Forearm Osteotomy and Exostosis Excision for Multiple Hereditary Exostoses: An Intraoperative Masterclass

Key Takeaway
This masterclass guides orthopaedic fellows through forearm osteotomy and exostosis excision for Multiple Hereditary Exostoses (MHE). We cover detailed anatomy, meticulous surgical steps from incision to hardware, and critical pearls for managing complex deformities and preventing complications. Master the techniques for improved function and alignment in affected patients.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater. Today, we are undertaking a highly complex and challenging reconstructive case: the correction of a severe forearm deformity stemming from Multiple Hereditary Exostoses (MHE). This condition, also recognized in the literature as multiple osteochondromatosis or diaphyseal aclasis, presents a unique and formidable blend of growth disturbance, profound anatomical distortion, and progressive functional impairment. Our objective in the surgical management of these patients extends far beyond the mere cosmetic correction of a bowed forearm; our mandate is to meticulously restore the biomechanical axes, stabilize adjacent articulations, and fundamentally improve the patient's long-term quality of life through tailored, precision-driven surgical interventions.
Multiple hereditary exostoses is a familial skeletal disorder characterized by an autosomal dominant inheritance pattern. First described comprehensively by Boyer in 1814, the disease is defined by the ubiquitous formation of benign, cartilage-capped bony prominences—exostoses—that arise predominantly from the metaphyses of long bones undergoing endochondral ossification. Modern molecular genetics has identified that MHE is primarily caused by loss-of-function mutations in the tumor suppressor genes EXT1 (located on chromosome 8q24) and EXT2 (located on chromosome 11p11-p12). These genes encode glycosyltransferases essential for the biosynthesis of heparan sulfate. The resulting heparan sulfate deficiency disrupts critical signaling pathways (such as Indian Hedgehog and Wnt) in the growth plate, leading to the abnormal proliferation of epiphyseal chondroblasts and a subsequent catastrophic failure of normal metaphyseal remodeling.
The phenotypic penetrance of MHE is highly age-dependent and nearly complete by skeletal maturity. Clinical manifestations typically become apparent between 2 and 3 years of age, with approximately 50% of affected individuals demonstrating palpable or radiographically visible lesions. By the age of 12, the presence of exostoses is almost universally evident across the patient cohort. Once the physes close and skeletal maturity is achieved, the vast majority of these lesions become quiescent and fully ossify; however, the complex multidirectional deformities they imparted upon the growing skeleton remain permanently etched into the patient's anatomy. The overall penetrance in adult obligate heterozygotes ranges between 93% and 100%. Notably, approximately 10% of individuals presenting with documented MHE manifestations possess no identifiable family history, representing de novo sporadic mutations.
A critical, life-altering consideration in the longitudinal management of MHE is the potential for malignant transformation of a benign osteochondroma into a secondary peripheral chondrosarcoma. While exceedingly rare during the pediatric years, the cumulative lifetime risk of malignant degeneration in adults with MHE is estimated to range between 0.57% and 5%. Osteochondromas, histologically mirroring the epiphyseal growth plate with a bony stalk and a cartilaginous cap, are the most common benign bone tumors. When malignant transformation occurs, it typically presents as an enlarging, painful mass in a skeletally mature patient. The clinical course of these secondary chondrosarcomas is generally indolent, and the prognosis remains highly favorable if wide surgical margins are achieved early. However, routine clinical and radiographic surveillance is mandatory, as patients with MHE maintain a normal life expectancy unless malignant degeneration with subsequent metastasis (usually hematogenous to the lungs) ensues.
Detailed Surgical Anatomy and Biomechanics
Forearm deformities are a quintessential hallmark of MHE, reported in an estimated 30% to 60% of the affected patient population. The natural history of these deformities is relentlessly progressive during the growing years, culminating in variable but predictably worsening weakness, chronic pain, and severe functional deficits. These pathological changes manifest clinically as subluxation or frank dislocation of the radial head, profoundly limited pronation and supination, severe ulnar deviation at the radiocarpal joint, and potential compression neuropathies affecting adjacent neurovascular structures. Cosmetically, patients present with the classic "bowed, short, and knobby-appearing forearm," a phenotype that frequently causes significant psychosocial distress.

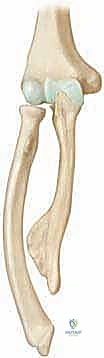
An intimate knowledge of the normal anatomy and biomechanics of the immature forearm is instrumental in understanding the pathogenesis of MHE-induced deformities. The forearm is a complex, articulated bi-osseous unit where the radius and ulna must function in perfect synchrony. The deformities seen in MHE are almost universally driven by a progressive length discrepancy between the radius and the ulna. This asynchronous rate of longitudinal growth in a confined anatomical compartment creates a high risk of distortion. Crucially, the majority of the longitudinal growth of the ulna occurs at its distal physis. Unfortunately, this distal ulnar physis is also the most frequently affected growth plate in MHE, with involvement seen in 30% to 85% of cases. The resulting premature growth arrest or severe retardation of the distal ulna sets the stage for the cascade of forearm deformities.

