Flexion Intertrochanteric Osteotomy for Severe Slipped Capital Femoral Epiphysis: An Intraoperative Masterclass

Key Takeaway
This masterclass details the flexion intertrochanteric osteotomy for severe slipped capital femoral epiphysis (SCFE). We cover comprehensive surgical anatomy, meticulous preoperative planning, and a granular, step-by-step intraoperative execution from the surgeon's perspective. Critical pearls, potential pitfalls, and a robust postoperative rehabilitation protocol are extensively discussed, ensuring fellows gain a deep understanding of this complex hip realignment procedure.
Comprehensive Introduction and Patho-Epidemiology
The Biomechanical Pathogenesis of SCFE
Slipped Capital Femoral Epiphysis (SCFE) represents one of the most mechanically complex and biologically precarious pathologies encountered in adolescent orthopedics. At its core, the condition is characterized by a structural failure through the hypertrophic zone of the proximal femoral physis. This failure leads to a predictable, three-dimensional displacement: the femoral neck translates anteriorly, superiorly, and externally rotates relative to the capital epiphysis, which remains seated within the acetabulum. While the exact etiology is multifactorial, the interplay between endocrine fluctuations during the adolescent growth spurt and mechanical overload is undeniable. The transition from a horizontally oriented juvenile physis to a more vertically oriented adolescent physis significantly increases the shear stresses across the growth plate, particularly in the context of childhood obesity, which exponentially magnifies joint reactive forces.
The resultant deformity fundamentally alters the biomechanics of the hip joint. As the epiphysis slips posteriorly and inferiorly, the anterior metaphysis of the femoral neck becomes prominent. This creates the classic "pistol-grip" deformity, characterized by a loss of the normal concave anterior contour of the femoral head-neck junction. This profound morphological alteration is not merely an anatomical curiosity; it is the primary driver of subsequent joint destruction. The prominent anterior metaphysis acts as a cam lesion, forcefully abutting against the anterosuperior acetabular rim and labrum during terminal hip flexion and internal rotation. This repetitive, high-energy impact initiates a cascade of chondrolabral damage, leading to early-onset, rapidly progressive secondary osteoarthritis if left unaddressed.
Understanding this pathoanatomy is crucial for the operating surgeon. The displacement is rarely uniplanar; it is a complex triplanar deformity involving varus, retroversion, and extension of the femoral head relative to the shaft. Consequently, any corrective surgical intervention must address all three planes of deformity to restore normal hip kinematics. The historical reliance on isolated in-situ fixation, while effective at preventing further slippage, frequently leaves the patient with a profound residual deformity and obligatory femoroacetabular impingement (FAI). It is this precise mechanical conflict that the flexion intertrochanteric osteotomy seeks to resolve.
Clinical Presentation and the Genesis of Impingement
Patients harboring a severe, healed SCFE present with a highly characteristic clinical picture that directly reflects their underlying bony morphology. The hallmark of this condition is an obligate external rotation gait. Because the femoral neck has externally rotated relative to the head during the slippage process, the patient must externally rotate the entire lower extremity to achieve a neutral position of the femoral head within the acetabulum during the stance phase of gait. This compensatory mechanism severely limits internal rotation, which is often completely absent or even negative (obligate external rotation) when the hip is flexed to 90 degrees.

Pain is typically insidious in onset, frequently localized to the groin, but classically referred to the anteromedial thigh or knee via the obturator nerve. This referred pain pattern is a notorious trap for the unwary clinician, often leading to delayed diagnosis and prolonged periods of mechanical damage to the hip joint. On physical examination, the Drehmann sign is almost universally positive: as the hip is passively flexed, it obligatorily falls into external rotation and abduction to clear the prominent anterior metaphyseal bump from the acetabular rim. True hip flexion is dramatically restricted, often to less than 80 or 90 degrees, and any attempt to force internal rotation in flexion elicits sharp, reproducible anterior groin pain indicative of acute cam impingement.
