be done to detect changes in range and end-feel.
**EXPERT OPINION (★★★):** Especially useful to determine level of instability – only a very unstable joint will behave like a true ‘piano key’.
Radial Collateral Ligament Stress Test
Aka: Wrist adduction test
Purpose
To stress the radial collateral ligament (RCL) and lateral capsule of the wrist in order to detect pain and/or laxity.
Technique
*
Patient position:
Sitting with the wrist supported on a table.
*
Clinician position:
One hand fixes the distal forearm by wrapping the fingers around the radius and ulna while the other grasps the hand, taking care not to involve the fingers or thumb.
*
Action:
With the forearm fixed, the distal hand takes the wrist into ulnar deviation (wrist adduction) where normal range is between 30° and 45°.
*
Positive test:
Pain is the most likely outcome but further evaluation would be needed if excessive range was noted suggesting significant disruption to the joint.

FIG 4.2: Radial collateral ligament stress test.
Clinical context
This test is most likely to identify an isolated sprain of the RCL where localized pain around the anatomical snuffbox would be the primary complaint. Depending on the severity of the trauma, a varying but equal degree of flexion/extension restriction may also be present at the wrist as the ligament blends with, and reinforces, the lateral joint capsule, thereby causing capsular limitation.
As the history is usually traumatic, careful screening is necessary (including X-ray evaluation in most cases) to eliminate fracture of the carpus—the scaphoid being the usual culprit. With pain reported in this area, osteoarthritis of the trapeziofirstmetacarpal joint (basal joint of the thumb; see axial compression test) and de Quervain’s tenosynovitis (see Finkelstein’s test) are other possible diagnoses to consider.
**Clinical tip:** The RCL can be found by identifying the radial styloid at the base of the anatomical snuffbox and moving the finger slightly distally with the wrist in a degree of radial deviation. The ligament and capsule are relaxed in this position. Keeping the finger in place, the RCL tautens (if intact) and becomes easily palpable as the wrist is passively taken into ulnar deviation. Make sure the patient’s thumb is not involved in this movement in order to avoid stress being placed on the thumb abductor and extensor tendons which may result in a false positive finding.
**EXPERT OPINION (★):** Usually included as part of radiocarpal assessment without specifically testing the ligaments as they are rarely injured in isolation.
Ulnar Collateral Ligament Stress Test
Aka: Wrist abduction test
Purpose
To stress the ulnar collateral ligament (UCL) and medial capsule of the wrist in order to detect pain and/or laxity.
Technique
*
Patient position:
Sitting with the wrist supported on a table.
*
Clinician position:
One hand fixes the distal forearm by wrapping fingers around the radius and ulna while the other grasps the hand, taking care not to involve the fingers or thumb.
*
Action:
With the forearm fixed, the distal hand takes the wrist into radial deviation (wrist abduction) where normal range is around 15°.
*
Positive test:
Pain is the most likely outcome but further evaluation would be needed if excessive range was noted, suggesting significant disruption to the joint.

FIG 4.3: Ulnar collateral ligament stress test.
Clinical context
The patient reports localized pain located at the inner, medial aspect of the wrist joint. If the UCL stress test is the only positive test, confirmation of the lesion can be made by palpation—tenderness is usually identifiable at its origin on the ulnar styloid. Isolated injury to the UCL is rare and, because of its anatomical connection, is more commonly associated with injury to the triangular fibrocartilaginous complex (see TFCC test). Medial wrist pain may also emanate from the inferior radio-ulnar joint (see piano key test) and the extensor carpi ulnaris tendon.
**Clinical tip:** The ligament is most easily identified by finding the styloid with the wrist in ulnar deviation and then passively moving the wrist radially until the ligament can be felt tautening under the finger.
**EXPERT OPINION (★):** Usually included as part of radiocarpal assessment without specifically testing the ligaments as they are rarely injured in isolation.
Scaphoid Shift Test
Aka: Watson test
Purpose
To establish the presence of abnormal movement of the scaphoid and lunate bones indicating instability or subluxation.
Technique
*
Patient position:
The patient is seated with the flexed elbow resting on a table, the forearm vertically positioned and fully pronated so that the patient’s palm faces the clinician.
*
Clinician position:
Seated facing the patient, the examiner places the thumb in the palm and wraps the fingers around the metacarpals on the dorsum of the hand. The thumb of the second hand is placed over the tubercle of the scaphoid and counterpressure applied with the other fingers over the dorsum of the lower radius.
*
Action:
Firm pressure is applied on the scaphoid while the hand is taken initially into ulnar deviation and slight extension to offload the scapholunate articulation. Maintaining the pressure on the scaphoid, the wrist is then taken slowly into radial deviation and slight flexion creating a subluxation force that stresses the articulation and exposes instability if present.
*
Positive test:
Excessive movement of the scaphoid in relation to the lunate is detected along with some pain and/or apprehension. If subluxation occurs the proximal pole of the scaphoid shifts dorsally over the dorsal rim of the radius. Removing the pressure from the palmar aspect of the scaphoid and returning the wrist into some ulnar deviation and extension will cause the scaphoid to shift back in a palmar direction to its reduced, normal position.




