Moberg Osteotomy & Cheilectomy: A Masterclass in Hallux Rigidus Correction

Key Takeaway
This masterclass provides an exhaustive, immersive guide to the Moberg osteotomy and concomitant cheilectomy for hallux rigidus. As your scrubbed-in instructor, we'll navigate comprehensive surgical anatomy, meticulous preoperative planning, and granular intraoperative execution. Learn critical pearls, pitfalls, and strategies for complication management, ensuring optimal outcomes for patients suffering from this debilitating condition. Master the art of restoring MTP joint function.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater, colleagues. Today, we are undertaking an exhaustive review of a common, yet frequently mismanaged, and often debilitating condition: Hallux Rigidus. This degenerative arthritic condition affects the first metatarsophalangeal (MTP) joint and is characterized by a progressive, insidious loss of motion, particularly in the sagittal plane of dorsiflexion. While it can occasionally mimic other systemic inflammatory conditions such as gout, pseudogout, or rheumatoid arthritis, the idiopathic osteoarthritic form remains overwhelmingly the most prevalent. Epidemiological data suggests it affects approximately 3% of the general adult population, with a significantly higher incidence observed in women and a strong propensity for bilateral presentation over the patient's lifetime.
Patients typically present to the clinic with an insidious onset of activity-related pain, localized swelling, and progressive stiffness at the first MTP joint. The hallmark physical examination finding is a measurably limited passive and active dorsiflexion, which is mechanically blocked by a prominent dorsal osteophyte on the first metatarsal head, often accompanied by an abutting osteophyte or ossicle on the dorsal base of the proximal phalanx. Furthermore, pain can frequently be elicited with forceful plantarflexion as the inflamed, hypertrophic synovium impinges against these dorsal osteophytes. This functional limitation profoundly impacts daily kinematics, interfering with terminal stance phase during the gait cycle, running, walking on inclines, and the accommodation of standard footwear, particularly dress shoes or high heels.
The increasing dorsal prominence not only acts as a mechanical block but also leads to direct, painful shoe-wear irritation. In rare but clinically significant instances, the compression of the dorsal cutaneous nerves by these expanding osteophytes or tightly constricting shoes can precipitate paresthesias and neuropathic pain distal to the MTP joint. Historically, the surgical management of this condition was heavily weighted toward joint-sacrificing procedures. However, the paradigm shifted significantly with the popularization of joint-preserving techniques.
The Moberg osteotomy, initially described as a dorsal closing wedge osteotomy of the proximal phalanx base, was conceptualized to directly address this functional dorsiflexion deficit. While Erik Moberg initially advocated this procedure primarily for younger, active patients, contemporary indications have broadly expanded to include middle-aged and older adults with preserved joint space. Crucially, as orthopedic surgeons, we must understand that the Moberg osteotomy is almost never executed as an isolated, standalone procedure. We routinely and necessarily perform it in conjunction with a comprehensive cheilectomy. The cheilectomy directly addresses the primary pathoanatomy by resecting the impinging dorsal osteophytes. The Moberg osteotomy subsequently augments the kinematic effect of the cheilectomy by effectively "stealing" motion from the arc of plantarflexion and "giving" it to the arc of dorsiflexion. This extra-articular reorientation of the phalangeal articular surface dramatically improves the functional range of motion required for a normal, pain-free gait cycle.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, a profound mastery of the critical anatomy of the first MTP joint is non-negotiable. This complex articulation is unforgiving to imprecise surgical technique, and a thorough anatomical understanding is paramount for safe exposure, precise osteotomy, and the prevention of devastating iatrogenic complications.
Osteology of the First Ray