Biomechanically, the ulna functions as a rigid, stable swivel hinge at the ulnohumeral joint, around which the radius rotates to facilitate pronation and supination. This intricate rotational movement demands absolute axial and rotational alignment of both bones, as well as the uncompromised integrity of the proximal radioulnar joint (PRUJ), distal radioulnar joint (DRUJ), and the central band of the interosseous membrane (IOM). Even a minimal axial deviation, asymmetric bone shortening, or ligamentous tethering can severely hinder this crucial kinematic function. When the distal ulnar physis is retarded by an exostosis, the ulna becomes relatively shortened and curved. The normally growing radius is then tethered by the shortened ulna via the DRUJ ligaments, the ulnar collateral ligament of the wrist, and the IOM, forcing the radius to bow laterally and anteriorly to accommodate its own continued longitudinal growth.
Furthermore, the local presence of a massive, sessile exostosis can directly cause radial bowing by mechanically disturbing hemiepiphyseal growth. Like solitary osteochondromas, MHE lesions can be sessile, pedunculated, or cauliflower-like, nearly always pointing away from the physis. In MHE, however, these lesions are characteristically larger, more bizarrely shaped, and involve a significantly greater portion of the metaphysis and diaphysis. As the radius bows and the ulna shortens, the radiocapitellar joint experiences massive compressive and shear forces, ultimately leading to cubitus varus deformity and radial head dislocation. Radial head dislocation is reported in up to 22% of affected forearms, presenting with mechanical blocks to elbow motion, chronic pain, and a characteristic mild flexion contracture. At the wrist, the relative ulnar shortening results in increased ulnar tilt of the radial epiphysis, ulnar deviation of the hand, and progressive ulnar translocation of the carpus, severely limiting radial deviation and forearm rotation.

Exhaustive Indications and Contraindications
The decision-making process for surgical intervention in MHE forearm deformities is nuanced, requiring a delicate balance between prophylactic intervention to prevent permanent joint damage and therapeutic reconstruction to restore lost function. The timing of surgery remains one of the most debated topics in pediatric orthopedic oncology. The primary goals of surgery are to prevent or reduce radial head dislocation, restore the DRUJ anatomy, improve the cosmetic appearance of the limb, and maximize the functional arc of pronation and supination. Intervention is generally guided by the Masada classification, which categorizes deformities based on the location of the exostoses and the presence or absence of radial head dislocation.
Absolute indications for surgical intervention include progressive symptomatic radial head subluxation or frank dislocation, severe and progressive loss of forearm rotation that interferes with activities of daily living, and significant pain originating from mechanical impingement by a specific exostosis. Early intervention is strongly advocated when serial radiographs demonstrate worsening ulnar variance and an increasing Radial Articular Angle (RAA), as early ulnar lengthening can de-tether the radius and theoretically prevent the progression to radial head dislocation. Furthermore, any rapid growth of an exostosis, newly onset pain in a previously asymptomatic lesion, or neurovascular compromise (such as posterior interosseous nerve palsy) necessitates immediate surgical exploration and excision.
Conversely, absolute contraindications include asymptomatic, non-progressive deformities in skeletally mature individuals who have adapted to their limited range of motion without pain. Surgery in these patients often yields minimal functional improvement and carries a high risk of iatrogenic stiffness or nerve injury. Relative contraindications include very young patients (under the age of 5 or 6) with mild deformities, as the recurrence rate of both the exostoses and the deformity is unacceptably high if osteotomies are performed too early in the growth cycle. In these cases, watchful waiting with serial clinical and radiographic examinations every 6 to 12 months is the preferred management strategy.
| Factor | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Clinical Symptoms | Intractable pain, neurovascular compression, severe functional deficit in ADLs. | Asymptomatic, highly functional despite radiographic deformity. |
| Joint Stability | Progressive radial head subluxation or frank dislocation. | Stable PRUJ and DRUJ with no signs of progressive subluxation. |
| Deformity Progression | Rapidly worsening ulnar shortening, increasing RAA, severe radial bowing. | Static deformity in a skeletally mature patient. |
| Patient Age/Maturity | Mid-childhood to adolescence (to prevent joint destruction) with sufficient bone stock. | Very young children (<5 years) due to high recurrence risk, unless nerve compression is present. |
| Lesion Characteristics | Rapidly growing lesion, suspicion of malignant transformation (chondrosarcoma). | Quiescent, heavily ossified lesions in adults with no pain. |
Pre-Operative Planning, Templating, and Patient Positioning
Before a single incision is made, exhaustive preoperative planning is paramount to the success of MHE forearm reconstruction. This meticulous process begins with a comprehensive history and physical examination. The surgeon must ascertain the onset and progression of symptoms, focusing on pain, weakness, functional difficulties (such as inability to receive change in the palm of the hand or use a keyboard), and the patient's primary cosmetic concerns. A detailed physical examination of the entire upper extremity is mandatory. We must evaluate comparative lengths of the forearms, assess the carrying angle and varus/valgus stability of the elbow, and precisely measure the active and passive range of motion of the elbow, wrist, and forearm (flexion/extension, radial/ulnar deviation, and pronation-supination).
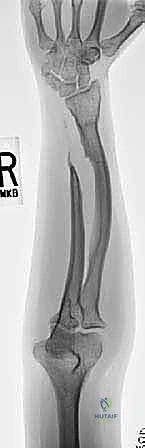
Radiographic evaluation is the cornerstone of our preoperative templating. Plain radiography is usually sufficient to confirm the diagnosis, classify the deformity (via the Masada system), and determine the morphology of the exostoses. At least two full, orthogonal views of the forearm—a true anteroposterior and a true lateral, encompassing both the elbow and the wrist joints—are absolutely necessary. These images allow us to quantify several critical parameters. First, we assess ulna variance, determining the exact millimeter discrepancy between the distal articular surfaces of the radius and ulna. Second, we measure the Radial Articular Angle (RAA). This angle is defined between a line running along the articular surface of the radius and a line perpendicular to a line joining the center of the radial head to the radial border of the distal radial epiphysis. The normal range is 15 to 30 degrees; angles exceeding this indicate severe tethering and distal radial deformity.