The long-term natural history of untreated or subclinical SCFE with residual deformity is grim. Landmark epidemiological and radiographic studies by Murray, Aronson, and Ganz have definitively established the causal link between the pistol-grip deformity of SCFE and the development of idiopathic osteoarthritis of the hip. The abnormal contact mechanics lead to early labral tearing, delamination of the adjacent acetabular cartilage, and eventual global joint space narrowing. Therefore, the goal of surgical intervention in a symptomatic, deformed, healed SCFE is not merely symptomatic relief, but joint preservation through the restoration of impingement-free kinematics.
The Rationale for Flexion Intertrochanteric Osteotomy
The modern surgical management of severe, healed SCFE deformity often requires a comprehensive, two-stage intraoperative approach. The first stage typically involves a surgical hip dislocation (SHD) as described by Ganz. This allows for direct, 360-degree visualization of the femoral head and neck, permitting an aggressive osteochondroplasty to remove the anterior metaphyseal bump and restore the spherical contour of the head-neck junction. However, in cases of severe slips (typically those exceeding a Southwick angle of 50-60 degrees), an intracapsular osteochondroplasty alone is insufficient. The degree of posterior and inferior displacement is so profound that attempting to re-create a normal offset intracapsularly would compromise the structural integrity of the femoral neck or risk devascularization.
When intracapsular correction reaches its limits and significant mechanical impingement persists, we must transition to an extracapsular, multiplanar realignment: the flexion intertrochanteric osteotomy (often referred to historically as the Imhäuser osteotomy). The rationale here is elegant in its biomechanical logic. By performing an osteotomy at the intertrochanteric level, we can reorient the entire proximal femoral segment (head and neck) relative to the femoral shaft. To counteract the posterior slip, we flex the proximal fragment. To counteract the inferior slip (varus), we valgus the proximal fragment. To counteract the external rotation deformity, we internally rotate the distal shaft.
This triplanar correction—flexion, valgus, and internal rotation—effectively repositions the articular cartilage of the femoral head into the weight-bearing dome of the acetabulum while simultaneously rotating the residual anterior metaphyseal prominence away from the critical anterosuperior impingement zone. Because the osteotomy is performed extracapsularly, distal to the trochanteric fossa, it carries a substantially lower risk of avascular necrosis (AVN) compared to intracapsular femoral neck osteotomies (such as the Dunn procedure), making it the workhorse procedure for severe, chronic, stable SCFE deformities.
Detailed Surgical Anatomy and Biomechanics
Osteology and Proximal Femoral Geometry
Mastery of the flexion intertrochanteric osteotomy requires a profound, three-dimensional understanding of proximal femoral osteology. The surgical theater is bounded by the greater trochanter laterally, the lesser trochanter medially, and the intertrochanteric line anteriorly. The osteotomy itself is typically planned at or just proximal to the level of the lesser trochanter. This specific location is chosen because it provides a broad surface area of highly vascularized cancellous bone, ensuring rapid and robust osseous union, while remaining distal enough to avoid violating the critical superior retinacular vessels that supply the femoral head.
The geometry of the deformity dictates the geometry of our correction. In a severe SCFE, the capital epiphysis is displaced posteriorly and inferiorly. This effectively decreases the femoral neck-shaft angle (varus) and creates a profound retroversion of the femoral neck. When planning the osteotomy, the surgeon must conceptualize the proximal femur as two distinct segments: the proximal fragment (head, neck, and greater trochanter) and the distal fragment (femoral shaft). The goal is to manipulate the distal shaft to accommodate the deformed proximal fragment, thereby restoring normal alignment of the limb relative to the pelvis.
