Fragment-Specific Fixation of Distal Radius Fractures: An Intraoperative Masterclass

Key Takeaway
This masterclass provides a granular, real-time guide to fragment-specific fixation of distal radius fractures. We meticulously cover comprehensive anatomy, preoperative planning, precise intraoperative execution from incision to hardware placement, and critical pearls to avoid pitfalls. Fellows will gain a deep understanding of restoring articular congruity and stability for optimal patient outcomes and immediate motion.
Comprehensive Introduction and Patho-Epidemiology
Evolution of the Fragment-Specific Philosophy
The surgical management of distal radius fractures has undergone a profound evolution over the past three decades, shifting from closed reduction and cast immobilization to sophisticated, anatomically precise internal fixation strategies. Historically, the advent of the volar locking plate (VLP) revolutionized the treatment of these injuries, providing a reliable, fixed-angle construct that mitigated the high complication rates associated with dorsal plating and external fixation. The VLP functioned primarily as an internal fixator, utilizing subchondral locking screws to raft the articular surface and resist the forces of axial impaction. This monolithic approach successfully addressed the majority of extra-articular and simple intra-articular fracture patterns, establishing a new gold standard in orthopedic trauma care.
However, as our understanding of complex intra-articular fracture kinematics matured, it became glaringly evident that a monolithic volar plate is not a universal panacea. Highly comminuted, multi-fragmentary articular fractures—particularly those involving independent volar marginal shearing, dorsal wall blowouts, or isolated radial styloid dissociation—often escape the capture of standard fixed-angle locking screws. The fixed trajectory of these screws, while excellent for rafting a relatively intact subchondral plate, fails to provide targeted, orthogonal compression to small, discrete articular fragments. This realization birthed the philosophy of fragment-specific fixation (FSF), a paradigm shift from simply "plating the bone" to meticulously "reconstructing the joint."
Fragment-specific fixation is not merely a surgical technique; it is a comprehensive treatment algorithm predicated on identifying, reducing, and independently stabilizing each discrete component of the fracture. By utilizing an array of low-profile, modular implants designed with specific biomechanical properties—such as spring-like elasticity for dynamic load sharing, wire forms for subchondral capture, or rigid mini-plates for shear force buttressing—the surgeon can create a customized, multiplanar construct. This modularity allows for the anatomical restoration of the articular surface while providing sufficient biomechanical stability to permit immediate, early active motion. The ultimate objective is to neutralize the specific deforming forces acting on each fracture fragment, thereby restoring the intricate spatial relationship between the radiocarpal and distal radioulnar joints.

Epidemiological Considerations and Injury Mechanisms
Distal radius fractures represent one of the most ubiquitous orthopedic injuries, accounting for approximately one-sixth of all fractures evaluated in emergency departments worldwide. The epidemiological profile of these fractures exhibits a classic bimodal distribution, reflecting distinct injury mechanisms and patient demographics that dictate the "personality" of the fracture. The first peak occurs in younger, predominantly male populations, typically resulting from high-energy trauma such as motor vehicle collisions, falls from significant heights, or extreme sports. These high-energy injuries impart immense axial and shear forces across the radiocarpal joint, shattering the subchondral plate and creating complex, multi-part fracture patterns.
These high-energy mechanisms are characterized by extensive articular comminution, severe soft tissue compromise, and a high propensity for concomitant carpal ligamentous disruptions or distal radioulnar joint (DRUJ) instability. The explosive nature of the impact often results in coronal plane splits, dorsal wall blowouts, and the creation of free intra-articular osteochondral fragments. Standard fixed-angle plating is frequently inadequate in these scenarios, as the fracture lacks the metaphyseal stability required to support a single implant. Consequently, these high-energy injuries necessitate the highly tailored, multi-incisional approach of fragment-specific fixation to capture and buttress each independent structural column.
Conversely, the second epidemiological peak is observed in the elderly population, predominantly post-menopausal females, secondary to low-energy falls from a standing height. In this demographic, osteopenia and osteoporosis play a critical role in the pathogenesis of the fracture. The diminished trabecular bone density within the distal radial metaphysis creates a structural void, predisposing the bone to severe impaction and dorsal or volar bending failure. While many osteoporotic fractures can be managed with standard volar locking plates, the presence of severe metaphyseal comminution, extreme osteopenia, or diminutive articular fragments often renders standard screw purchase inadequate. In these fragile osteoporotic variants, fragment-specific implants, such as wire forms or low-profile buttress pins, can be utilized to capture small, osteopenic articular fragments that would otherwise displace, ensuring maintenance of the articular reduction until osseous union is achieved.