Third, we calculate the Carpal Slip (CS), which measures the percentage of the lunate in contact with the radius. A line drawn from the center of the olecranon through the ulnar border of the radial epiphysis normally bisects the lunate. An abnormal CS is present when ulnar displacement of the lunate exceeds 50%, indicating progressive instability of the carpus due to loss of ulnar support. Finally, the relative radial bow is assessed to determine if a corrective radial osteotomy will be required in conjunction with ulnar lengthening. In complex cases, particularly those with impending radial head dislocation or suspected malignant transformation, advanced imaging such as MRI or 3D-reconstructed CT scans are invaluable for assessing the cartilage cap thickness, evaluating the integrity of the interosseous membrane, and planning patient-specific osteotomy trajectories.


Patient positioning in the operating room must facilitate simultaneous access to the elbow, forearm diaphysis, and wrist. The patient is placed supine with the affected extremity extended on a radiolucent hand table. A sterile pneumatic tourniquet is applied high on the brachium. The entire upper extremity, from the fingertips to the axilla, is prepped and draped to allow for unhindered intraoperative fluoroscopy and manipulation. A sterile C-arm must be positioned to allow for seamless AP and lateral imaging throughout the procedure without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The surgical reconstruction of the MHE forearm is frequently a multi-staged or multi-component procedure within a single anesthetic event. The classical approach involves three primary objectives: excision of the offending exostoses, restoration of ulnar length, and correction of radial bowing or radial head dislocation. The procedure begins with the systematic excision of the osteochondromas that are causing mechanical blocks, neurovascular tethering, or severe cosmetic deformity.

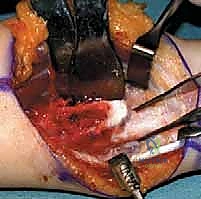
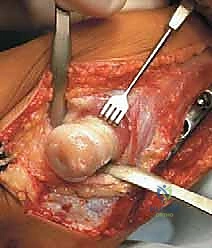
For distal ulnar exostoses, a longitudinal incision is made over the subcutaneous border of the ulna. The extensor carpi ulnaris (ECU) is retracted, and the exostosis is exposed. It is absolutely critical to perform an extraperiosteal resection. Leaving the periosteal sleeve intact over the exostosis significantly increases the risk of recurrence, as the cambium layer contains the aberrant chondroblasts responsible for the pathology. The exostosis is excised flush with the native cortex using sharp osteotomes or a high-speed burr, taking immense care not to violate the adjacent physis if the patient is still growing. For proximal radial exostoses, a modified Kocher or Henry approach is utilized, demanding meticulous identification and protection of the posterior interosseous nerve (PIN), which is frequently draped over or displaced by the mass.
Following exostosis excision, attention is turned to the ulnar lengthening osteotomy. The goal here is to restore the normal distal radioulnar relationship and de-tether the radius. Depending on the magnitude of the discrepancy, lengthening can be achieved acutely or gradually. For discrepancies less than 1.5 to 2.0 cm, an acute lengthening with a structural tricortical iliac crest bone graft and rigid internal plate fixation is often preferred. A transverse or step-cut osteotomy is performed in the distal third of the ulnar diaphysis. The ulna is distracted using a lamina spreader until the distal articular surface is level with the sigmoid notch of the radius. The structural graft is impacted into the defect, and a dynamic compression plate is applied.

