Mastering Shoulder Anatomy: An Intraoperative Surgical Approach & Pearls

Key Takeaway
This masterclass guides orthopaedic fellows through a comprehensive shoulder surgical approach, emphasizing critical anatomy. We'll detail neurovascular risks, muscular intervals, and precise instrument use from incision to hardware application. Learn to navigate the complex shoulder girdle, understand glenohumeral stability, and manage potential pitfalls for optimal patient outcomes. This immersive session ensures a deep understanding of shoulder and elbow surgical principles.
Welcome, fellows, to the operating theater. Today, we are embarking on a profound journey into the intricate and unforgiving world of shoulder and elbow anatomy. We will examine these structures not merely from the static, idealized perspective of a textbook, but from the dynamic, real-time, intraoperative vantage point that dictates surgical success or failure. Our overarching goal is to translate theoretical anatomical knowledge into practical, reproducible surgical skill, emphasizing precision, patient safety, and an unwavering respect for the complex neurovascular and musculotendinous structures that afford the upper extremity its incredible range of motion.
Remember, the fundamental art of any orthopedic surgery lies in the meticulous reconstruction of diseased or injured tissues with the absolute minimum of iatrogenic destruction. Skillful, atraumatic handling of the soft tissues is the definitive hallmark of all master upper extremity surgeons. The upper extremity functions primarily as a highly evolved kinematic chain designed to position and move the hand in a three-dimensional spatial envelope. Its attachment to the axial skeleton is astonishingly tenuous, occurring solely through the sternoclavicular joint, with the entirety of the appendicular mass suspended by a delicate, finely tuned balance of soft tissues. This anatomical arrangement provides unparalleled mobility, but at the steep cost of inherent instability, particularly at the glenohumeral joint. The elbow, in stark contrast, offers intrinsic osseous stability, primarily functioning as a hinge to adjust the functional length of the limb. There is no distinct physiological demarcation between the shoulder and elbow regions; pathological pain can refer from the cervical spine or shoulder down the arm, dictating that a thorough, comprehensive physical examination from the neck to the digits is always paramount before any surgical intervention is considered.
Comprehensive Introduction and Patho-Epidemiology
The glenohumeral joint represents a fascinating evolutionary compromise, sacrificing intrinsic osseous constraint for a maximized global arc of motion. Unlike the hip, which relies on deep acetabular coverage for stability, the shoulder depends almost entirely on a complex interplay of static capsuloligamentous restraints and dynamic muscular force couples. When this delicate equilibrium is disrupted—whether by acute high-energy trauma, repetitive microtrauma, or insidious degenerative processes—the resultant pathology often necessitates surgical intervention. Understanding the epidemiology of these conditions is critical for the practicing orthopedic surgeon, as it informs our diagnostic algorithms and surgical planning. Rotator cuff disease, for instance, exists on a continuum from mild tendinopathy to massive, irreparable tears, with prevalence increasing exponentially with advancing age. By the seventh decade of life, a significant percentage of the population harbors asymptomatic rotator cuff defects, highlighting the necessity of correlating advanced imaging findings with meticulous clinical examinations.
Glenohumeral instability is another primary driver of surgical volume, particularly in the young, athletic demographic. Anterior dislocations account for the vast majority of these events, frequently resulting in classic Bankart lesions—avulsions of the anteroinferior capsulolabral complex—and associated Hill-Sachs impaction fractures of the posterosuperior humeral head. The patho-epidemiology of instability dictates that younger patients face a dramatically higher recurrence rate following conservative management, often exceeding eighty percent in patients under twenty years of age, thereby lowering the threshold for early surgical stabilization. Conversely, older patients sustaining primary dislocations are at a significantly heightened risk for concurrent rotator cuff tears, a devastating "terrible triad" of the shoulder that requires a high index of suspicion and prompt surgical management.
Furthermore, the incidence of primary glenohumeral osteoarthritis and rotator cuff tear arthropathy is rising in tandem with the aging global population. The progressive destruction of articular cartilage, coupled with the loss of the dynamic superior restraint normally provided by an intact supraspinatus, leads to proximal humeral migration, articulation with the coracoacromial arch, and profound functional debilitation. The surgical management of these end-stage arthropathies has been revolutionized by the advent of anatomic and reverse total shoulder arthroplasty. However, the success of these arthroplasty procedures remains inextricably linked to the surgeon's mastery of the underlying anatomy, their ability to achieve precise implant positioning, and their capacity to meticulously balance the remaining soft tissue envelope.