FIG 4.4: Scaphoid shift test: unloaded start position (A) and stress applied to the scapholunate joint (B).
Clinical context
Although comparatively rare, the instability that results from disruption of the scapholunate articulation is the most common carpal instability. A complete tear of the scapholunate ligaments, usually resulting from a severe hyperextension injury, will lead to significant scapholunate dissociation and disruption to the normal motion of the proximal carpal bones during wrist movement. Because of the loss of connection between the scaphoid and lunate, the scaphoid rotates into a degree of flexion leaving the lunate and triquetral free to rotate into extension which causes pain, an inability to weight-bear on the wrist and an overall loss of function (Placzek & Boyce 2006).
Chronic instability of the joint also strongly predisposes to a recognized sequence of osteoarthritis involving the unstable capito-lunate and capitoscaphoid articulations, a sequence known as scapholunate advance collapse (SLAC) (Miller & Schweitzer 2005).
The normal extent of separation between the scaphoid and lunate bones should be less than 2 mm (Gross et al 2002) but a diastasis of more than 3 mm is pathognomonic of scapholunate dissociation and should be detectable on plain X-rays (McRae 1990). The evident space between the bones is known as the Terry Thomas sign , named after the comedian who famously had a gap between his two front teeth.
Using a cadaver model where the wrist was progressively loaded in extension and ulnar deviation, a sequential, four-staged pattern of injury was noted; scapholunate diastasis, dorsal subluxation of the capitate, disruption of the lunotriquetral ligament and complete dislocation of the scapholunate articulation (Brown & Neumann 2004).
**Clinical tip:** It is not always necessary to reproduce subluxation with this test as it is usually painful for the patient and they are likely to indicate apprehension as the forces are gradually applied. The presence of pain and apprehension are good indicators of instability and, as an alternative, detecting increased excursion without causing subluxation can be achieved by applying an anterior/posterior glide to the scaphoid in a neutral position and comparing with the opposite side.
**EXPERT OPINION (★★★):** A tricky test to perform, as well as interpret, but very useful once perfected. Care should be taken when interpreting the findings as up to 30% of healthy wrists can give a false positive result due to general ligamentous laxity at the wrist. It is thought that repeating this dynamically (see variations), particularly when the patient makes a fist, reduces this tendency (Weiss & Finkelstein 2005).
Variations
The
scaphoid stress test
is a simple modification where the patient actively moves the wrist from ulnar to radial deviation while the scaphoid is stabilized by the examiner in the same way. Apprehension and/or a painful clunk during the movement demonstrates dynamic subluxation.
Lunotriquetral Shear Test
Aka: Ballottement test, Reagan’s test, Shuck test
Purpose
To establish the presence of abnormal movement of the lunate and triquetral bones indicating instability or subluxation.
Technique
*
Patient position:
The patient is seated with the forearm supinated and comfortably supported on a table.
*
Clinician position:
Seated facing the patient, the clinician, using a pincer grip, stabilizes the lunate by placing a thumb on its palmar surface and fixes the dorsal surface with the index finger. The other hand grasps the combined bony mass of the pisiform and triquetral using the same pincer grip.
*
Action:
With the lunate stabilized, the examiner moves the triquetral/pisiform in an anteroposterior direction. The test can be reversed by stabilizing the triquetral/pisiform and moving the lunate in the same plane.
*
Positive test:
Excessive mobility of the triquetral in relation to the lunate when compared to the unaffected side is detected along with pain. Crepitus on movement is also sometimes noted.

FIG 4.5: Lunotriquetral shear test.
Clinical context
Differing descriptions for this test can be found in the literature and this has led to the same test being assigned several names. Injury to the lunotriquetral articulation is uncommonly encountered requiring impact in extension and radial deviation (Brown & Neumann 2004). A strain to the lunotriquetral ligament may be evident with localized tenderness and a positive test, but if the trauma has been sufficiently significant to cause disruption of the articulation, normal kinematics will be lost.
The combined unit of the scaphoid and lunate rotate into flexion leaving the untethered triquetral to drift into extension. Pain, apprehension, a reluctance to move and weakness will all be reported by the patient, with a more significant injury likely to predispose to osteoarthritis (Placzek & Boyce 2006). Lunotriquetral ligament injury is often associated with triangular fibrocartilage complex (TFCC) tears and MRI can therefore be helpful in making the distinction (Miller & Schweitzer 2005).
**Clinical tip:** An isolated injury to the lunotriquetral ligament does not usually produce a static diastasis between the lunate and triquetral so there may be dynamic and functional instability present but a normal plain X-ray reported.
**EXPERT OPINION (★★):** It is important to establish what is normal excursion on the unaffected side as differences in range can be subtle.
Related tests
Murphy’s sign
may also indicate the presence of lunate dislocation. The patient is asked to make a fist and the relationship between the heads of the 2nd, 3rd and 4th metacarpals is examined. Normally the head of the 3rd metacarpal extends more distally but where the lunate has dislocated, it remains in line with the heads of the other two metacarpals.
Capitate Apprehension Test
Aka: Capitate displacement test
Purpose
To determine the presence of capitate instability.
Technique
*
Patient position:
The patient sits with the forearm supinated and supported on a table.
*
Clinician position:
Facing the patient, one of the examiner’s thumbs is placed over the palmar aspect of the capitate bone reinforced with the thumb of the other hand. The fingers of both hands are then wrapped around the dorsum of the patient’s hand ensuring the wrist is supported in a neutral position and taking care with the handhold not to involve the patient’s thumb.
*
Action:
The examiner pushes the capitate posteriorly with both thumbs, ensuring the hand is stabilized by the fingers placed around the dorsum of the wrist.
*
Positive test:
Pain and/or apprehension is reproduced as the posterior pressure is applied and this is sometimes accompanied by a click.