For larger discrepancies (greater than 2.0 cm), gradual distraction osteogenesis using a monolateral external fixator or a circular frame is mandatory to prevent excessive tension on the ulnar nerve and the interosseous membrane. Half-pins are inserted proximally and distally to the planned osteotomy site under fluoroscopic guidance. A low-energy corticotomy is performed, preserving the periosteal blood supply. Distraction typically commences on postoperative day 5 to 7 at a rate of 0.25 mm every 6 hours (1 mm per day) until the desired length and neutral ulnar variance are achieved.

If the radius remains severely bowed after ulnar lengthening, a corrective radial osteotomy is indicated. This is typically performed at the apex of the deformity. A closing wedge or opening wedge osteotomy is executed, and the radius is fixed with a pre-contoured locking plate. If the radial head is dislocated (Masada Type I or IIb), open reduction must be attempted. This often requires release of the contracted annular ligament and joint capsule. If the radial head is irreducible or highly unstable post-reduction, an annular ligament reconstruction (such as the Bell-Tawse procedure using a slip of the triceps tendon or palmaris longus) may be necessary. In older adolescents with chronic, painful, and irreducible radial head dislocations, a radial head excision may be considered as a salvage procedure, though this is strictly avoided in growing children to prevent proximal migration of the radius.



Complications, Incidence Rates, and Salvage Management
The surgical management of MHE forearms is fraught with potential complications, primarily due to the altered anatomy, the necessity of operating near delicate physes, and the extensive nature of the reconstructive osteotomies. A thorough understanding of these risks and their salvage pathways is essential for any orthopedic surgeon undertaking these procedures.
The most common complication in the pediatric population is the recurrence of the deformity. Because MHE is a systemic disorder of endochondral ossification, the underlying biological drive for asymmetric growth persists until skeletal maturity. Even with perfect initial surgical correction, the ulna may fall behind in longitudinal growth again, leading to recurrent radial bowing and carpal slip. Recurrence rates for deformity have been reported to be as high as 40% to 60% in children operated on before the age of 10. Management of recurrence typically involves a secondary ulnar lengthening procedure near skeletal maturity. Recurrence of the excised exostosis itself is less common (less than 5%) if an extraperiosteal resection was meticulously performed, but it can occur if residual cartilage cap or periosteum is left behind.
Nonunion or delayed union at the osteotomy sites is another significant concern, particularly with acute ulnar lengthening utilizing structural bone grafts. The incidence of nonunion ranges from 5% to 15%. This is often due to inadequate graft compression, poor soft tissue envelope, or premature failure of fixation. Salvage management requires returning to the operating room for debridement of the nonunion site, application of copious autologous cancellous bone graft (often harvested from the iliac crest or proximal tibia), and revision of the internal fixation to a more rigid construct, potentially supplementing with bone morphogenetic proteins (BMPs) off-label if the patient is nearing skeletal maturity.
Neurologic complications, particularly involving the posterior interosseous nerve (PIN) and the ulnar nerve, can occur via two distinct mechanisms: direct iatrogenic injury during exposure/excision of proximal radial exostoses, or traction neuropraxia during acute ulnar lengthening or radial head reduction. The incidence of transient nerve palsy is estimated at 3% to 8%. Most traction injuries resolve spontaneously with observation and supportive care over 3 to 6 months. If a nerve is known to be transected intraoperatively, primary microsurgical repair or nerve grafting is indicated immediately. Pin tract infections are ubiquitous in patients undergoing gradual distraction osteogenesis with external fixators, occurring in up to 30% of cases. These are generally managed successfully with local pin care and oral antibiotics, rarely requiring premature removal of the fixator.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Deformity Recurrence | 40% - 60% (in young children) | Continued asymmetric growth, early age at initial surgery. | Delay initial surgery if possible; perform repeat lengthening near skeletal maturity. |
| Nonunion / Delayed Union | 5% - 15% | Poor graft incorporation, inadequate rigid fixation, acute massive lengthening. | Revision ORIF with autologous bone grafting; ensure stable fixation. |
| Nerve Palsy (PIN / Ulnar) | 3% - 8% | Direct surgical trauma, excessive traction during acute lengthening. | Meticulous dissection; limit acute lengthening to <2cm; observation for traction neuropraxia. |
| Pin Tract Infection | 20% - |
