Irreparable Rotator Cuff Tears: What Are Your Treatment Options?
Key Takeaway
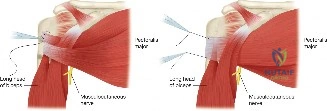
We review everything you need to understand about Irreparable Rotator Cuff Tears: What Are Your Treatment Options?. Massive, immobile rotator cuff tears, often presenting as an **irreparable rotator cuff** injury due to retraction and immobility, can be surgically repaired using specialized techniques. An anterior or posterior interval slide decreases tension and improves mobilization, allowing the supraspinatus to be reattached to the greater tuberosity. This is often followed by marginal convergence to facilitate final repair.
A 70-year-old right-hand-dominant female presents with a 6-month history of worsening shoulder pain and weakness. She reports inability to comb her hair or reach overhead. Examination reveals 30 degrees of active forward flexion, full passive range of motion, and a positive external rotation lag sign. She has no previous surgery. What is your diagnosis, and how do you differentiate this from true glenohumeral arthritis?
Candidate: The clinical picture is highly suggestive of a massive rotator cuff tear leading to pseudoparalysis. To differentiate from osteoarthritis, I would order a true AP (Grashey) view to check the acromiohumeral interval (AHI). An AHI less than 7mm suggests a massive tear, while the presence of glenohumeral joint space narrowing indicates cuff tear arthropathy.
Candidates often forget the importance of the physical exam in differentiating arthritis. They may jump immediately to an MRI. A failing candidate misses the clinical distinction that "pseudoparalysis" is defined by full passive range of motion, which is typically restricted in end-stage osteoarthritis.
The patient exhibits signs of a massive posterosuperior rotator cuff tear with pseudoparalysis. The diagnosis is confirmed by the discrepancy between limited active elevation (pseudoparalysis) and preserved passive range of motion. To differentiate from primary osteoarthritis, I would analyze the Hamada classification on a true AP radiograph. An AHI < 7mm is pathognomonic for a massive tear, whereas primary OA would show concentric joint space narrowing and osteophyte formation without the extreme superior migration of the humeral head seen in cuff tear arthropathy.
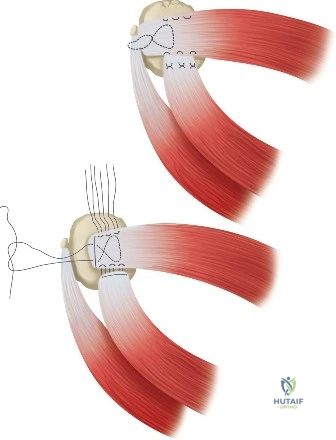
During diagnostic arthroscopy for a massive cuff tear, you find a large U-shaped tear retracted to the glenoid rim. How do you assess its "reparability," and what technical maneuvers would you employ to attempt a primary repair?
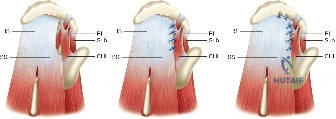
Candidate: I would grasp the tendon edges with a grasper to see if they reach the footprint without undue tension. If they don't, I would perform an anterior interval slide by releasing the coracohumeral ligament. I could also use marginal convergence to bring the leaves together.
Failure to mention the risk to the suprascapular nerve during posterior releases. A poor candidate might suggest aggressive releases without acknowledging the 1.5-2.0cm "safe zone" from the glenoid rim, putting the patient at risk for iatrogenic nerve injury.
Reparability is determined by the ability to mobilize the cuff to the tuberosity without excessive tension. I would perform a stepwise approach: 1) Bursectomy and intra-articular capsular release. 2) Anterior interval slide by incising the rotator interval and releasing the coracohumeral ligament. 3) If still tight, a posterior interval slide, being extremely cautious not to dissect medial to the glenoid rim to protect the suprascapular nerve. Finally, I would use marginal convergence to convert the U-shaped tear into a V-shape, reducing strain on the tendon-to-bone interface before final fixation.
The patient has a confirmed irreparable tear with severe atrophy. You are considering a Reverse Total Shoulder Arthroplasty (RTSA). Explain the biomechanical rationale for this implant and why it is the "gold standard" for this condition.
Candidate: The RTSA works by reversing the anatomy. It creates a new center of rotation, which allows the deltoid to lift the arm because the rotator cuff is missing. It is the gold standard for cuff tear arthropathy.
Using vague terms like "it makes the deltoid work better." A senior candidate must specifically articulate the mechanical changes: medialization and distalization of the center of rotation.
The Grammont design of the RTSA is based on medializing and distalizing the center of rotation. Medialization reduces the torque on the glenoid component, while distalization increases the tension and moment arm of the deltoid muscle. This enables the deltoid to serve as the primary elevator of the humerus, compensating for the dysfunctional rotator cuff force couples. It effectively converts a shoulder that requires a dynamic cuff into one that relies on the deltoid as a global stabilizer and motivator.