FIG 4.6: Capitate apprehension test.
Clinical context
Capitate subluxation is most commonly associated with instability at the scapholunate articulation, usually resulting from a fall on an outstretched hand. Laxity or rupture of the scapholunate ligaments creates a static or dynamic diastasis that leaves the proximal capitate vulnerable to dorsal subluxation, either at the time of the injury or subsequently. In the presence of laxity, the capitate may sublux and reduce recurrently. When subluxed, the capitate can become more prominent and this is best observed on the dorsum of the hand with the wrist in a flexed position. Passive wrist extension will also be painfully blocked particularly when weight-bearing (Atkins et al 2010).
**Clinical tip:** The capitate is located at the base of the 3rd metacarpal and can more easily be palpated on the dorsum of the wrist. There is normally a palpable ‘dip’ over the capitate in the neutral position although this is lost if subluxation has occurred.
**EXPERT OPINION (★★):** Only used when a generalized mid-carpal instability is suspected with a patient complaining of episodic subluxation and pain.
Related tests
The
midcarpal pivot shift test
aims to identify instability as a result of traumatic attenuation of the scapholunate or lunotriquetral ligaments as midcarpal instability is often associated with concurrent injury to these articulations. The patient sits with the elbow at 90° with the supinated forearm supported on a table. The examiner stabilizes the distal forearm with one hand and, supporting the patient’s hand in a neutral position with the other, takes the wrist from a fully radially deviated position into full ulnar deviation. Instead of a normal smooth movement, it is irregular and accompanied by a painful clunk which indicates a positive finding.




FIG 4.7: Midcarpal pivot shift. Start position (A). End position stressing the scapholunate and lunotriquetral articulations (B).
Lichtman’s test is a variation of the midcarpal pivot shift test where axial compression is added to the movement. Pain and/or dorsal movement of the capitate are considered to be positive findings.
**EXPERT OPINION (★) for Lichtman’s Test:** This test can be hard to do well and interpret the findings accurately.
B. TRIANGULAR FIBROCARTILAGE COMPLEX (TFCC) TESTS
TFCC Load Test
Aka: Ulnar meniscal grind test
Purpose
To reproduce pain and/or apprehension indicating a tear or degeneration of the TFCC.
Technique
*
Patient position:
Sitting or standing.
*
Clinician position:
Facing the patient, the examiner stabilizes the patient’s forearm with one hand and, as if shaking hands, places their other hand in the palm where it is held firmly.
*
Action:
Axial compression is then applied through the patient’s hand while ulnar deviation is added. This part of the manoeuvre has been described as the
ulnar impaction test
. This may be enough to reproduce localized pain at the base of the ulna negating the need for further loading. If asymptomatic, stress on the TFCC is increased by ‘scooping’ the hand from flexion to extension while maintaining the ulnar deviation and compression.
*
Positive test:
Localized pain at the ulnar side of the wrist joint is sometimes accompanied by apprehension and/or a click or crepitus on movement.

