Overlooked Tears? Advanced Treatment of Subscapularis Tears

Key Takeaway
We review everything you need to understand about Overlooked Tears? Advanced Treatment of Subscapularis Tears. Subscapularis tendon tears, often at the lesser tuberosity, impair shoulder internal rotation and stability. Due to frequent underdiagnosis, proper evaluation is vital. The treatment of subscapularis tears aims to restore functional shoulder stability, typically through arthroscopic repair. This addresses the tear and conditions like subcoracoid impingement, helping centralize the humeral head for normal motion.
Comprehensive Introduction and Patho-Epidemiology
Definition and Clinical Significance
A subscapularis tendon tear typically occurs at its insertion into the lesser tuberosity of the proximal humerus. Although the subscapularis is the largest and most powerful of the rotator cuff muscles, historically, it has received surprisingly little attention in both clinical literature and surgical practice. Subscapularis tendon tears are still often overlooked and underdiagnosed, earning the moniker of the "hidden lesion" of the shoulder. This historical oversight is largely due to the challenging arthroscopic visualization of the subscapularis footprint, which often requires specific arm positioning and the use of a 70-degree arthroscope. Consequently, a comprehensive and meticulous evaluation of the shoulder is of paramount importance to avoid missing this critical pathology.
The clinical significance of the subscapularis cannot be overstated, as it serves as the primary anterior dynamic stabilizer of the glenohumeral joint. Treatment of subscapularis tendon tears is essential to restore the functional stability and kinematics of the shoulder. When the subscapularis is compromised, the delicate balance of the glenohumeral force couples is disrupted, leading to abnormal joint mechanics, accelerated degenerative changes, and profound functional disability. Recognizing these tears early and intervening appropriately can prevent the cascade of joint deterioration that typically follows massive, unaddressed rotator cuff failures.
Furthermore, the subscapularis is intrinsically linked to the long head of the biceps tendon and the superior glenohumeral ligament complex. Pathology in the subscapularis frequently heralds or accompanies biceps instability, making isolated treatment of either structure without addressing the other a recipe for surgical failure. As arthroscopic techniques have evolved, our ability to identify, mobilize, and anatomically repair even massively retracted subscapularis tears has dramatically improved, shifting the paradigm from open, morbid procedures to elegant, minimally invasive reconstructions.
Pathogenesis and Subcoracoid Impingement
As with the other rotator cuff tendons, intrinsic factors such as age-related microvascular changes, collagen degeneration, and tenocyte apoptosis play a significant role in the development of a subscapularis tendon tear. However, extrinsic mechanical factors have been heavily implicated in the pathogenesis of these specific tears. The normal subcoracoid space, also known as the coracohumeral interval, represents the critical distance from the tip of the coracoid process to the lesser tuberosity of the proximal humerus. Anatomic and advanced imaging studies have defined the normal coracohumeral interval to be between 8.4 and 11 mm.
If this space becomes stenotic, the prominent coracoid tip will impinge against the anterior surface of the subscapularis insertion, causing repetitive mechanical damage to the tendon fibers. Subcoracoid stenosis is clinically defined as less than 6 mm of space between the coracoid and the proximal humerus, measurable by either magnetic resonance imaging (MRI) or direct arthroscopic evaluation. Patients presenting with subscapularis tears consistently demonstrate a significantly reduced coracohumeral interval—averaging 5 mm in those with subscapularis tears compared to 10 mm in matched cohorts without subscapularis pathology.
In the setting of subcoracoid impingement, the coracoid abuts against the anterior surface of the subscapularis during internal rotation and forward elevation. This abutment creates a "roller-wringer effect," causing increased tensile forces on the convex, articular (under) surface of the tendon. This mechanical disadvantage leads to progressive tendon fiber failure, typically beginning as a partial-thickness articular-sided tear. Cadaveric and clinical studies confirm that these tears almost universally initiate at the superior-most aspect of the insertion, where the tensile loads are highest, and are particularly prevalent in the elderly population.
Natural History of Subscapularis Tears
There remains a paucity of longitudinal data detailing the exact natural history of untreated subscapularis tendon tears, but clinical observation suggests a predictable pattern of progressive deterioration. What begins as a superior articular-sided partial tear slowly propagates inferiorly and superficially, eventually resulting in a complete, full-thickness detachment of the tendon from the lesser tuberosity. Once full-thickness failure occurs, the continuous pull of the massive subscapularis muscle belly leads to rapid medial retraction.