The "pistol-grip" deformity, a critical osteological landmark in this pathology, represents the widened, non-concave anterior femoral neck. During the preceding surgical hip dislocation, this area is often partially contoured. However, the intertrochanteric osteotomy leverages this remaining deformity by rotating it out of the impingement zone. By flexing the proximal fragment (or extending the distal shaft), we move the anterior neck prominence superiorly and away from the anterior acetabular rim during hip flexion. The addition of valgus improves the abductor moment arm, which is often compromised by the relative shortening of the femoral neck and superior migration of the greater trochanter inherent in severe SCFE.
Musculotendinous Intervals and Dynamic Stabilizers
The surgical approach for this procedure is a direct lateral extension of the approach utilized for the surgical hip dislocation. The primary muscular interval involves the vastus lateralis. This massive pennate muscle originates from the anterior and lateral aspects of the greater trochanter, the lateral lip of the gluteal tuberosity, and the proximal half of the linea aspera. To expose the intertrochanteric and subtrochanteric regions of the femur, the vastus lateralis must be meticulously elevated. We utilize a vastus-splitting or vastus-sparing (subvastus) technique, reflecting the muscle belly anteriorly from the lateral intermuscular septum and the vastus ridge.
Superficial to the vastus lateralis lies the iliotibial band (ITB), a thick, fascial continuation of the tensor fasciae latae and gluteus maximus. The ITB must be incised longitudinally to access the deeper muscular layers. Careful closure of the ITB at the conclusion of the procedure is paramount to restore lateral tension and prevent postoperative lateral thigh pain or snapping hip syndrome. Proximal to the osteotomy site, the abductor complex (gluteus medius and minimus) inserts onto the greater trochanter. If a trochanteric flip osteotomy was performed during the initial surgical hip dislocation, the integrity of this repair must be rigorously protected during the subsequent manipulation and fixation of the intertrochanteric osteotomy.
The dynamic stabilizers of the hip, particularly the iliopsoas tendon inserting onto the lesser trochanter, play a significant role in the biomechanics of the deformity and the correction. The severe external rotation deformity often leads to adaptive shortening of the posterior structures and the iliopsoas. While an isolated psoas release is rarely indicated, the surgeon must be aware that the internal rotation correction applied to the distal shaft will place tension on these medial structures. The robust fixation provided by a blade plate or dynamic condylar screw is necessary to counteract these deforming muscular forces during the healing phase.
Critical Neurovascular Topography
The proximal femur is surrounded by a complex and unforgiving neurovascular network. The most critical vascular structures are those supplying the femoral head, primarily the deep branch of the medial circumflex femoral artery (MFCA). The MFCA courses posteriorly, superior to the lesser trochanter, and gives rise to the superior retinacular vessels that traverse the posterosuperior aspect of the femoral neck. The absolute cardinal rule of the intertrochanteric osteotomy is to remain extracapsular and distal to the trochanteric fossa to preserve this delicate blood supply. An osteotomy that strays too proximally risks catastrophic avascular necrosis (AVN) of the femoral head.
As the vastus lateralis is reflected anteriorly off the linea aspera, the surgeon will invariably encounter a series of perforating arteries and veins. These vessels arise from the profunda femoris artery, pierce the lateral intermuscular septum, and arborize within the vastus lateralis. There are typically three to four main perforators in this region. These must be systematically identified, isolated, and ligated or heavily coagulated prior to dividing them. Failure to achieve meticulous hemostasis of the perforators will result in a massive postoperative hematoma, increased risk of infection, and profound postoperative pain.
Neurologically, the surgical field is relatively safe, provided the dissection remains within the prescribed anatomical boundaries. The sciatic nerve lies posterior to the operative field, protected by the gluteus maximus and the short external rotators. However, aggressive posterior retraction, particularly if the hip is externally rotated, can place traction on the sciatic nerve. Anteriorly, the branches of the femoral nerve supply the quadriceps. While the main trunk of the femoral nerve is far medial to the approach, vigorous anterior retraction of the vastus lateralis can occasionally cause a transient neurapraxia of the muscular branches, leading to postoperative quadriceps weakness. Careful, controlled retraction is therefore essential.
