Capsular Interposition Arthroplasty for Hallux Rigidus: An Operative Masterclass

Key Takeaway
Welcome, fellows, to an immersive operative masterclass on capsular interposition arthroplasty for hallux rigidus. We'll meticulously navigate the first MTP joint, from precise incision and anatomical dissection to meticulous tissue balancing and hardware application. This procedure aims to restore pain-free motion in end-stage arthritis, emphasizing crucial neurovascular protection and optimal long-term function. Prepare for a granular, real-time walkthrough, addressing every critical step and potential pitfall.
Comprehensive Introduction and Patho-Epidemiology
Alright, fellows, gather 'round. Welcome to the operating theater. Today, we are tackling a challenging but immensely rewarding case: Capsular Interpositional Arthroplasty for advanced Hallux Rigidus. This procedure is designed to restore pain-free motion in patients suffering from debilitating degenerative arthritis of the first metatarsophalangeal (MTP) joint, particularly when conservative measures have failed, and joint-preserving options like cheilectomy are no longer sufficient. Our goal here is to create a functional, stable, and mobile joint using the patient's own tissue, bridging the therapeutic gap between simple debridement and definitive arthrodesis.
Hallux rigidus is essentially progressive, degenerative osteoarthritis of the first MTP joint. It is characterized by debilitating pain, a significantly decreased range of motion (ROM) primarily in dorsiflexion, and the formation of robust, proliferative osteophytes, especially along the dorsal and lateral articular margins. Epidemiologically, it is the most common arthritic condition of the foot, affecting roughly 1 in 40 adults over the age of 50. The precise etiology is often multifactorial, encompassing repetitive microtrauma, altered first ray biomechanics, metatarsus primus elevatus, and occasionally systemic inflammatory conditions, though primary osteoarthritis remains the most prevalent driver.
Patients typically present with localized pain to the dorsal aspect of the great toe MTP joint, which is exquisitely exacerbated by activities requiring terminal dorsiflexion, such as wearing high-heeled shoes, running, ascending stairs, or executing specific yoga poses. They frequently complain of a progressive increase in the girth of the MTP joint, sometimes erroneously attributing it to a "bunion-type deformity." Initially, the loss of motion might be minimal and purely functional, but over years, the mechanical block becomes profound, eventually leading to near-total ankylosis. You might also observe compensatory hyperextension of the hallucal interphalangeal (IP) joint in long-standing cases, a biomechanical adaptation that can lead to secondary IP joint arthritis.
Pain felt at the mid-range of the motion arc often implies a more global MTP joint arthritis, which is precisely why we are considering an interpositional arthroplasty today, rather than just a dorsal cheilectomy. A simple cheilectomy only addresses the dorsal impingement; it does nothing for the denuded central cartilage. Furthermore, during physical examination, a positive Tomassen's sign—where dorsiflexion of the MTP joint is blocked when the ankle is held in neutral—must be evaluated. This suggests a stenosing flexor hallucis longus (FHL) tenosynovitis rather than a static dorsal osteophyte, an important differential to rule out before committing to an articular resection.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate anatomy and biomechanics of the first MTP joint is paramount for a successful outcome and, more importantly, to avoid critical, limb-altering complications. The first MTP joint is a complex hinge joint formed by the convex, cam-shaped head of the first metatarsal and the shallow, concave base of the proximal phalanx. In the setting of hallux rigidus, the metatarsal head typically becomes broader and flatter, leading to increased contact pressure and altered kinematics. The instant center of rotation shifts, causing the joint to transition from a normal sliding-and-rolling motion to a purely compressive, grinding articulation.
The capsuloligamentous complex is the primary stabilizing structure of the first ray. The dorsal joint capsule is a robust fibrous structure that becomes pathologically thickened and contracted in hallux rigidus; ironically, this pathologic tissue serves as our primary source of interpositional material. The medial and lateral collateral ligaments provide crucial mediolateral stability. We must respect their integrity where possible, especially during the capsulotomy, to maintain coronal plane stability post-resection. Plantarly, the plantar plate-sesamoid-flexor hallucis brevis (FHB) tendon complex provides dynamic and static support. The FHB tendon, with its medial and lateral heads inserting into the sesamoids and subsequently the base of the proximal phalanx, plays a vital role in plantarflexion and stability. Disruption of this insertion without meticulous repair guarantees a catastrophic "cock-up" toe deformity.
The tendinous anatomy surrounding the first MTP joint requires meticulous navigation. The Extensor Hallucis Longus (EHL) tendon, a powerful dorsiflexor, runs superficially over the dorsal aspect of the joint. It must be identified and protected throughout the procedure, ensuring it is neither transected nor inadvertently tethered by capsular sutures. Deep to the EHL lies the Extensor Hallucis Brevis (EHB) tendon, which inserts onto the dorsal aspect of the proximal phalanx. In our technique, we will be transecting this tendon proximally and mobilizing it distally to augment our soft tissue interposition. Plantarly, the Flexor Hallucis Longus (FHL) tendon runs deep to the metatarsal head, between the sesamoids, and inserts onto the distal phalanx. It is a critical plantarflexor and must be protected from injury during any deep plantar suturing.
Neurovascular preservation is the hallmark of a master surgeon. The dorsomedial sensory cutaneous nerve to the hallux, a terminal branch of the superficial peroneal nerve, runs directly along the dorsomedial aspect of the MTP joint. It is highly susceptible to injury during the initial skin incision and subcutaneous dissection. Identify it early, mobilize it gently, and protect it meticulously; iatrogenic injury here leads to intractable, painful neuromas. Plantarly, the medial plantar digital nerves (including Joplin's nerve) run along the plantar-medial aspect of the great toe. While our primary approach is medial, deep dissection and especially the passage of plantar sutures require extreme caution to avoid ensnaring these nerves.
Exhaustive Indications and Contraindications
Patient selection is the single most critical variable in predicting the success of a capsular interposition arthroplasty. The ideal candidate is a moderately active individual, typically in their fifth to seventh decade of life, who presents with Coughlin and Shurnas Grade 3 or early Grade 4 hallux rigidus. These patients possess severe, global joint space narrowing, extensive periarticular osteophytosis, and subchondral sclerosis or cyst formation. Crucially, they must express a strong desire to maintain MTP joint motion—often for specific occupational requirements, footwear preferences (such as a modest heel), or recreational activities like cycling or light hiking—and explicitly wish to avoid a joint fusion.
Conversely, high-demand athletes, heavy manual laborers, and dancers present a significant challenge. While these individuals strongly desire motion, the interpositional arthroplasty may not withstand their extreme functional demands, leading to early failure, recurrent pain, or progressive deformity. For these high-demand patients, a primary arthrodesis remains the most predictable and durable option. Furthermore, a significantly long second metatarsal (a negative Maestro curve) is a relative contraindication. Resecting the base of the proximal phalanx inherently shortens the first ray, which can drastically shift weight-bearing forces laterally, resulting in severe transfer metatarsalgia under the second metatarsal head. If a long second metatarsal is present, a concomitant second metatarsal shortening osteotomy (e.g., Weil osteotomy) must be considered.
Absolute contraindications are non-negotiable. Patients with poor vascular status, such as severe peripheral arterial disease, lack the necessary healing capacity for this extensive soft-tissue and bony reconstruction. Peripheral neuropathy, commonly secondary to diabetes mellitus, eliminates the protective sensation necessary to prevent post-operative Charcot arthropathy or unrecognized hardware/suture failure. Active or recent local infection absolutely precludes the implantation of hardware or the creation of a large biological dead space. Finally, severe systemic inflammatory arthropathies (like advanced Rheumatoid Arthritis) often result in poor capsular tissue quality, making the interposition flap structurally inadequate and prone to rapid degradation.
| Category | Specific Conditions / Factors | Clinical Rationale |
|---|---|---|
| Primary Indications | Coughlin & Shurnas Grade 3 or 4 Hallux Rigidus | Global joint destruction where cheilectomy is insufficient. |
| Desire to preserve joint motion | Patient refuses arthrodesis due to footwear or lifestyle needs. | |
| Moderate activity demands | Older, community ambulators or recreational athletes. | |
| Relative Contraindications | High-demand athletics / Heavy manual labor | Risk of premature failure, tissue degradation, or instability. |
| Long second metatarsal | High risk of post-operative transfer metatarsalgia. | |
| Moderate osteopenia | May compromise drill hole integrity for flap fixation. | |
| Absolute Contraindications | Peripheral Neuropathy (e.g., Diabetic) | Inability to protect the joint; risk of Charcot breakdown. |
| Severe Peripheral Arterial Disease | Inadequate perfusion for complex soft-tissue healing. | |
| Active local or systemic infection | Risk of deep space surgical site infection. | |
| Inadequate dorsal capsular tissue | Previous aggressive surgeries leaving no tissue for the flap. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning dictates our surgical strategy and helps us anticipate intraoperative challenges before the first incision is made. Radiographic evaluation is the cornerstone of this process. We must obtain standard weight-bearing anteroposterior (AP), oblique, and lateral radiographs of the foot, along with an axial sesamoid view. These views are crucial for assessing the degree of joint space narrowing, the location and size of osteophytes, and the presence of subchondral cysts.