Biomechanical Rationale for Modular Fixation
The biomechanical superiority of fragment-specific fixation lies in its ability to address the unique vector of displacement for each fracture fragment. Traditional plates rely on the friction between the plate and the bone, or the fixed-angle stability of locking screws, to resist displacement. However, in the setting of severe comminution, the load-sharing capacity of the bone is lost, and the implant must bear the entirety of the physiological load. A single, monolithic plate placed on the volar aspect of the radius is biomechanically disadvantaged when attempting to resist dorsal bending forces or stabilize a completely dissociated radial styloid.
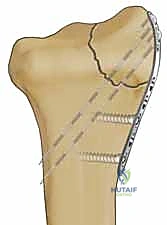
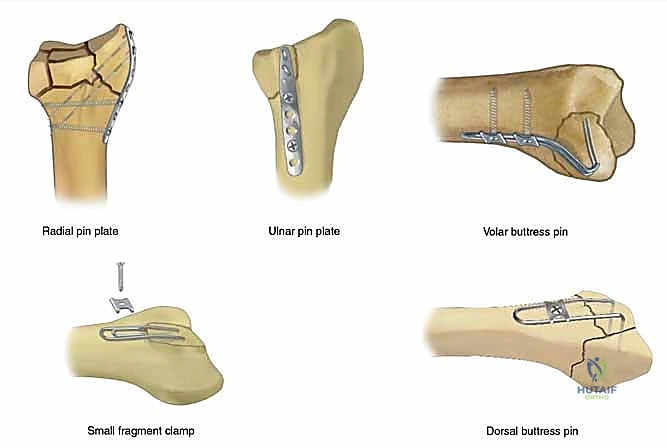
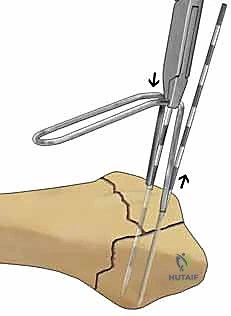
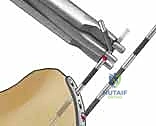
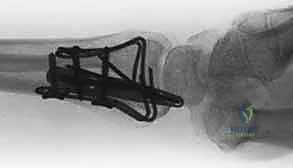
Modular fixation systems distribute the biomechanical load across multiple, low-profile implants strategically placed along the anatomical columns of the radius. By applying a dedicated pin-plate to the radial styloid, a hook plate to the volar lunate facet, and a buttress plate to the dorsal wall, the surgeon constructs a three-dimensional scaffold that neutralizes shear, tension, and compressive forces simultaneously. This orthogonal plating strategy significantly increases the construct's resistance to torsional and bending moments, providing a level of rigidity that a single plate cannot achieve.

Furthermore, the low-profile nature of fragment-specific implants minimizes soft tissue irritation and tendon impingement, a common complication associated with bulky traditional plates. The implants are designed to sit flush against the cortical bone, often contoured to match the complex topography of the distal radius. This close approximation not only improves biomechanical stability but also preserves the critical gliding planes for the extensor and flexor tendons, facilitating early, unimpeded active motion. The ability to achieve rigid, multi-columnar stability while minimizing the implant footprint is the defining biomechanical advantage of the fragment-specific approach.
Detailed Surgical Anatomy and Biomechanics
The Radial Column and Brachioradialis Deforming Forces
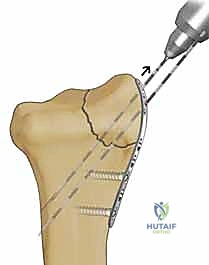
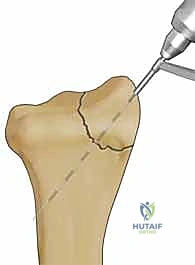
A profound comprehension of distal radius anatomy is the bedrock upon which successful fragment-specific fixation is built. The distal radius is conceptually divided into three distinct biomechanical columns, as popularized by Rikli and Regazzoni: the radial, intermediate, and ulnar columns. The radial column, encompassing the radial styloid and the scaphoid fossa, serves as the critical lateral buttress of the radiocarpal joint. Its structural integrity is paramount for maintaining radial length, radial inclination, and supporting the scaphoid in its normal spatial orientation.