The first metatarsal head presents a convex, cam-shaped articular surface that is morphologically broader medially than laterally. In the setting of hallux rigidus, the pathoanatomy is characterized by progressive articular cartilage erosion, subchondral sclerosis, and florid osteophyte formation, predominantly localized to the dorsal and lateral aspects of the metatarsal head. The corresponding proximal phalanx base features a concave articular surface. Dorsal osteophytes, or occasionally distinct intra-articular ossicles, routinely form at this dorsal phalangeal margin, creating a "kissing lesion" that acts as a rigid mechanical block to terminal extension.
The sesamoid complex comprises two small, functionally vital bones—the tibial (medial) and fibular (lateral) sesamoids. These are intimately embedded within the tendinous slips of the flexor hallucis brevis (FHB) muscle and articulate within distinct longitudinal grooves on the plantar aspect of the first metatarsal head, separated by the crista. They form an integral component of the MTP joint complex, acting as a fulcrum to increase the mechanical advantage of the flexor hallucis longus (FHL), absorbing weight-bearing forces, and protecting the FHL tendon. While the sesamoids are not directly altered during a Moberg osteotomy, preserving their structural integrity, articular congruity, and precise anatomical position is vital for maintaining overall forefoot biomechanics and preventing postoperative sesamoiditis.
The vascular supply to the first metatarsal head is another critical osteological consideration. It is primarily perfused by an extraosseous arterial ring supplied by the first dorsal metatarsal artery and the first plantar metatarsal artery. The capsular branches enter the metatarsal head predominantly at the anatomical neck. Overly aggressive soft tissue stripping during capsulotomy and cheilectomy, particularly on the plantar-lateral aspect, can theoretically compromise this blood supply, precipitating avascular necrosis of the metatarsal head—a catastrophic complication that mandates meticulous, tissue-respecting surgical technique.
Soft Tissue Structures and Neurovascular Risks
The soft tissue envelope surrounding the first MTP joint is dense and functionally dynamic. Dorsally, the extensor hallucis longus (EHL) tendon traverses the joint space to insert on the base of the distal phalanx. During our standard dorsomedial surgical approach, the EHL must be carefully mobilized and retracted laterally. Because it lies immediately superficial to the dorsal joint capsule, it is highly susceptible to iatrogenic laceration, particularly during the aggressive use of oscillating saws for the dorsal cheilectomy and the proximal phalanx osteotomy.
Plantarly, the flexor hallucis longus (FHL) tendon is the primary dynamic stabilizer against dorsal subluxation and is essential for powerful toe-off during gait. During the execution of the proximal phalanx osteotomy, the surgeon must meticulously expose the plantar cortex and protect the FHL tendon. If the saw blade breaches the plantar cortex uncontrolled, it can easily violate the FHL tendon sheath or sever the tendon entirely, leading to a profound and largely irreversible loss of active plantarflexion and a destabilized "floating toe."
The neurovascular anatomy demands the highest level of vigilance. The dorsomedial cutaneous nerve, a terminal sensory branch originating from the superficial peroneal nerve, courses longitudinally along the dorsomedial aspect of the first metatarsal and proximal phalanx. This nerve is exceptionally vulnerable during the initial skin incision and superficial dissection. Iatrogenic transection, crushing, or aggressive traction can result in the formation of intractable, painful neuromas, or debilitating paresthesias over the dorsum of the great toe. The medial plantar nerve, while located deeper and more plantarly, provides terminal digital branches that innervate the plantar aspect of the hallux. While less commonly injured during a dorsal approach, excessively deep plantar retractors can induce neuropraxia.
Surgical Warning: The anatomical course of the dorsomedial cutaneous nerve is notoriously variable. The surgeon must operate under the assumption that it is present, superficial, and directly in the path of the incision. Meticulous sharp and blunt spreading dissection is mandatory to isolate and protect this structure before any significant retraction is applied. A postoperative neuroma often completely overshadows a technically perfect osteotomy.