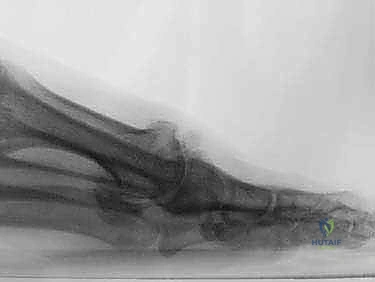
During templating, pay close attention to the relative lengths of the first and second metatarsals on the AP radiograph. As previously discussed, a long second metatarsal is a red flag for potential transfer metatarsalgia following first ray shortening. Additionally, evaluate the shape of the metatarsal head; a severely flattened metatarsal head may require more extensive contouring to restore a functional articulation. The lateral radiograph is invaluable for assessing the dorsal osteophytes and the extent of dorsal joint space narrowing, which dictates the volume of bone we must resect during the initial cheilectomy phase.
Precision in patient positioning ensures optimal surgical exposure and seamless fluoroscopic access. The patient is placed supine on the operating table. A bolster is placed under the greater trochanter of the ipsilateral hip to prevent external rotation of the operated extremity, ensuring the foot rests in a neutral or slightly internally rotated position. If necessary, a small bump can be placed under the contralateral lumbar region to subtly evert the operative foot, significantly improving access to the medial aspect of the first MTP joint. The foot is positioned at the extreme bottom corner of the bed, allowing ample space for the surgical team and equipment to maneuver without breaking sterility.
Anesthesia and hemostasis must be meticulously managed. We typically utilize a comprehensive ankle block anesthesia, which provides excellent, long-lasting pain control and regional muscle relaxation, minimizing the need for deep systemic anesthetic agents. For hemostasis, a sterile Esmarch ankle tourniquet is applied. We use three tight wraps, aiming for a pressure approximating 300 mmHg. Crucially, a full roll of Webril must be wrapped around the ankle underneath the Esmarch to protect the skin, the superficial nerves, and the underlying Achilles tendon from excessive, concentrated pressure and potential crush injury.
Step-by-Step Surgical Approach and Fixation Technique
Alright, the patient is prepped and draped, the ankle block is mature, and the tourniquet is up. It is time to execute. We will be utilizing a medial approach, which I find vastly superior for this specific procedure as it grants exceptional access to the plantar structures necessary for securing the interpositional flap.
Incision and Deep Dissection
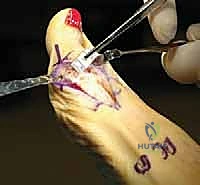
I begin with a longitudinal midaxial medial incision centered directly over the first MTP joint. This curvilinear incision should be approximately 4 to 5 cm in length, extending from the mid-diaphysis of the first metatarsal to the mid-diaphysis of the proximal phalanx.
As we deepen the incision through the skin and subcutaneous tissue, extreme vigilance is required. We must be acutely aware of the dorsomedial sensory cutaneous nerve to the hallux. This nerve lies superficially in this exact region and is highly vulnerable to sharp transection or aggressive retraction. I use careful, blunt dissection with a Metzenbaum scissors or a small hemostat to spread the subcutaneous fat, identify the nerve, and gently mobilize it.