Detailed Surgical Anatomy and Biomechanics
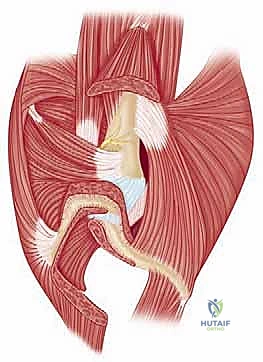
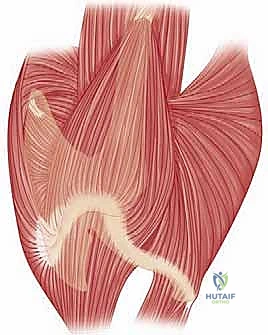
A profound, three-dimensional understanding of shoulder anatomy is the absolute prerequisite for surgical mastery. The shoulder girdle is not a single articulation, but rather a complex interplay of four distinct joints: the glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic articulations. The scapula serves as the foundational platform for this system. It is a thin, flat bone, significantly thickened at its superior and inferior angles, and along its lateral border, where powerful dynamic stabilizers attach. The posterior surface of the scapula is divided by the prominent scapular spine, creating the supraspinatus and infraspinatus fossae, which house the correspondingly named rotator cuff muscles. Blood supply to the scapula is robust, deriving from vessels within the muscles that take fleshy origin from its surfaces, creating a rich anastomotic network that facilitates rapid osseous healing following fractures.

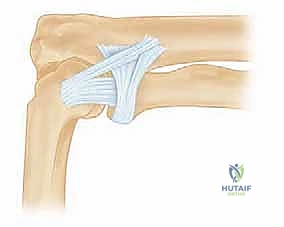
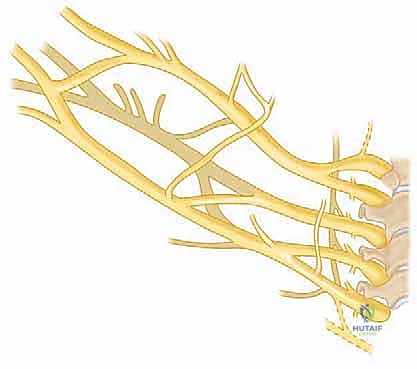
Deep within the anterior surgical field, the coracoid process emerges as a critical, lighthouse-like landmark. Arising from the upper base of the glenoid neck, it projects anteriorly before hooking laterally. This robust osseous process serves as the origin for the short head of the biceps and the coracobrachialis (the conjoint tendon), and as the insertion site for the pectoralis minor. Furthermore, it is the crucial anchor point for the coracoacromial, coracohumeral, and coracoclavicular ligaments. The clavicle, acting as the sole osseous strut connecting the upper extremity to the thorax, exhibits a relatively straight anterior profile but possesses a distinct italic S-shape in the transverse plane. This complex morphology is critical to understand when evaluating fracture patterns or contouring fixation plates. Posterior to the medial third of the clavicle lie the vital subclavian vessels and the cords of the brachial plexus, demanding extreme caution during dissection in this region.
The glenohumeral joint itself is stabilized by a complex array of capsuloligamentous structures. The Rotator Interval, a triangular space between the supraspinatus and subscapularis tendons, contains the coracohumeral ligament and the superior glenohumeral ligament (SGHL). The SGHL arises near the origin of the long head of the biceps and inserts superior to the lesser tuberosity. The Middle Glenohumeral Ligament (MGHL) is highly variable, originating inferior to the SGHL and inserting medial to the lesser tuberosity. The Inferior Glenohumeral Ligament (IGHL) complex is the most critical static stabilizer against anterior and posterior translation. Comprising an anterior band, a posterior band, and an interposed axillary pouch, the IGHL functions like a hammock. With the arm in abduction and external rotation, the anterior band becomes taut, preventing anterior subluxation; conversely, internal rotation tension the posterior band.