Exhaustive Indications and Contraindications
Patient selection is the absolute determinant of success in joint-preserving surgery for hallux rigidus. The Moberg osteotomy combined with cheilectomy is not a panacea for all stages of degenerative joint disease; it requires a nuanced understanding of clinical grading systems and patient-specific functional demands.
The ideal surgical candidate is a patient presenting with Coughlin and Shurnas Grade I or Grade II hallux rigidus. These patients demonstrate mild to moderate radiographic joint space narrowing, primarily localized to the dorsal aspect, with a preserved plantar joint space. Clinically, their pain is highly specific—it occurs predominantly at the extremes of dorsiflexion, directly correlating with the mechanical impingement of the dorsal osteophytes. They have failed rigorous conservative management, including rigid Morton's extensions, rocker-bottom shoe modifications, intra-articular corticosteroid injections, and NSAID therapy.
Conversely, patients with Coughlin and Shurnas Grade III hallux rigidus represent a clinical gray area. While some highly active patients with Grade III disease may benefit from a cheilectomy and Moberg osteotomy to delay arthrodesis, they must be extensively counseled regarding the higher risk of persistent pain and the potential need for future fusion. Grade IV hallux rigidus, characterized by global joint space obliteration, severe constant pain throughout the entire arc of motion, and pain at the mid-range of motion, is an absolute contraindication for this joint-preserving procedure.
Other absolute contraindications include active local or systemic infection, severe inflammatory arthropathies (e.g., active rheumatoid arthritis) where the joint destruction is global and progressive, and profound neurovascular compromise of the affected limb. Relative contraindications include severe osteopenia, which may compromise hardware fixation, and significant concomitant forefoot deformities, such as severe hallux valgus, which may require a more complex, multi-planar corrective osteotomy rather than a simple sagittal plane Moberg.
| Clinical Parameter | Indications for Moberg & Cheilectomy | Contraindications for Moberg & Cheilectomy |
|---|---|---|
| Coughlin/Shurnas Grade | Grade I, Grade II, select early Grade III | Grade IV (Global joint space loss) |
| Pain Characteristics | Pain strictly at terminal dorsiflexion | Constant pain, pain at mid-range of motion |
| Radiographic Findings | Preserved plantar joint space, dorsal osteophytes | Complete joint space obliteration, cystic changes |
| Underlying Pathology | Idiopathic osteoarthritis, post-traumatic (mild) | Severe Rheumatoid Arthritis, active gouty arthropathy |
| Previous Treatments | Failed conservative shoe wear modifications, injections | Active local soft tissue or bone infection |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough, systematic preoperative planning is the bedrock upon which a flawless surgical execution is built. The margin for error in small bone osteotomies is minimal, and rigorous preparation mitigates intraoperative surprises.
Comprehensive Imaging and Templating
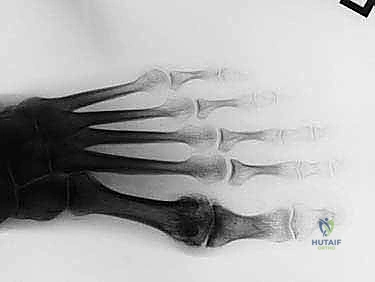
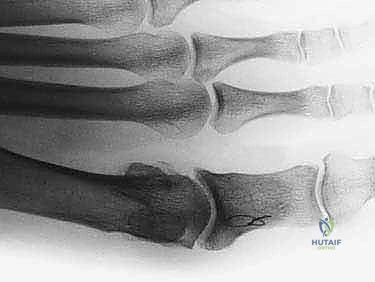
The standard imaging protocol mandates weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the affected foot. The lateral projection is our primary diagnostic tool for assessing the morphological size, location, and extent of the dorsal osteophytes on both the metatarsal head and the proximal phalanx. Weight-bearing views are absolutely critical; non-weight-bearing films passively plantarflex the hallux, which artificially opens the dorsal joint space, obscures the true extent of impingement, and frequently leads to an underestimation of the arthritic severity.
The AP view is utilized to critically evaluate the medial and lateral joint gutters for joint space narrowing and the presence of marginal osteophytes. Surgeons must be cognizant that large, overhanging dorsal osteophytes can project over the joint line on an AP radiograph, creating a radiographic illusion of severe joint space collapse when the true articular cartilage may still be viable. While advanced imaging like MRI or CT is not routinely indicated, it becomes invaluable when subtle osteochondral lesions of the metatarsal head are suspected, or when the severity of pain is disproportionate to the radiographic findings.