FIG 4.8: Triangular fibrocartilage complex (TFCC) test.
Clinical context
The TFCC, sometimes referred to as the ulnar articular disc, is a homogeneous structure comprising of the dorsal and palmar radioulnar ligaments, a meniscus, the ulnar collateral ligament and the sheath of the extensor carpi ulnaris (Palmer & Werner 1981). It acts as the primary soft tissue stabilizer of the distal radioulnar joint and takes 20% of the compressive load across the wrist. It is thickest (approx. 5 mm) at its ulnar insertion but thinner (2 mm) and more vulnerable to injury nearer to its radial origin which, unsurprisingly, is the most common site of TFCC tears (Miller & Schweitzer 2005).
The central 80% of the TFCC is avascular and has little potential for repair although its periphery and the dorsal and palmar ligaments are well vascularized, opening the possibility for healing in this zone (Bulstrode et al 2002).
Traumatic lesions (class one) usually involve a compressive force with rotation and/or ulnar deviation. The injury can be masked by associated fractures of the radius and/or ulna. Degenerative/over-use lesions (class two) are found increasingly over the age of 30 and in some cases may progress from simple TFCC ‘wear’ to accompanying lunotriquetral ligament disruption and ulnocarpal arthritis (Bulstrode et al 2002, Miller & Schweitzer 2005).
**Clinical tip:** Clinical features of TFCC lesions include wrist pain accentuated by movement, particularly pronation and ulnar deviation as well as loading of the clenched fist. These findings are usually accompanied by tenderness and crepitus over the TFCC area (Bulstrode et al 2002).
**EXPERT OPINION (★★★):** A very useful test but it can produce false positives and should therefore be taken in conjunction with all other findings.
Related tests
The
supination lift test
requires the patient to sit facing an examination couch with the elbows flexed to 90° and the forearms fully supinated. The couch is positioned at a height that allows the palms of both hands to comfortably make contact with its under-surface. The patient is then asked to attempt to lift the couch up. Localized pain at the base of the ulnar and a reluctance to apply full force are both indicative of a TFCC tear.
C. THUMB TESTS
Axial Compression Test
Aka: Axial grind test, Thumb grind test, Basal joint grind test
Purpose
To detect osteoarthritis (OA) of the trapeziofirstmetacarpal joint (basal joint of the thumb).
Technique
*
Patient position:
The hand rests in a mid-pronated position on a table.
*
Clinician position and action:
The compression test is performed by stabilizing the radial aspect of the wrist with one hand and gripping the first metacarpal shaft with the fingers and thumb of the other. An axial load is applied downwards along the shaft while the metacarpal is gently moved against the trapezium. This has been described as a ‘grind’ technique as the articular surfaces are moved together under compression.
*
Positive test:
A sudden, sharp pain is usually elicited as compression is applied. Occasionally crepitus may also be noted.

FIG 4.9: Axial compression test of the trapeziofirstmetacarpal joint. The arrow indicates the direction of axial compression.
Clinical context
OA of the trapeziofirstmetacarpal joint is the most common site of degenerative joint disease in the hand (Brown & Neumann 2004, Ghavami & Oishi 2006, McRae 1990). The pain is localized around the base of the thumb and typically described as ‘piercing’ and exacerbated by twisting and gripping motions making functional tasks difficult. In the early stages, before changes become detectable on X-ray, the irritated joint capsule may begin to develop capsular restriction causing loss of extension (Atkins et al 2010).
At this stage, in the absence of articular changes, the axial compression test is unlikely to be positive but as the condition worsens, laxity of the supporting ligaments and a reduction of bony constraints leads to increasing joint stress and progressive degenerative disease. Once established, the sensitivity of the test increases but diagnosis is ultimately confirmed by radiology.
Trapeziofirstmetacarpal Osteoarthritis Staging
(Eaton & Glickel 1987)
*
Stage I:
Mild joint narrowing or subchondral sclerosis noted with small effusion. No laxity, subluxation or osteophyte formation.
*
Stage II:
Possible osteophyte formation at the ulnar side of the distal trapezial articular surface. Mild to moderate subluxation might appear.
*
Stage III:
Further joint space narrowing with cystic changes, bone sclerosis and prominent osteophytes. The first metacarpal is moderately subluxed radially and dorsally. Passive reduction might not be possible.
*
Stage IV:
Scaphotrapezial joint also involved with evidence of destruction, with the trapeziofirstmetacarpal joint immobile and usually largely pain-free.
**Clinical tip:** Care needs to be taken when assessing this joint as axial loading can elicit severe twinges of pain, particularly when the condition presents acutely.
**EXPERT OPINION (★★★):** Used regularly as part of the routine clinical examination – especially if X-rays are not available to grade the stage of osteoarthritis.
Finkelstein’s Test
Purpose
To detect pain and limitation caused by inflammation between the tendons of abductor pollicis longus (APL) and extensor pollicis brevis (EPB) and their shared synovial sheath at the distal end of the radius (de Quervain’s tenosynovitis).
Technique
*
Patient position:
With the forearm positioned in pronation, the patient is asked to flex the thumb and close their fingers over it.
*
Clinician position and action:
The lower forearm is fixed with one hand and the patient’s hand taken into ulnar deviation passively with the other.
*
Positive test:
As the wrist is taken towards ulnar deviation, significant pain is reproduced over the radial aspect of the wrist.