Once identified, the nerve is retracted gently, usually dorsally, using a small Senn or Ragnell retractor. We must avoid excessive tension, which can cause a traction neuropraxia. With the nerve protected, we continue our dissection down to the level of the joint capsule, clearing the overlying areolar tissue to expose the robust, often thickened, capsuloligamentous complex of the medial first MTP joint.
Capsulotomy and Joint Debridement
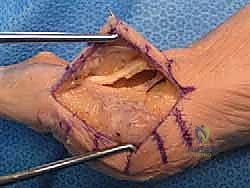
The capsulotomy is a critical step, as we are simultaneously exposing the joint and defining the margins of our future interpositional flap. I perform a dorsal and medial capsulotomy, starting proximally on the metatarsal neck and extending distally to the base of the proximal phalanx.

We carefully elevate the dorsal capsule off the underlying dorsal osteophytes. This tissue is often adherent and requires sharp dissection with a #15 blade. We must preserve as much length and thickness of this dorsal capsule as possible, as it will form the bulk of our interpositional material. Once the capsule is reflected dorsally and plantarly, we gain full visualization of the arthritic joint.

The extent of the degenerative changes is usually profound. We proceed with a comprehensive cheilectomy. Using a combination of a sagittal saw and a rongeur, I resect the prominent dorsal, medial, and lateral osteophytes from the metatarsal head. The goal here is not just to remove the mechanical block to dorsiflexion, but to contour the metatarsal head back to a smooth, rounded shape that will articulate favorably with our soft-tissue flap.

Phalangeal Resection and Joint Preparation
With the metatarsal head decompressed, we turn our attention to the proximal phalanx. The core of the interpositional arthroplasty relies on creating adequate joint space to accommodate the soft tissue flap without over-stuffing the joint. Using a sagittal saw, I resect the articular base of the proximal phalanx.