Exhaustive Indications and Contraindications
Patient Selection Criteria
The decision to proceed with a flexion intertrochanteric osteotomy is highly nuanced and requires rigorous patient selection. The ideal candidate is an adolescent or young adult with a severe, healed (stable) SCFE who presents with symptomatic femoroacetabular impingement that cannot be adequately addressed by intracapsular osteochondroplasty alone. Clinically, these patients demonstrate a profound loss of hip flexion and internal rotation, an obligate external rotation gait, and positive impingement signs. Radiographically, they typically present with a Southwick slip angle exceeding 50 to 60 degrees, indicating a severe deformity.
Timing is a critical factor. This procedure is generally reserved for patients whose physis has closed or is nearing closure, ensuring that the deformity is stable and will not progress postoperatively. It is also the procedure of choice for patients who have previously undergone in-situ pinning but continue to suffer from debilitating impingement due to the uncorrected residual deformity. In these cases, the hardware must be removed, the intracapsular pathology addressed via surgical hip dislocation, and the extracapsular alignment corrected via the osteotomy.
The primary goal in this patient population is joint preservation. Therefore, the patient must have well-preserved articular cartilage. Preoperative MRI or delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) can be invaluable in assessing the biochemical integrity of the chondral surfaces. If significant, full-thickness cartilage loss or advanced secondary osteoarthritis is already present, the joint preservation window has closed, and the patient is better served by arthroplasty.
Absolute and Relative Contraindications
Absolute contraindications to the flexion intertrochanteric osteotomy include the presence of advanced, irreversible joint destruction (Kellgren-Lawrence grade 3 or 4 osteoarthritis). In these scenarios, realigning the femur will not salvage the necrotic or severely degenerated cartilage, and a total hip arthroplasty is the definitive solution. Active joint infection or systemic sepsis is an absolute contraindication to any elective osteotomy and internal fixation. Furthermore, established avascular necrosis (AVN) of the femoral head with structural collapse is a contraindication, as the osteotomy relies on a viable femoral head to articulate with the acetabulum.
Relative contraindications revolve around patient factors and the specific nature of the deformity. An acute, unstable SCFE is generally not treated with an immediate intertrochanteric osteotomy due to the unacceptably high risk of provoking AVN during the manipulation required for positioning and fixation. These are typically managed with gentle in-situ fixation or a modified Dunn procedure. Severe obesity (BMI > 40) is a significant relative contraindication, as it drastically increases the mechanical demands on the internal fixation, elevating the risk of hardware failure, nonunion, and perioperative complications such as deep vein thrombosis and infection.
Another relative contraindication is a lack of patient compliance. The postoperative rehabilitation protocol following a complex multiplanar osteotomy is arduous, requiring strict adherence to weight-bearing restrictions and physical therapy regimens. Patients with severe cognitive impairments or those who demonstrate an inability to follow complex postoperative instructions are at a high risk for catastrophic failure of the osteotomy and may not be suitable candidates for this demanding joint preservation technique.