FIG 4.10: Finkelstein’s test.
Clinical context
De Quervain’s tenosynovitis involves the two tendons in the first dorsal synovial compartment of the wrist. In the chronic stage where adhesions have developed and the sheath has become thickened, the condition is known as de Quervain’s stenosing tenosynovitis (Atkins et al 2010, Placzek & Boyce 2006). The patient reports localized pain over the dorsum of the distal radius and this is often accompanied by swelling and crepitus on movement. Isometric resisted testing of the affected tendons is painful but repeated active thumb extension more so. The history is usually one of overuse or unaccustomed activity.
The incidence is reported to be considerably higher in the female population, with age also being a significant risk factor and prevalence increasing in the 40+ age group (Wolf et al 2009). The relative excursions of the APL and EPB tendons during Finkelstein’s testing suggest that a positive Finkelstein’s test may result more from EPB pathology than the APL (Kutsumi et al 2005).
**Clinical tip:** Even in the asymptomatic hand this test can be uncomfortable and care should be taken to ensure that the pain is not excessively provoked by an over-vigorous technique, particularly when acutely painful. De Quervain’s tenosynovitis should not be confused with intersection syndrome which involves the same two tendons as they cross over the wrist extensor muscles in the lower forearm about 5 cm proximal from their sheathed extent (Atkins et al 2010) and, because of this, Finkelstein’s test should not be significantly provocative.
**EXPERT OPINION (★★):** This can be approached with too much vigour. A subtle test if done well.
Ulnar Collateral Ligament Laxity Test
Purpose
To detect pain and/or laxity of the ulnar collateral ligament (UCL) of the first metacarpophalangeal (MCP) joint.
Technique
*
Patient position:
Seated with the hand supported on a table in a mid-pronated position.
*
Clinician position:
The examiner stabilizes the distal end of the first metacarpal with the thumb and index finger. The same pincer grip is used with the other hand, placing the fingers over the radial and ulnar aspects of the proximal phalanx.
*
Action:
Fixing the metacarpal, a valgus stress is applied to the joint (which in this position involves the thumb being moved towards the patient).
*
Positive test:
Pain and/or laxity reproduced at the base of the thumb.

FIG 4.11: Valgus stress on the ulnar collateral ligament of the first MCP joint.
Clinical context
Gamekeeper’s thumb (Campbell 1955) is caused by a chronic insufficiency of the UCL at the first MCP joint leading to pain and weakness of the ‘pinch grasp’. Injury to the UCL also presents acutely, most commonly among the skiing population (skier’s thumb), as a result of the ski-pole abruptly stopping in the snow during a fall and the static handle forcing a sudden valgus or abduction stress to the thumb (Davidson & Laliotis 1996, Van Dommelen & Zvirbulis 1989).
When both the ulnar and accessory collateral ligaments are ruptured, a Stener lesion may develop, where the aponeurosis of the adjacent adductor brevis muscle becomes interposed between the ruptured ligament and the phalanx. The ligament retracts, no longer able to make contact with its insertion, and fails to heal (Stener 1962). As an important stabilizer of the thumb the loss of the UCL hampers function considerably and surgical repair is often necessary (Miller & Schweitzer 2005).
**Clinical tip:** With the joint in an extended position, valgus testing primarily determines the competence of the accessory collateral ligament which is taut in this position. Laxity of between 15° and 30° would indicate rupture or partial rupture of the ligament and arouse suspicion of a gamekeeper’s fracture where a portion of the proximal phalanx at the UCL insertion becomes avulsed. A displaced fracture should be eliminated with X-ray before the clinician repeats the valgus test in 30° of flexion, as this position preferentially stresses the UCL and could disturb the fracture site. If gamekeeper’s fracture has been ruled out, an MRI or MR arthrography would be necessary to diagnose a Stener lesion (Harper et al 1996, Spaeth et al 1993).
**EXPERT OPINION (★★★):** In acute injuries this test can determine whether surgical intervention is required. Most surgeons will have a point at which they will repair the ligament (usually around 30–40° of laxity). However, it is a matter of weighing up a number of factors: age, occupation, patient choice, time elapsed since trauma, anaesthetic risk, etc., as this may alter the threshold for surgical repair.
D. CARPAL TUNNEL TESTS
Phalen’s Test
Purpose
To increase pressure on the median nerve as it passes through the carpal tunnel in order to aid diagnosis of carpal tunnel syndrome (CTS).
Technique
*
Patient position:
Seated with the hand resting on a table in mid-pronation.
*
Clinician position:
Seated facing the patient. The affected hand is taken into full wrist flexion. Alternatively, the patient is asked to flex both wrists and oppose the dorsum of the hands so that the flexion is maintained bilaterally.
*
Action:
In either position, the wrist flexion is maintained for a minute.
*
Positive test:
Paraesthesiae is reproduced in the cutaneous distribution of the median nerve (the palmar aspect of the thumb, index and middle fingers and the lateral half of the ring finger) as a result of the sustained narrowing at the carpal tunnel during flexion of the wrist. If severe, pain may also be reproduced.
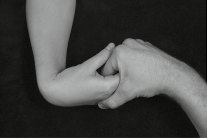