The cut is made perpendicular to the long axis of the phalanx in both the AP and lateral planes. Typically, a resection of 3 to 5 millimeters of bone is sufficient. It is absolutely critical to avoid resecting too much bone plantarly; we must preserve the insertion of the flexor hallucis brevis (FHB) onto the plantar base of the phalanx. If the FHB insertion is completely violated, the patient will inevitably develop a disastrous cock-up deformity. After the resection, I use a rongeur and a rasp to smooth the edges of the cut phalangeal surface, ensuring no sharp bony spicules remain to abrade the interpositional flap.
Interpositional Flap Harvest and Mobilization
Now we prepare the biological spacer. We utilize the previously elevated dorsal capsule, but to provide adequate bulk and length, we augment it with the Extensor Hallucis Brevis (EHB) tendon. I identify the EHB tendon dorsally, running deep and slightly lateral to the EHL.

The EHB is transected approximately 3 to 4 centimeters proximal to the joint line. We then mobilize the EHB tendon distally, leaving its insertion onto the proximal phalanx intact. This mobilized tendon is then sutured to the deep surface of our dorsal capsular flap using a 2-0 absorbable suture, creating a thick, robust, composite soft-tissue spacer.

This composite flap (capsule + EHB) is now hinged distally at the base of the proximal phalanx. We verify that the flap has sufficient length to be draped over the resected phalangeal base and tucked deep into the joint space, reaching the plantar plate.
Flap Inset and Fixation
The fixation of the flap is the most technically demanding portion of the procedure. We must secure the dorsal flap to the plantar structures to ensure it remains interposed during active range of motion. First, I drill two or three small longitudinal holes through the dorsal cortex of the remaining proximal phalanx, exiting at the resected articular surface.

Next, we place heavy, non-absorbable sutures (such as 2-0 FiberWire or equivalent) into the free proximal edge of our composite capsular flap. Using a suture passer or a Keith needle, these suture limbs are passed from dorsal to plantar, through the joint space, and then driven through the robust plantar plate and the stumps of the FHB tendon.

This step requires extreme caution to avoid ensnaring the FHL tendon or the plantar digital nerves. Once the sutures are passed through the plantar structures, they are routed back dorsally through the previously drilled bony tunnels in the proximal phalanx.

While an assistant holds the toe in approximately 10 to 15 degrees of dorsiflexion and applies slight axial traction to open the joint space, I tie the sutures securely over the dorsal bony bridge of the phalanx. This maneuver draws the capsular flap deep into the joint, covering the denuded metatarsal head and the resected phalangeal base, effectively resurfacing the articulation.
Closure and Final Alignment
With the flap securely inset, we assess the joint. The MTP joint should now have a smooth, unencumbered range of motion, free of crepitus or impingement. The medial capsule is then closed over the joint using 2-0 or 3-0 absorbable sutures, ensuring the EHL tendon remains centralized and un-tethered.

The subcutaneous tissues are closed in layers, and the skin is approximated with a running subcuticular suture or nylon mattress sutures. A bulky, compressive soft dressing is applied, utilizing a specialized taping technique to hold the great toe in slight plantarflexion. This taping is critical; it neutralizes the pull of the EHL and prevents the dorsal capsular flap from being pulled out of the joint space during the early healing phase.


Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications can and do occur. The most feared complication specific to this procedure is the "cock-up" toe deformity, characterized by fixed hyperextension at the MTP joint and flexion at the IP joint. This occurs due to the loss of the intrinsic plantarflexory power of the flexor hallucis brevis (FHB), usually resulting from over-resection of the plantar base of the proximal phalanx or failure to adequately secure the plantar plate during closure. If a severe cock-up deformity develops, conservative management inevitably fails, and surgical salvage via an interphalangeal joint fusion and MTP joint arthrodesis or flexor-to-extensor tendon transfer is required.
Transfer metatarsalgia, specifically under the second metatarsal head, is another significant complication, occurring in roughly 10-15% of patients. By resecting the base of the proximal phalanx, the first ray is inherently shortened, decreasing its weight-bearing capacity. The load is subsequently transferred laterally to the lesser metatarsals. This risk is exponentially higher in patients with a pre-existing long second metatarsal. Management begins with custom orthotics featuring a metatarsal pad and a Morton's extension; however, recalcitrant cases may necessitate a second metatarsal shortening osteotomy (Weil osteotomy).
Neurovascular injuries, while rare, carry high morbidity. Injury to the dorsomedial sensory cutaneous nerve during the surgical approach results in a painful neuroma or persistent numbness over the medial hallux. If a neuroma forms and fails conservative management (injections, desensitization), surgical excision and burying