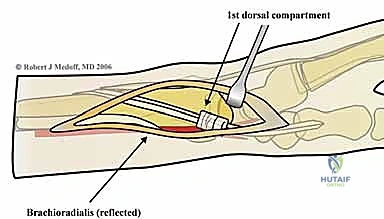
The stout radioscaphocapitate (RSC) and long radiolunate (LRL) ligaments originate from the volar aspect of the radial styloid, acting as primary stabilizers of the proximal carpal row. When the radial column is fractured, the tension within these ligaments can lead to secondary carpal translation if the osseous anatomy is not perfectly restored. Furthermore, the radial column is subject to immense dynamic deforming forces, most notably from the brachioradialis muscle. The brachioradialis inserts broadly onto the base of the radial styloid, and in the setting of a fracture, its tonic contraction exerts a proximal, volar, and supinating deforming force.
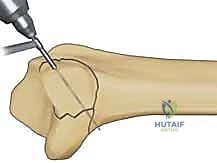
This muscular pull leads to shortening of the radial column, loss of radial inclination, and subsequent impaction of the carpus into the metaphyseal void. Metaphyseal comminution at the base of the styloid further compromises stability, creating a fulcrum for angular deformity. Surgical fixation of the radial column must, therefore, be robust enough to counteract the brachioradialis pull. This is typically achieved through the application of a dedicated radial pin plate that acts as a tension band against the deforming muscular forces, ensuring the scaphoid facet remains anatomically reduced and the crucial ligamentous origins are stabilized.

The Volar Rim and Lunate Facet Load-Bearing Mechanics
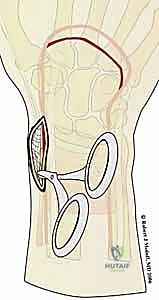
The intermediate column, primarily comprising the lunate facet and the sigmoid notch, is the primary load-bearing axis of the wrist, transmitting the majority of axial forces from the carpus to the forearm. Within this column, the volar rim of the lunate facet is an anatomical structure of critical importance. The volar rim provides the essential volar buttress that prevents palmar subluxation of the carpus and serves as the origin for the short radiolunate (SRL) ligament, a stout, unyielding structure that tethers the lunate to the distal radius.
We typically encounter two distinct patterns of instability when the volar rim is compromised. The Volar Instability Pattern is characterized by shortening and volar translation of the volar marginal fragment, inevitably dragging the tethered lunate with it and leading to catastrophic radiocarpal subluxation. The Axial Instability Pattern occurs when extreme axial impaction drives the carpus proximally, forcing the volar rim into severe dorsiflexion and creating a massive articular step-off. Because the volar rim fragments are often diminutive, highly comminuted, and located distal to the watershed line, standard volar locking plates frequently fail to capture them adequately.
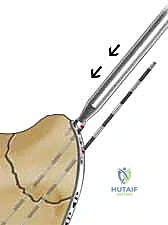
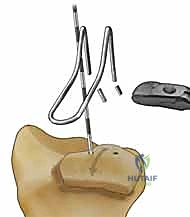
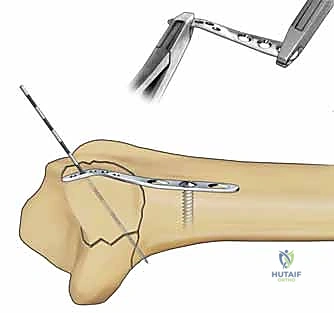
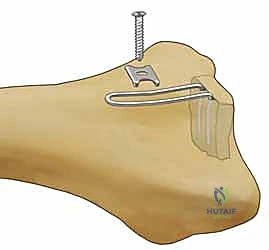
Attempting to place standard locking screws into these small, distal fragments carries an unacceptably high risk of intra-articular penetration. Fragment-specific fixation addresses this by utilizing specialized, low-profile volar hook plates or wire forms that contour distally over the watershed line. These implants physically buttress the small volar rim fragments, neutralizing the shear forces and restoring the critical volar restraint of the radiocarpal joint without violating the articular surface.