FIG 4.12: Phalen’s test (A) and alternative position (B).
Clinical context
Studies of CTS have generated a great deal of controversy and no universally accepted diagnostic criteria exist (Placzek & Boyce 2006). Phalen’s test was always widely considered to be the most sensitive physical test, but over recent years a number of studies have challenged this and attempted to demonstrate enhanced sensitivity with related or modified tests.
The absence of an agreed ‘gold standard’ of diagnosis requires the clinician to combine a number of clinical findings which can be used to predict the probability of CTS. The ‘CTS 6’ is a validated clinical diagnostic aid which assesses six factors (Graham 2008):
1. Numbness exclusively or predominantly in the median nerve distribution of the hand.
2. Nocturnal numbness.
3. Thenar atrophy or weakness (≤grade 4 on examination).
4. Positive Phalen’s test.
5. Loss of two-point discrimination (failure to distinguish two points 5 mm apart).
6. Positive Tinel’s test.
Table 4.1: Phalen’s Test Validity
| Author and year | LR + | LR - | Target condition |
|---|---|---|---|
| Golding et al 1986 | 0.71 | 1.05 | CTS |
| Gerr & Letz 1998 | 1.3 | 0.8 | CTS |
| Williams et al 1992 | 88 (★★★) | 0.12 (★★) | CTS |
| Tetro et al 1998 | 3.6 (★) | 0.5 (★) | CTS |
**Clinical tip:** Differential diagnosis of hand paraesthesiae/pain should include cervical myelopathy, radiculopathy, adverse neurodynamics involving the lower cervical nerve roots, thoracic outlet syndrome and ulnar nerve entrapment syndromes at the elbow and wrist. Flattening of the thenar eminence muscles may be evident in more chronic cases.
**EXPERT OPINION (★★★):** This is the preferential test for CTS but the clinician should always be aware of the potential of a more proximal source of symptoms requiring further examination of the cervical spine and brachial plexus.
Additional tests
The
prayer test
can also be used to detect CTS. The affected hand is taken into full wrist extension (or together the palms of the hands are opposed and lowered until full extension at both wrists is achieved) and held there for a minute. A ‘decompression phenomenon’ is sometimes observed when pressure on the nerve trunk is removed.

FIG 4.13: Prayer test.
The tourniquet test attempts to exacerbate median neuropathy by inducing temporary ischaemia in the hand. The hand elevation test (Ahn 2001) simply involves elevating the hand for up to a minute to reproduce symptoms. The three jaw chuck test involves opposing the fingers with the thumb and then flexing the wrist maximally.

FIG 4.14: Three jaw chuck test.
Tinel’s Test
Aka: Median nerve percussion test
Purpose
To elicit paraesthesiae and/or pain in the median nerve distribution of the hand in order to aid diagnosis of carpal tunnel syndrome (CTS).
Technique
*
Patient position:
Seated with the hand resting on a table with the forearm fully supinated.
*
Clinician position:
Sitting facing the patient, the affected hand is held in a neutral position.
*
Action:
The mid-point of the carpal tunnel is identified and ‘tapped’ with a finger or a percussion hammer.
*
Positive test:
Temporary paraethesiae or pain in the cutaneous distribution of the median nerve in the hand is reported.

FIG 4.15: Tinel’s test at the carpal tunnel.
Clinical context
Tinel’s test is used in other compressive neuropathies, although it is best known for the detection of CTS. Wide variations in both sensitivity and specificity of the test have been reported. No physical test has been shown to be definitive although a combination of tests, including Tinel’s, was shown to yield reasonable detection rates (Graham 2008).
Table 4.2: Tinel’s Test Validity
| Author and year | LR + | LR - | Target condition |
|---|---|---|---|
| DeKrom et al 1990 | 0.6 | 1.3 | CTS |
| Golding et al 1986 | 1.3 | 0.9 | CTS |
| Gerr & Letz 1998 | 0.67 | 1.1 | CTS |
| Tetro et al 1998 | 8.2 (★★) | 0.3 (★) | CTS |
| Williams et al 1992 | 67 (★★★) | 0.3 (★) | CTS |
**Clinical tip:** Tinel’s test can also be used to detect the extent of regeneration of the sensory fibres of the median nerve where the most distal point of abnormal sensation represents the distal extent of the regeneration. The clinician commences tapping at the tip of the palmar surface of the index finger and moves proximally towards the mid-point of the carpal tunnel.
**EXPERT OPINION (★★):** Used mainly to determine continued potential for nerve recovery post op/trauma rather than actual diagnosis of the condition.
Related tests
Although less common,
ulnar tunnel syndrome
results from compression of the ulnar nerve as it passes through Guyon’s canal. It is usually caused by sustained compression (e.g. positioning the ulnar border of the hand on the handlebars when cycling with the wrist in extension and radial deviation). Tinel’s test can be repeated, tapping distally from the pisiform.