In many patients, especially those with concomitant massive posterosuperior rotator cuff tears, this progression is profoundly disabling. The loss of the anterior restraint allows for anterosuperior migration of the humeral head, permanently altering the center of rotation. Some patients with these massive, uncoupled rotator cuff tears never regain functional overhead use of their arms without surgical intervention, developing a pseudoparalytic shoulder that severely limits activities of daily living.
Interestingly, chronic tears of the subscapularis should be considered for repair even in the presence of advanced fatty degeneration and significant muscle atrophy. Unlike the supraspinatus, the subscapularis has a unique capacity to function through a "tenodesis effect." By restoring the anterior tissue envelope and re-establishing the transverse force couple, a repaired, albeit atrophic, subscapularis can still provide a stable fulcrum for the deltoid and remaining rotator cuff to elevate the arm, highlighting the critical importance of surgical intervention even in delayed presentations.
Detailed Surgical Anatomy and Biomechanics
Osseous and Musculotendinous Anatomy
A profound understanding of the subscapularis anatomy is the cornerstone of successful surgical repair. The subscapularis muscle originates from the medial two-thirds of the anterior scapular fossa, forming a massive, multipennate muscle belly. The muscle courses laterally beneath the coracoid process and becomes progressively tendinous as it crosses the anterior glenoid rim. The subscapularis tendon becomes confluent with the anterior glenohumeral joint capsule deep to it, creating a robust, inseparable tissue complex before inserting into the lesser tuberosity of the proximal humerus.
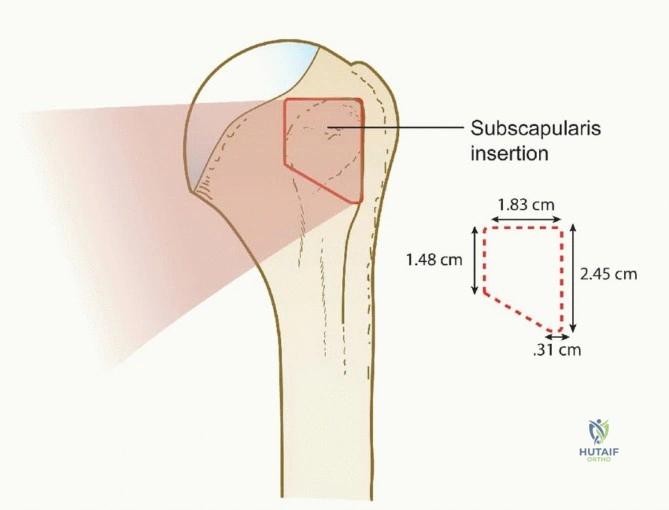
The normal subscapularis tendon not only intermingles with the fibers of the underlying joint capsule but, at its insertion, also intricately weaves with the fibers of the medial sling of the long head of the biceps tendon. The tendon insertion footprint on the lesser tuberosity is approximately 2.5 cm long (ranging from 1.5 to 3.0 cm) and is distinctly trapezoidal. The widest and thickest portion of the footprint is located at its most superior (cephalad) aspect, tapering inferiorly. This unique insertion footprint strongly resembles the shape of the state of Nevada, a useful mnemonic for anatomic footprint restoration during repair.
The superior aspect of the insertion is not only the widest but also the strongest part of the subscapularis, bearing the majority of the tensile load during active internal rotation. The muscle is innervated by the upper and lower subscapular nerves, branches of the posterior cord of the brachial plexus, which enter the muscle belly medially. Its robust blood supply is primarily derived from the subscapular artery, ensuring excellent healing potential if the tendon is adequately mobilized and securely fixed to a well-prepared bony bed.
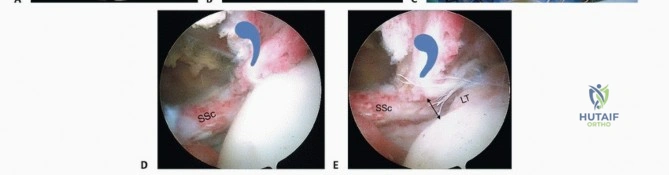
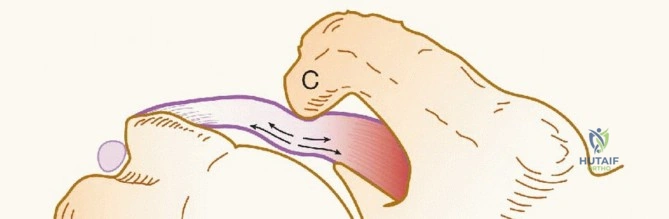
The Biceps Sling and Comma Sign
The intricate relationship between the subscapularis and the long head of the biceps tendon is defined by the medial sling. The medial sling is a critical stabilizing structure composed of fibers from the superior glenohumeral ligament (SGHL) and the coracohumeral ligament (CHL) complex. These ligaments form a pulley system that maintains the biceps tendon within the bicipital groove during shoulder motion. Disruption of the superior subscapularis inevitably compromises this medial sling, leading to medial subluxation or dislocation of the biceps tendon.