Preoperative templating, while less formalized than in total joint arthroplasty, is a vital mental and physical exercise. The surgeon must estimate the required size of the dorsal closing wedge to achieve the desired functional outcome. Typically, a 3 to 5-millimeter wedge base is planned, aiming to dorsiflex the phalanx by approximately 15 to 20 degrees. The goal is to restore a functional arc of 60 to 70 degrees of dorsiflexion relative to the first metatarsal, which is the biomechanical prerequisite for a normal, uncompensated terminal stance phase of gait.

Patient Positioning and Anesthesia Protocols
The procedure is highly amenable to regional anesthesia, typically performed under a comprehensive ankle block. This technique provides profound regional analgesia and motor blockade, drastically minimizing the requirement for volatile systemic anesthetics and postoperative narcotics. The ankle block systematically targets the deep peroneal, superficial peroneal, saphenous, sural, and posterior tibial nerves. This regional approach frequently allows for a highly tolerable tourniquet time for the conscious or lightly sedated patient.
The patient is positioned supine on the operating table. The operative extremity is meticulously prepped and draped in a standard sterile fashion, typically extending from the mid-calf down to the toes, allowing full manipulation of the foot and ankle. A Martin-type exsanguinating tourniquet, or a standard pneumatic tourniquet, is applied to the supramalleolar region of the ankle over adequate soft padding. Achieving a perfectly bloodless surgical field is not merely a convenience; it is a strict requirement for the precise identification of the cutaneous nerves and the meticulous execution of the osteotomy cuts.
A mini C-arm fluoroscopy unit is an indispensable tool for this procedure. It must be positioned, draped sterilely, and tested prior to the incision to ensure it can easily capture true AP and lateral views of the first MTP joint without requiring awkward repositioning of the patient's limb. Finally, weight-based prophylactic intravenous antibiotics (typically a first-generation cephalosporin) are administered within 60 minutes prior to tourniquet inflation, strictly adhering to institutional antimicrobial stewardship protocols.
Step-by-Step Surgical Approach and Fixation Technique
We are now scrubbed, the patient is optimally positioned, anesthetized, and the surgical field is sterile. The execution of the Moberg osteotomy and cheilectomy requires a symphony of precise soft tissue handling and aggressive, yet controlled, bony resection.
I. The Surgical Approach and Exposure
The primary objective of the approach is to achieve wide, unhindered exposure of the dorsal and lateral aspects of the MTP joint while strictly preserving the neurovascular envelope.
- Incision and Superficial Dissection: Begin by palpating the anatomical landmarks: the medial eminence of the first metatarsal head and the base of the proximal phalanx. Using a #15 scalpel blade, execute a longitudinal dorsomedial skin incision, perfectly centered over the first MTP joint. The incision should span approximately 4 to 5 centimeters, originating at the distal third of the first metatarsal diaphysis and extending distally to the mid-diaphysis of the proximal phalanx.

- Nerve Identification and Protection: Immediately upon breaching the dermis, discard the scalpel. Utilize meticulous, blunt spreading dissection with delicate tenotomy scissors or a small hemostat. The immediate goal is the visual identification of the dorsomedial cutaneous nerve. It routinely courses superficial to the EHL tendon sheath. Once positively identified, it must be gently mobilized and retracted—typically medially—using a soft silicone vessel loop or a blunt Senn retractor.

-
Capsular Exposure: Deepen the dissection through the subcutaneous adipose layers to expose the extensor hallucis longus (EHL) tendon. The EHL is mobilized from its tendon sheath and retracted laterally using a small Hohmann retractor. This lateral retraction is critical as it protects the tendon and exposes the direct dorsal and dorsolateral aspects of the MTP joint capsule, which is the primary site of our intended bony work.
-
MTP Capsulotomy: Execute a robust, linear capsulotomy directly in line with the initial skin incision, traversing the dorsomedial aspect of the joint. Before proceeding further, utilize 2-0 absorbable sutures (e.g., Vicryl) to place tagging stitches in the dorsal and plantar-medial capsular edges. This seemingly minor step is invaluable during closure, as the capsule tends to retract and become difficult to identify after extensive bony resection.