Biomechanically, the shoulder relies on exquisite force couples to maintain the humeral head centered within the shallow glenoid vault. In the coronal plane, the inferiorly directed pull of the inferior rotator cuff (infraspinatus, teres minor, subscapularis) precisely counteracts the superiorly directed sheer force generated by the deltoid during early abduction. In the transverse plane, the anterior subscapularis balances the posterior infraspinatus and teres minor. Disruption of these force couples, typically through massive rotator cuff tears, leads to superior humeral migration, altered kinematics, and accelerated joint destruction. Understanding these dynamic relationships is essential not only for executing repairs but also for designing rehabilitation protocols that restore functional balance without overloading healing tissues.


Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in the shoulder must be predicated on a rigorous evaluation of the patient's pathology, physiological age, functional demands, and medical comorbidities. Surgical indications are rarely absolute; they exist on a spectrum that requires nuanced clinical judgment. For instance, while a displaced, multi-part proximal humerus fracture in a young, active patient is a clear indication for open reduction and internal fixation (ORIF), the identical fracture pattern in a low-demand octogenarian with severe osteoporosis may be more appropriately managed with a reverse total shoulder arthroplasty (RTSA) or even non-operative functional bracing. The surgeon must weigh the biological healing capacity of the patient against the mechanical requirements of the proposed construct.
In the realm of degenerative joint disease, primary osteoarthritis with an intact rotator cuff and concentric glenoid wear is the classic indication for anatomic total shoulder arthroplasty (aTSA). However, if the patient presents with rotator cuff tear arthropathy—characterized by massive, irreparable cuff tearing, superior humeral migration, and acetabularization of the coracoacromial arch—aTSA is strictly contraindicated due to the inevitability of early glenoid component loosening (the "rocking horse" phenomenon). In these scenarios, the RTSA is indicated, as it medializes and distalizes the center of rotation, recruiting the deltoid to compensate for the deficient rotator cuff.
Contraindications must be respected to avoid catastrophic outcomes. Active, untreated infection within the joint or surrounding soft tissues is an absolute contraindication to any elective arthroplasty or hardware implantation. Neuropathic joints (Charcot arthropathy) represent a severe relative, if not absolute, contraindication due to the exceptionally high rates of hardware failure and instability. Furthermore, a non-functioning deltoid muscle—often secondary to a severe axillary nerve palsy—precludes the use of a reverse total shoulder arthroplasty, as the deltoid is the primary motor unit required for elevation in this biomechanical construct.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anatomic Total Shoulder Arthroplasty (aTSA) | Primary osteoarthritis; Intact rotator cuff; Concentric glenoid wear; Rheumatoid arthritis. | Active joint infection; Neuropathic joint; Absent/paralyzed deltoid; Massive, irreparable rotator cuff tear. | Severe glenoid bone loss (B2/C/D glenoids without grafting); Parkinson's disease. |
| Reverse Total Shoulder Arthroplasty (RTSA) | Rotator cuff tear arthropathy; Pseudoparalysis; Revision arthroplasty; Complex proximal humerus fractures in the elderly. | Active joint infection; Absent/paralyzed deltoid muscle; Functionally debilitating axillary nerve palsy. | Extreme glenoid bone loss precluding baseplate fixation; Severe cognitive impairment. |
| Open Reduction Internal Fixation (ORIF) | Displaced 2-, 3-, or 4-part proximal humerus fractures in physiologically young patients; Head-splitting fractures. | Active infection; Medically unstable patient; Severe, uncorrectable coagulopathy. | Severe osteoporosis precluding screw purchase; Highly comminuted fractures in the elderly. |
| Open Bankart / Latarjet Procedure | Recurrent anterior instability with significant bipolar bone loss (>15-20% glenoid loss); Failed arthroscopic stabilization. | Active infection; Medically unfit for surgery; Voluntary, multidirectional instability without structural lesions. | Seizure disorders (until medically controlled); Non-compliant patients. |
Pre-Operative Planning, Templating, and Patient Positioning
Before a scalpel ever touches the skin, meticulous preoperative planning is absolutely non-negotiable. This phase is not merely about identifying the gross pathology; it is an intellectual exercise in anticipating every conceivable anatomical challenge, selecting the optimal surgical approach, and ensuring the immediate availability of all necessary instrumentation and salvage equipment. We begin with a rigorous review of the patient's imaging modalities. Standard plain radiographs (true AP, axillary lateral, and scapular Y views) are mandatory. For complex fractures, severe glenoid deformity, or any planned arthroplasty, a non-contrast Computed Tomography (CT) scan is essential. 3D CT reconstructions allow for the precise evaluation of glenoid version, inclination, and volumetric bone loss, which are critical for accurate component positioning.