FIG 4.16: Tinel’s test at the ulnar tunnel.
Carpal Compression Test
Aka: Pressure provocative test, Manual carpal compression test, Durkan’s compression test
Purpose
To increase pressure on the median nerve as it passes through the carpal tunnel in order to aid diagnosis of carpal tunnel syndrome (CTS).
Technique
*
Patient position:
Seated with the forearm supinated with the hand rested on a table.
*
Clinician position and action:
Sitting facing the patient, the examiner places one thumb, superimposed with the other, over the mid-point of the flexor retinaculum and presses firmly downwards for up to a minute while maintaining counterpressure with the fingers on the dorsum of the hand.
*
Positive test:
Paraesthesiae are reproduced in the cutaneous distribution of the median nerve and if the condition is severe, pain may also be evoked.

FIG 4.17: Carpal compression test.
Clinical context
The carpal compression test has been shown to be more sensitive than both Phalen’s and Tinel’s tests, with symptoms often reproducible within several seconds, suggesting that it is a simple, fast and valuable provocative test for CTS (González et al 1997). In an attempt to standardize the amount of pressure required to consistently reproduce the symptoms, the use of an instrumented carpal compression device was tested and shown to deliver a similar degree of sensitivity and specificity (Durkan 1994).
Table 4.3: Carpal Compression Test Validity
| Author and year | LR + | LR - | Target condition |
|---|---|---|---|
| Gonzalez et al 1997 | 7.9 (★★) | 0.15 (★★) | CTS |
| Durkan 1994 | 22.3 (★★★) | 0.11 (★★) | CTS |
| Tetro et al 1998 | 10.7 (★★★) | 0.27 (★) | CTS |
| Williams et al 1992 | 33 (★★★) | 0.01 (★★★) | CTS |
**Clinical tip:** This test is also usefully employed where there is limited range of flexion or pain at the wrist which prevents an effective Phalen’s test from being performed. Accurate localization of the median nerve in the carpal tunnel is necessary for effective testing. The distal wrist crease is level with the proximal border of the flexor retinaculum so pressure needs to be distal to this line and centrally.
Variations
The test can be further modified by either adding passive wrist extension (while asking the patient to grip) or passive wrist flexion (Fertl et al 1998, Tetro et al 1998). The latter has been found to have an optimal cut-off time of just 20 seconds.
Table 4.4: Carpal Compression Test with Flexion/Extension
| Author and year | LR + | LR - | Target condition |
|---|---|---|---|
| Tetro et al 1998 | 82 (★★★) | 0.18 (★★) | CTS |
Scientific References
- Ahn, D.S., 2001. Hand elevation: a new test for carpal tunnel syndrome. Ann. Plast. Surg. 46 (2), 120–124.
- Atkins, E., Kerr, E., Goodlad, J., 2010. A Practical Approach to Orthopaedic Medicine , third ed. Churchill Livingstone, Edinburgh.
- Brown, D.E., Neumann, R.D., 2004. Orthopaedic Secrets , third ed. Hanley & Belfus, Philadelphia.
- Bulstrode, C., Buckwalter, J., Carr, A., et al., 2002. Oxford Textbook of Orthopaedics and Trauma . Oxford University Press, Oxford.
- Campbell, C.S., 1955. Gamekeeper’s thumb. J. Bone Joint Surg. Br. 37 (1), 148–149.
- Davidson, T.M., Laliotis, A.T., 1996. Snowboarding injuries, a four-year study with comparison with alpine ski injuries. West. J. Med. 164 (3), 231–237.
- DeKrom, M.C., Knipschild, P.G., Kester, A.D., 1990. Efficacy of provocative tests for diagnosis of carpal tunnel syndrome. Lancet 335 (8686), 393–395.
- Durkan, J.A., 1994. The carpal-compression test: an instrumented device for diagnosing carpal tunnel syndrome. Orthop. Rev. 23 (6), 522–525.
- Eaton, R.G., Glickel, S.Z., 1987. Trapeziometacarpal osteoarthritis: staging as a rationale for treatment. Hand Clin. 3 (4), 455–471.
- Fertl, E., Wober, C., Zeitlhofer, J., 1998. The serial use of two provocative tests in the clinical diagnosis of carpal tunnel syndrome. Acta Neurol. Scand. 98 (5), 328–332.
- Gerr, F., Letz, R., 1998. The sensitivity and specificity of tests for carpal tunnel syndrome vary with the comparison subjects. J. Hand Surg. Br. 23 (2), 151–155.
- Ghavami, A., Oishi, S.N., 2006. Thumb trapeziometacarpal arthritis: treatment with ligament reconstruction tendon interposition arthroplasty. Plast. Reconstr. Surg. 117 (6), 116e–128e.