II. The Cheilectomy Phase
With the capsule tagged and retracted, the joint is fully exposed. The cheilectomy must be aggressive enough to remove all impingement but conservative enough to preserve joint stability.
- Osteophyte Resection: Identify the prominent dorsal osteophyte on the metatarsal head. Using a micro-sagittal saw or a sharp osteotome, resect the osteophyte along with the dorsal 20% to 30% of the metatarsal head. The cut should be angled slightly obliquely, from dorsal-distal to plantar-proximal, ensuring the resection is flush with the native dorsal metatarsal shaft.

- Phalangeal Debridement: Direct attention to the base of the proximal phalanx. Resect any corresponding dorsal osteophytes or loose intra-articular ossicles that contribute to the "kissing lesion" impingement.

- Joint Debridement and ROM Check: Use a rongeur and curette to meticulously debride the medial and lateral gutters of any hypertrophic synovium or marginal osteophytes. Following the cheilectomy, temporarily relocate the joint and assess the passive range of motion. You should note a marked improvement in dorsiflexion, free of hard bony blocks. If impingement persists, further resection is mandated.
III. The Moberg Osteotomy Phase
The cheilectomy removes the block; the Moberg osteotomy reorients the functional arc of motion.
-
Marking the Wedge: On the dorsal aspect of the proximal phalanx, approximately 5 to 8 millimeters distal to the articular surface (to preserve the capsular attachments and intra-articular congruity), mark the planned dorsal closing wedge. The base of the wedge is dorsal, typically measuring 3 to 5 millimeters, tapering to an apex at the plantar cortex.
-
Executing the Osteotomy: Utilizing a fine micro-sagittal saw, make the distal cut first, perpendicular to the long axis of the phalanx. Next, make the proximal cut, angling it distally to meet the first cut at the plantar cortex. Crucial Step: Place a small Freer elevator or a miniature Hohmann retractor subperiosteally along the plantar cortex to absolutely protect the underlying FHL tendon from the saw blade.

- Completing the Wedge: Carefully remove the dorsal bony wedge. It is highly preferable to leave a paper-thin hinge of intact plantar cortex. This intact hinge acts as a tension band, providing immense intrinsic stability to the osteotomy and facilitating anatomical closure of the wedge. If the plantar cortex is inadvertently breached, the osteotomy becomes inherently unstable and requires more robust fixation.

- Osteotomy Closure and Fixation: Manually close the osteotomy by dorsiflexing the distal phalanx. The bone ends should oppose flushly. Fixation can be achieved via multiple modalities. A common and highly effective method utilizes a single, dorsally placed staple or a headless compression screw. Alternatively, smooth K-wires can be utilized.

If using a screw, guide wire placement is critical to ensure it crosses the osteotomy perpendicular to the cut and achieves purchase in the plantar-proximal fragment without violating the MTP joint.

Verify the final hardware position and the restored range of motion under multi-planar fluoroscopy.


- Closure: Thoroughly irrigate the wound to remove all bone debris. Repair the MTP joint capsule using the previously placed tagging sutures. The EHL is allowed to fall back into its anatomical position. Close the subcutaneous tissue and skin meticulously. Apply a sterile, mildly compressive dressing.
Complications, Incidence Rates, and Salvage Management
While the Moberg osteotomy with cheilectomy is highly successful when properly indicated, it is not immune to complications. A profound understanding of potential pitfalls is required for rapid identification and salvage.
Intraoperative complications are primarily iatrogenic. The most devastating is the laceration of the flexor hallucis longus (FHL) tendon during the plantar completion of the phalangeal osteotomy. This results in an immediate loss of active hallux plantarflexion and a destabilized toe. If identified intraoperatively, immediate primary tendon repair is mandatory. Similarly, iatrogenic injury to the dorsomedial cutaneous nerve can lead to intractable postoperative neuromas. Prevention through meticulous