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating the soft tissue envelope. We must meticulously assess the rotator cuff tendons for retraction and the muscle bellies for fatty infiltration, utilizing the Goutallier classification system. High-grade fatty infiltration (Goutallier stage 3 or 4) indicates irreversible muscle degeneration, which significantly impacts the prognosis of a primary repair and may alter the surgical plan toward a superior capsular reconstruction, tendon transfer, or arthroplasty. Furthermore, we must pay close attention to the acromion morphology, as originally described by Bigliani and Morrison.


A Type 1 acromion, with its flat undersurface, offers the least compromise to the supraspinatus outlet. A Type 2 is curved, while a Type 3 acromion, characterized by a distinct anterior hook, is strongly associated with extrinsic mechanical impingement and full-thickness rotator cuff pathology. Understanding these osseous variations guides our intraoperative approach, particularly when determining the necessity and extent of an acromioplasty. Once the imaging is reviewed, we utilize digital templating software to size our hardware, whether it is a proximal humeral locking plate, an intramedullary nail, or the components for a total shoulder arthroplasty. We template for the ideal fit, but always ensure that sizes immediately above and below our templated plan are sterilized and available in the room.
Patient positioning is the foundation of a successful operation. For the vast majority of open shoulder procedures, including arthroplasty and fracture fixation, we favor the beach chair position. This orientation provides excellent, unhindered access to the anterior, superior, and often posterior aspects of the shoulder girdle. The patient's torso is typically elevated to an angle of 30 to 45 degrees. The head must be securely supported in a specialized headrest, positioned in neutral alignment or slightly flexed and rotated away from the operative side to avoid any traction injury to the brachial plexus. All pressure points—including the occiput, sacrum, and heels—must be meticulously padded to prevent pressure necrosis or peripheral nerve compression. The operative arm is draped free, allowing the surgeon full, unrestricted manipulation for range of motion assessment and fracture reduction maneuvers. Crucially, the fluoroscopic C-arm must be positioned and tested to ensure it can obtain orthogonal views (AP and axillary) without requiring repositioning of the patient. This must be confirmed prior to sterile draping.
Step-by-Step Surgical Approach and Fixation Technique
The deltopectoral approach remains the undisputed workhorse for open shoulder surgery, providing unparalleled, extensile access to the anterior glenohumeral joint, the proximal humerus, and the coracoid process. It is an internervous plane, exploiting the boundary between the deltoid (innervated by the axillary nerve) and the pectoralis major (innervated by the medial and lateral pectoral nerves), thereby minimizing the risk of denervation to the primary dynamic stabilizers. The procedure begins with a curvilinear skin incision, starting just lateral to the tip of the coracoid process and extending distally and laterally along the deltopectoral groove toward the deltoid insertion.
Following the skin incision, the subcutaneous tissues are sharply divided, and meticulous hemostasis is achieved with electrocautery. The surgeon must immediately identify the cephalic vein, which serves as the primary landmark for the deltopectoral interval. The management of the cephalic vein is a topic of historical debate; however, the contemporary consensus favors preserving the vein and retracting it laterally with the deltoid muscle. This lateral retraction preserves the vein's primary venous tributaries, which predominantly arise from the deltoid, thereby reducing the risk of postoperative venous congestion and thrombosis. Once the interval is developed, blunt dissection with a finger or a sponge stick is utilized to separate the deltoid from the pectoralis major.

Deep to this superficial muscular layer, the clavipectoral fascia is encountered. This thin fascial layer must be incised longitudinally, lateral to the conjoint tendon, to expose the deeper structures of the anterior shoulder. The conjoint tendon (short head of the biceps and coracobrachialis) is identified and gently retracted medially. It is imperative to avoid aggressive medial retraction of the conjoint tendon, as this places profound traction on the musculocutaneous nerve, which typically enters the coracobrachialis approximately 5 to 8 centimeters distal to the coracoid tip. With the conjoint tendon retracted medially and the deltoid retracted laterally, the subscapularis tendon and the underlying lesser tuberosity are brought into full view.