The Ulnar Corner and Distal Radioulnar Joint Kinematics
The ulnar corner fragment, representing the dorsal and ulnar aspect of the lunate facet and the dorsal half of the sigmoid notch, is a frequently underappreciated component of complex distal radius fractures. This fragment is typically generated by the forceful impaction of the lunate into the articular surface during high-energy trauma, causing the dorsal-ulnar corner to shear off, migrate dorsally, and shorten proximally. The anatomical significance of this fragment cannot be overstated, as it serves as the primary attachment site for the dorsal radioulnar ligament, a critical component of the triangular fibrocartilage complex (TFCC).

Residual displacement or malunion of the ulnar corner leads to profound incongruity of the sigmoid notch, fundamentally altering the kinematics of the distal radioulnar joint (DRUJ). This incongruity results in a loss of the normal sweeping motion of the ulnar head within the sigmoid notch during pronation and supination. Consequently, patients experience severe restriction of forearm rotation, chronic DRUJ instability, and early-onset post-traumatic arthrosis.
Because this fragment is located dorsally and ulnarly, it is virtually impossible to reduce and stabilize from a standard volar approach using a single VLP. Fragment-specific fixation mandates a dedicated dorsal or combined approach to directly visualize the sigmoid notch, reduce the ulnar corner fragment, and stabilize it with a specialized dorsal-ulnar pin plate or micro-screws. This targeted intervention is the only reliable method to restore the anatomical concavity of the DRUJ and preserve forearm rotation.

Dorsal Wall Integrity and Comminution Patterns
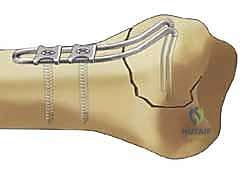
The dorsal wall of the distal radius acts as the primary restraint against dorsal translation of the carpus. Fragmentation of the dorsal wall is a hallmark of high-energy axial loading and severe dorsal bending injuries. Unlike the thick, dense cortical bone of the volar cortex, the dorsal cortex is inherently thinner and more susceptible to explosive comminution upon impact. When the dorsal wall shatters, it creates a massive structural void that eliminates the dorsal buttress, rendering the fracture highly unstable in the sagittal plane.
This loss of dorsal integrity allows the carpus to translate dorsally, leading to a profound loss of volar tilt and secondary carpal instability. Managing dorsal wall comminution requires meticulous surgical strategy. While volar locked plating relies on subchondral support to "prop up" the articular surface, severe dorsal comminution can lead to late collapse if the subchondral screws lack sufficient purchase or if the dorsal void is too expansive to be bridged by rafting screws alone.
In the fragment-specific paradigm, the dorsal wall is addressed directly. This may involve the use of low-profile dorsal plates applied orthogonally to bridge the comminution, or the utilization of structural bone graft (autograft or allograft) to fill the metaphyseal defect and provide a biological buttress. By explicitly reconstructing the dorsal wall, the surgeon restores the normal load-sharing biomechanics of the distal radius, preventing late dorsal collapse and ensuring the long-term maintenance of the anatomical reduction.
Exhaustive Indications and Contraindications
Defining the Ideal Candidate for Fragment-Specific Fixation
The decision to employ a fragment-specific fixation strategy over traditional volar locked plating hinges on a rigorous preoperative assessment of the fracture's "personality." The ideal candidate for FSF presents with a complex, multi-fragmentary intra-articular fracture where the discrete components cannot be adequately captured or neutralized by a single, fixed-angle implant. Primary indications include severe four-part articular fractures, which typically involve independent radial styloid, volar lunate facet, dorsal lunate facet, and metaphyseal shaft fragments.
Furthermore, FSF is definitively indicated for specific shear fracture patterns that are notoriously difficult to manage. Volar marginal shearing fractures (often termed volar Barton's fractures) that involve very small, distal fragments located beyond the watershed line are prime indications. These fragments are critical for carpal stability but are too small for standard screw fixation without risking articular penetration. Similarly, isolated, displaced radial styloid fractures (Chauffeur's fractures) with associated scapholunate ligament injuries benefit immensely from the targeted compression and tension-band effect provided by a dedicated radial column plate.