Decision Matrix Table
| Clinical Scenario | Primary Pathology | Recommended Intervention | Rationale / Contraindications |
|---|---|---|---|
| Mild/Moderate SCFE (<40°) | Stable slip, minimal impingement | In-situ pinning +/- Arthroscopic Osteochondroplasty | Low risk of severe FAI; osteotomy is overly aggressive. |
| Severe Healed SCFE (>50°) | Chronic impingement, preserved cartilage | SHD + Flexion Intertrochanteric Osteotomy | Triplanar deformity requires extracapsular realignment; joint preservation is viable. |
| Severe SCFE with AVN | Structural collapse of femoral head | Total Hip Arthroplasty (THA) | Joint preservation impossible; osteotomy contraindicated. |
| Acute Unstable SCFE | Physis fractured, high risk of AVN | Modified Dunn Procedure or Gentle In-situ Pinning | Immediate ITO contraindicated due to high AVN risk during manipulation. |
| Severe SCFE with Advanced OA | Joint space narrowing, osteophytes | Total Hip Arthroplasty (THA) | Cartilage is unsalvageable; realignment will not relieve arthritic pain. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging Modalities and Deformity Analysis
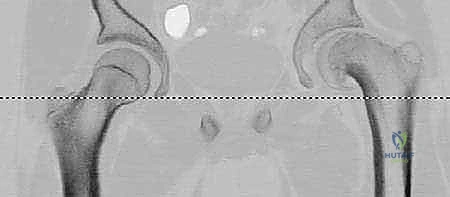
The foundation of a successful multiplanar osteotomy lies in exhaustive preoperative imaging and meticulous deformity analysis. Standard plain radiographs are the starting point. We require a true anteroposterior (AP) view of the pelvis to assess the varus deformity and a frog-leg lateral view to assess the posterior slip angle (Southwick angle). These images provide a macroscopic overview of the deformity and the overall health of the joint space. However, plain radiographs are two-dimensional representations of a three-dimensional problem and are frequently insufficient for precise surgical planning in severe cases.
Consequently, high-resolution Computed Tomography (CT) with two- and three-dimensional (3D) reconstructions is mandatory. The CT scan must encompass the entire pelvis and extend distally through the femoral condyles to accurately assess femoral version. 3D reconstructions allow the surgeon to virtually rotate the femur, visualizing the exact location and volume of the anterior metaphyseal prominence (the cam lesion) and its dynamic relationship with the acetabulum. This helps determine how much of the impingement can be addressed intracapsularly during the surgical hip dislocation and how much requires extracapsular correction via the osteotomy.

Furthermore, radial sequence MRI or CT arthrography is highly recommended to evaluate the status of the acetabular labrum and the articular cartilage. The presence of severe chondral delamination or a massive, irreparable labral tear may alter the surgical decision-making process, pushing the surgeon away from joint preservation and toward arthroplasty. The imaging data is then imported into digital templating software, which allows for precise, millimeter-accurate planning of the osteotomy cuts and hardware placement.
Precision Templating for Multiplanar Correction
Templating is not a suggestion; it is an absolute requirement. The goal of templating is to quantify the exact degrees of flexion, valgus, and internal rotation required to restore normal anatomy. We begin with the AP radiograph to determine the required valgus correction. We measure the anterior head-shaft angle on both the affected and the contralateral normal hip (assuming it is unaffected). The difference between these two angles dictates the degree of valgus that must be built into the osteotomy. If the normal side is 145 degrees and the affected side is 115 degrees, a 30-degree valgus correction is required.

Next, we utilize the true lateral or frog-leg lateral radiograph to determine the required flexion correction. We measure the lateral head-shaft angle on both sides. The degree of posterior slippage translates directly to the amount of flexion needed in the proximal fragment. For example, a 40-degree posterior slip requires a 40-degree flexion osteotomy to reorient the articular surface anteriorly into the weight-bearing zone.

Finally, the rotational correction is determined clinically by assessing the patient's obligate external rotation and radiographically via the CT scout views of the femoral neck and condyles. The sum of these three measurements dictates the choice of implant. We typically utilize a 130-degree or 90-degree angled blade plate, or a dynamic condylar screw system. The template allows us to determine the exact entry point for the seating chisel, the angle of insertion relative to the femoral shaft, and the precise level of the osteotomy cut to ensure the hardware sits flush against the lateral cortex after the deformity is reduced.
Optimal Patient Positioning and Operating Room Setup
Patient positioning is critical, as this procedure is a marathon, not a sprint, often taking several hours and involving complex, heavy manipulations of the lower extremity. The patient is placed in the full lateral decubitus position on a radiolucent operating table. Rigid stabilization is paramount. We utilize a specialized pegboard system or robust anterior and posterior pelvic supports to lock the pelvis in a true vertical orientation.
Clinical & Radiographic Imaging Archive