To access the glenohumeral joint, the subscapularis must be mobilized. Depending on the specific procedure and surgeon preference, this can be achieved via a subscapularis tenotomy, a subscapularis peel off the lesser tuberosity, or a lesser tuberosity osteotomy (LTO). An LTO provides excellent bone-to-bone healing upon closure and is particularly favored in anatomic total shoulder arthroplasty. Once the subscapularis is reflected, an anterior capsulotomy is performed, exposing the articular surface of the humeral head and the glenoid vault. At this stage, the humeral head can be dislocated anteriorly by externally rotating and extending the arm, providing comprehensive access for fracture reduction, joint debridement, or the preparation of osseous surfaces for arthroplasty components.

Complications, Incidence Rates, and Salvage Management
Despite meticulous technique and exhaustive preoperative planning, complications in open shoulder surgery remain a persistent reality. The complex, condensed neurovascular anatomy of the axilla and shoulder girdle renders these structures highly vulnerable to iatrogenic injury. Neurologic complications are among the most devastating. The axillary nerve, coursing inferior to the glenoid capsule through the quadrangular space, is at significant risk during inferior capsular releases or when placing retractors on the inferior glenoid neck. Similarly, the musculocutaneous nerve is highly susceptible to traction injury if the conjoint tendon is aggressively retracted medially during the deltopectoral approach.

Infection, while relatively uncommon in primary shoulder surgery (typically occurring in less than 1-2% of cases), presents a monumental challenge, particularly in the presence of arthroplasty implants or massive hardware constructs. Cutibacterium acnes (C. acnes), an indolent, slow-growing anaerobic bacterium resident deep within the dermal sebaceous glands of the shoulder, is a frequent culprit. Its indolent nature often leads to delayed presentations, characterized by vague pain and stiffness rather than overt signs of acute sepsis. Management of deep infections frequently necessitates multiple staged surgeries, including radical debridement, implant removal, placement of antibiotic-impregnated spacers, and prolonged courses of targeted intravenous antibiotics.
Mechanical failures and instability are also significant concerns. Following anatomic total shoulder arthroplasty, subscapularis failure is a recognized complication that can lead to devastating anterior instability and catastrophic failure of the joint construct. This highlights the absolute necessity of a robust, secure repair of the subscapularis tendon or lesser tuberosity osteotomy during the closure phase of the procedure. Postoperative stiffness, or secondary adhesive capsulitis, is a frequent complication following both fracture fixation and soft tissue repairs. While often self-limiting, severe stiffness may require aggressive physical therapy, manipulation under anesthesia, or arthroscopic capsular release.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage Management & Avoidance Strategy |
|---|---|---|---|
| Axillary Nerve Injury | 1% - 4% | Inferior capsular release; Retractor placement on inferior glenoid neck; Plating of proximal humerus. | Avoid blind inferior dissection; Place retractors carefully; Consider nerve exploration/grafting if no recovery by 3-6 months. |
| Musculocutaneous Nerve Palsy | 1% - 3% | Aggressive medial retraction of the conjoint tendon during deltopectoral approach. | Limit medial retraction tension; Release proximal conjoint fascia if necessary; Observation (most are transient neuropraxias). |
| Deep Joint Infection (C. acnes) | 1% - 2.5% | Arthroplasty procedures; Male gender; Prior shoulder surgery; Inadequate skin preparation. | Meticulous skin prep (Chlorhexidine/alcohol); Benzoyl peroxide pre-treatment; Staged revision with antibiotic spacer for established infections. |
| Subscapularis Failure | 2% - 7% (Post-aTSA) | Poor tissue quality; Over-aggressive early external rotation rehab; Inadequate surgical repair. | Utilize Lesser Tuberosity Osteotomy (LTO) for bone-to-bone healing; Strict adherence to post-op ROM limits; Revision repair or conversion to RTSA. |
| Postoperative Stiffness | 5% - 15% | Prolonged immobilization; Non-compliance with rehab; Biologic predisposition. | Early, controlled passive ROM; Judicious use of NSAIDs; Arthroscopic capsular release if refractory after 6-9 months of therapy. |
Phased Post-Operative Rehabilitation Protocols
The surgical intervention itself represents only the first phase of the patient's recovery journey; the ultimate functional outcome is heavily dictated by the execution