Ultimately, any fracture pattern where a standard VLP leaves a critical anatomical component (such as the dorsal wall or ulnar corner) unsupported is a definitive indication for a modular, fragment-specific approach. Highly comminuted fractures with significant metaphyseal bone loss, and fractures exhibiting profound radiocarpal or DRUJ instability, also demand the multiplanar stability that only a modular system can provide.
Absolute and Relative Contraindications to the Technique
While fragment-specific fixation is a powerful tool in the orthopedic armamentarium, it is not without limitations, and careful patient selection is paramount. Absolute contraindications are relatively few but critical to observe. Active, untreated local or systemic infection absolutely precludes the insertion of internal hardware. Additionally, severe soft tissue compromise, such as massive degloving injuries, untreated compartment syndrome, or heavily contaminated open fractures (Gustilo-Anderson Grade III), may necessitate temporizing external fixation rather than immediate, extensive internal plating.

Relative contraindications revolve around patient physiology, functional demands, and the inherent complexity of the procedure. Non-ambulatory patients with severe baseline dementia or minimal functional demands may be better served by conservative management or less invasive techniques. The extensive surgical time, multiple incisions, and complex rehabilitation associated with FSF may not yield a proportional clinical benefit in this demographic. Severe, uncorrectable coagulopathies also present a relative contraindication due to the extensive surgical approaches required.
Furthermore, the surgeon's experience and familiarity with the modular implant systems are critical. FSF is technically demanding, requires a deep understanding of three-dimensional carpal anatomy, and possesses a steep learning curve. In the hands of an inexperienced operator, the risk of iatrogenic nerve injury, tendon irritation from poorly placed low-profile plates, and prolonged operative times may outweigh the biomechanical advantages of the technique.

Algorithmic Decision-Making and Clinical Parameters
The transition from preoperative imaging to intraoperative execution requires a structured, algorithmic approach. Surgeons must systematically evaluate the radial column, the intermediate column, and the ulnar corner to determine the necessity of modular implants. If a standard volar plate can secure the lunate facet but fails to compress the radial styloid against the brachioradialis pull, a supplementary radial pin plate is indicated.
Clinical parameters such as bone quality, patient age, and occupational demands heavily influence this algorithm. In a young manual laborer with a high-energy crush injury, maximizing biomechanical rigidity via orthogonal dorsal and volar plating is essential to permit early return to heavy lifting. Conversely, in an osteoporotic patient with a low-energy fall, the goal shifts toward utilizing wire forms and hook plates to gently cradle fragile subchondral bone without causing iatrogenic fragmentation.
| Parameter | Indications for Fragment-Specific Fixation | Contraindications for Fragment-Specific Fixation |
|---|---|---|
| Fracture Pattern | 4-part articular, volar marginal shear, dorsal blowout, Chauffeur's | Simple extra-articular, non-displaced 2-part |
| Anatomical Defect | Ulnar corner dissociation, massive metaphyseal void | Intact volar cortex, solid dorsal buttress |
| Patient Profile | High functional demand, young trauma, severe osteoporosis | Severe dementia, non-ambulatory, low demand |
| Soft Tissue Status | Intact or minor swelling, closed injury | Active infection, Gustilo III open, compartment syndrome |
| Surgeon Factors | High volume trauma experience, familiarity with modular sets | Limited experience, lack of specialized implant availability |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities and 3D Reconstruction
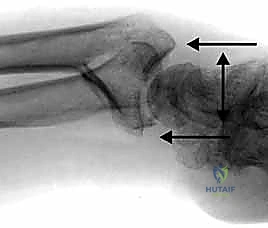
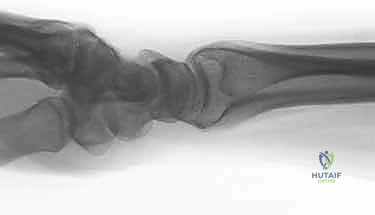
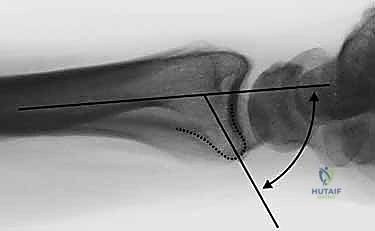
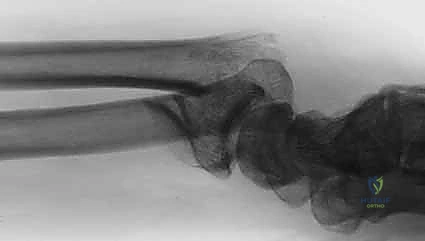
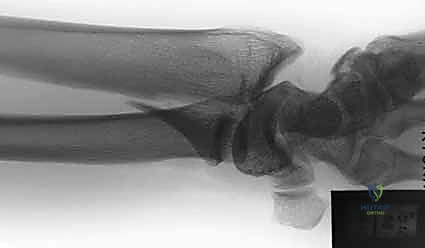
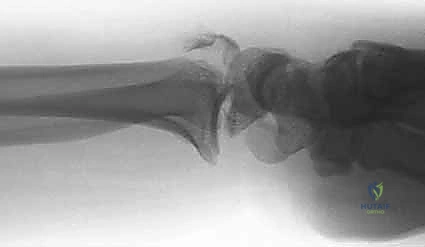
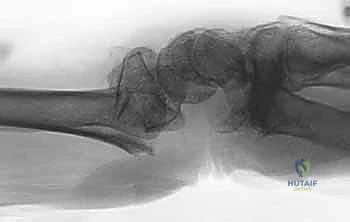
The foundation of successful fragment-specific fixation is an uncompromising preoperative imaging protocol. Standard posteroanterior, lateral, and oblique plain radiographs are mandatory but frequently insufficient for deciphering the complex spatial geometry of multi-fragmentary intra-articular fractures. The superimposition of carpal bones and metaphyseal comminution often masks critical details, such as articular step-offs, coronal plane splits, and rotational malalignment of the ulnar corner.
Consequently, high-resolution, thin-slice Computed Tomography (CT) without contrast is considered the gold standard and is virtually obligatory prior to FSF. Sagittal and coronal 2D reformats allow the surgeon to meticulously trace the fracture lines, identify independent articular fragments, and assess the degree of central impaction. Furthermore, 3D volumetric reconstructions provide an invaluable topographical map of the injury, enabling the surgeon to mentally "disassemble and reassemble" the fracture prior to entering the operating theater.