- Golding, D.N., Rose, D.M., Selvarajah, K., 1986. Clinical tests for carpal tunnel syndrome: an evaluation. Br. J. Rheumatol. 25 (4), 388–390.
- González del Pino, J., Delgado-Martínez, A.D., González González, I., et al., 1997. Value of the carpal compression test in the diagnosis of carpal tunnel syndrome. J. Hand Surg. Br. 22 (1), 38–41.
- Graham, B., 2008. The value added by electrodiagnostic testing in the diagnosis of carpal tunnel syndrome. J. Bone Joint Surg. Am. 90 (12), 2587–2593.
- Gross, J., Fetto, J., Rosen, E., 2002. Musculoskeletal Examination , second ed. Wiley-Blackwell, Chichester.
- Harper, M.T., Chandnani, V.P., Spaeth, J., et al., 1996. Gamekeeper thumb: diagnosis of ulnar collateral ligament injury using magnetic resonance imaging, magnetic resonance arthrography and stress radiography. J. Magn. Reson. Imaging 6 (2), 322–328.
- Heller, L., Ring, H., Costeff, H., et al., 1986. Evaluation of Tinel’s and Phalen’s signs in diagnosis of the carpal tunnel syndrome. Eur. Neurol. 25 (1), 40–42.
- Heyman, P., 1997. Injuries to the ulnar collateral ligament of the thumb metacarpophalangeal joint. J. Am. Acad. Orthop. Surg. 5 (4), 224–229.
- Jordan, R., Carter, T., Cummins, C., 2002. A systematic review of the utility of electrodiagnostic testing in carpal tunnel syndrome. Br. J. Gen. Pract. 52 (481), 670–673.
- Katz, J.N., Larson, M.G., Sabra, A., et al., 1990. The carpal tunnel syndrome: diagnostic utility of the history and physical examination findings. Ann. Intern. Med. 112 (5), 321–327.
- Kutsumi, K., Amadio, P.C., Zhao, C., et al., 2005. Finkelstein’s test: a biomechanical analysis. J. Hand Surg. Am. 30 (1), 130–135.
- Lo, J.K., Finestone, H.M., lbert, K., et al., 2002. Community-based referrals for electrodiagnostic studies in patients with possible carpal tunnel syndrome: what is the diagnosis? Arch. Phys. Med. Rehabil. 83 (5), 598–603.
- McRae, R., 1990. Clinical Orthopaedic Examination , third ed. Churchill Livingstone, London.
- Magee, D.J., 2008. Orthopaedic Physical Assessment , fifth ed. Saunders, Philadelphia.
- Malanga, G.A., Nadler, S., 2006. Musculoskeletal Physical Examination: An Evidence-Based Approach . Elsevier Health Sciences, Philadelphia.
- Miller, T.T., Schweitzer, M.E., 2005. Diagnostic Musculoskeletal Imaging . McGraw-Hill, New York.
- Palmer, A.K., Werner, F.W., 1981. The triangular fibrocartilage complex of the wrist – anatomy and function. J. Hand Surg. Am. 6 (2), 153–162.
- Placzek, J.D., Boyce, D.A., 2006. Orthopaedic Physical Therapy Secrets , second ed. Elsevier Health Sciences, Missouri.
- Rivner, M.H., 1994. Statistical errors and their effect on electrodiagnostic medicine. Muscle Nerve 17 (7), 811–814.
- Seror, P., 1987. Tinel’s sign in the diagnosis of carpal tunnel syndrome. J. Hand Surg. Br. 12 (3), 364–365.
- Spaeth, H.J., Abrams, R.A., Bock, G.W., et al., 1993. Gamekeeper thumb: differentiation of nondisplaced and displaced tears of the ulnar collateral ligament with MR imaging: work in progress. Radiology 188 (2), 553–556.
- Stener, B., 1962. Displacement of the ruptured ulnar collateral ligament of the metacarpo-phalangeal joint of the thumb. J. Bone Joint Surg. Br. 44, 869–879.
- Szabo, R.M., Slater, R.R., Farver, T.B., et al., 1999. The value of diagnostic testing in carpal tunnel syndrome. J. Hand Surg. Am. 24 (4), 704–714.
- Tetro, A.M., Evanoff, B.A., Hollstien, S.B., et al., 1998. A new provocative test for carpal tunnel syndrome: assessment of wrist flexion and nerve compression. J. Bone Joint Surg. Br. 80 (3), 493–498.
- Van Dommelen, B.A., Zvirbulis, R.A., 1989. Upper extremity injuries in snow skiers. Am. J. Sports Med. 17 (6), 751–753.
- Weiss, S., Finkelstein, N., 2005. Hand Rehabilitation – A Quick Reference Guide and Review , second ed. Elsevier Mosby, St Louis.
- Williams, T.M., Mackinnon, S.E., Novak, C.B., et al., 1992. Verification of the pressure provocative test in carpal tunnel syndrome. Ann. Plast. Surg. 29 (1), 8–11.
- Wolf, J.M., Sturdivant, R.X., Owens, B.D., 2009. Incidence of de Quervain’s tenosynovitis in a young, active population. J. Hand Surg. Am. 34 (1), 112–115.
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding wrist-and-hand