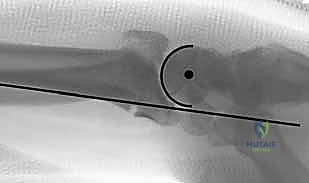
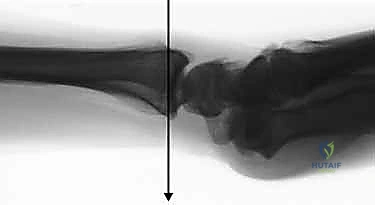
In cases of severe impaction where the fracture fragments are compressed into a chaotic mass, traction radiography can be employed. By applying longitudinal traction during fluoroscopy or plain film acquisition, ligamentotaxis partially restores radial length and distracts the articular fragments, unmasking the true fracture pattern and providing a preview of the reduction that can be achieved intraoperatively.
Digital Templating and Implant Selection Strategy
Once the fracture morphology is fully delineated via advanced imaging, digital templating becomes the next critical phase of preoperative planning. Unlike standard volar plating, where a single implant size and length are selected, FSF requires the surgeon to choreograph a symphony of modular implants. Using specialized templating software, the surgeon overlays various low-profile plates, wire forms, and screws onto the CT reformats to determine the optimal trajectory and implant size for each discrete fragment.
The selection strategy must account for the specific biomechanical demands of each column. For the radial styloid, a contoured pin-plate is chosen to resist the proximal migration induced by the brachioradialis. For the volar lunate facet, a hook plate or a specialized subchondral wire form is selected to buttress the volar rim without violating the joint space. For the dorsal wall, a low-profile titanium mini-plate is templated to bridge the comminution and act as a rigid dorsal restraint.
Crucially, the surgeon must plan the spatial relationship between these implants to prevent hardware collision. Because multiple plates and screws will be inserted from different orthogonal planes (volar, dorsal, and radial), meticulous 3D templating ensures that the trajectory of a volar locking screw does not intersect with a dorsal buttress pin. This foresight prevents intraoperative frustration and the need for repetitive hardware adjustments.
Optimal Operative Suite Setup and Patient Positioning
The physical setup of the operative suite and the positioning of the patient are paramount for facilitating the complex, multi-incisional approaches required for FSF. The patient is placed supine on a standard operating table with the operative extremity extended onto a radiolucent hand table. A well-padded upper arm tourniquet is applied to provide a bloodless surgical field, which is critical for identifying small articular fragments and delicate neurovascular structures.

The fluoroscopy unit (C-arm) must be positioned to allow unhindered, rapid acquisition of posteroanterior, lateral, and oblique views without compromising the sterile field or requiring awkward repositioning of the extremity. Typically, the C-arm is brought in parallel to the hand table, with the monitor placed directly across from the primary surgeon for optimal ergonomic viewing.

The surgical team, including the primary surgeon, assistant, and scrub nurse, must be positioned to allow seamless transition between volar and dorsal approaches. The modular implant sets, which often contain dozens of specialized plates, pins, and instruments, must be meticulously organized on the back table. The scrub nurse should be intimately familiar with the sequence of the fragment-specific algorithm, ensuring that the correct modular components are readily available as the reconstruction progresses from the intermediate column to the radial and ulnar columns.
Step-by-Step Surgical Approach and Fixation Technique
The Modified Henry Approach and Volar Exposure
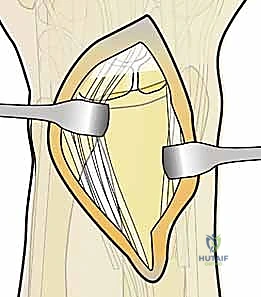
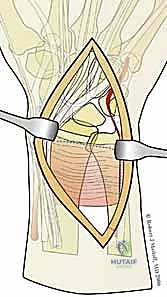
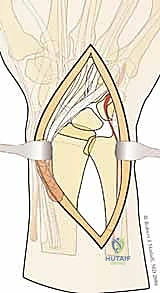
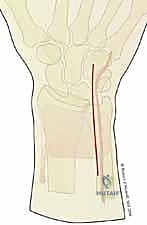
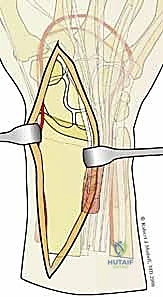
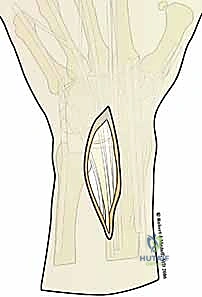
The surgical execution of fragment-specific fixation typically commences with the volar approach, specifically the modified Henry approach, to address the intermediate column and the volar rim. An longitudinal incision is made overlying the flexor carpi radialis (FCR) tendon. The FCR sheath is incised, and the tendon is retracted ulnarly, protecting the median nerve. The floor of the FCR sheath is then incised to reveal the deep space containing the flexor pollicis longus (FPL) and the pronator quadratus (PQ) muscle.

The PQ is sharply elevated from its radial and distal borders, exposing the volar metaphysis and the critical watershed line of the distal radius. In the setting of a volar marginal
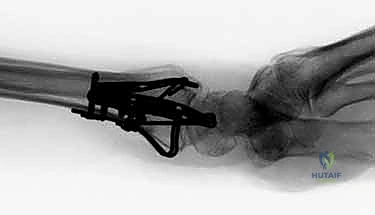
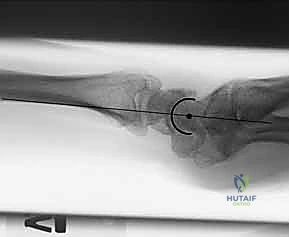
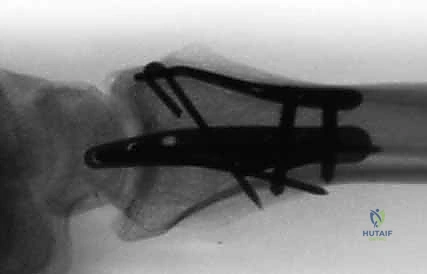
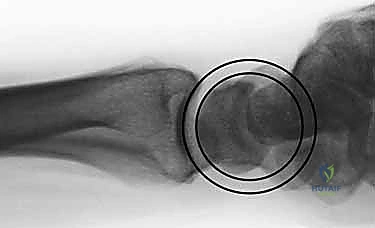
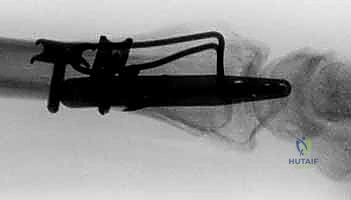
Clinical & Radiographic Imaging Archive