When a complete tear of the subscapularis tendon occurs, it often results in significant medial retraction of the tendon edge, sometimes retracting as far medial as the glenoid rim. As the tendon retracts, it pulls the adjacent, torn medial sling of the biceps tendon along with it. The fibers of this medial sling are oriented approximately perpendicular to the fibers of the subscapularis tendon.
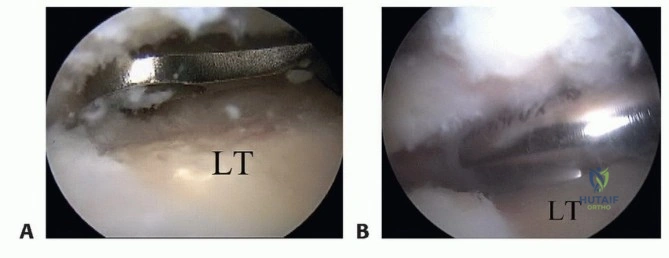
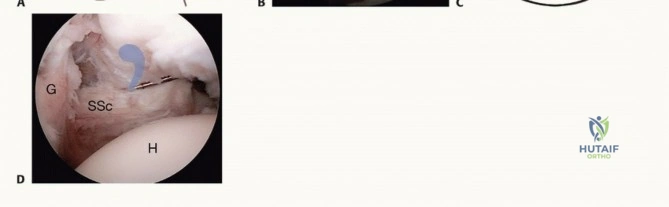
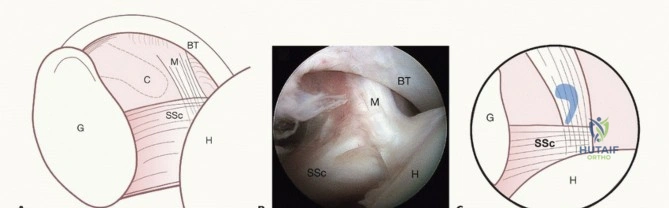
Arthroscopically, this retracted complex of the SGHL/CHL forms a distinct, thick, comma-shaped soft tissue structure located at the superolateral corner of the retracted subscapularis tendon. This is universally referred to as the "comma sign." The comma sign is an invaluable arthroscopic landmark; by identifying this structure and following it inferiorly, the surgeon is reliably led directly to the retracted superolateral edge of the subscapularis tendon, facilitating its mobilization and repair.
Biomechanics and Transverse Force Couples
The primary kinematic functions of the subscapularis muscle are to internally rotate and adduce the humerus, while simultaneously providing a dynamic anterior restraint to anterior humeral head translation. However, its most critical biomechanical role is its participation in the glenohumeral force couples. The shoulder joint relies on a delicate balance of muscular forces to maintain the humeral head centered within the shallow glenoid fossa during a wide arc of motion.
The subscapularis acts in concert with the remaining rotator cuff muscles (specifically the infraspinatus and teres minor posteriorly) to balance the transverse-plane force couple. Simultaneously, it works with the inferior cuff to balance the superior pull of the deltoid, maintaining the coronal-plane force couple. This synergistic co-contraction results in dynamic stabilization, effectively compressing and centralizing the humeral head on the glenoid.
This biomechanical phenomenon is often likened to "maintaining a golf ball on a golf tee." When the subscapularis is torn, this compressive fulcrum is lost, resulting in abnormal glenohumeral arthrokinematics. The humeral head translates anterosuperiorly, leading to secondary impingement, accelerated wear of the coracoacromial arch, and eventual cuff tear arthropathy. Restoring the subscapularis footprint is therefore not just about restoring internal rotation strength; it is about salvaging the fundamental biomechanical fulcrum of the entire shoulder joint.
Exhaustive Patient Evaluation and Diagnostic Imaging
Clinical History and Physical Examination
Diagnosing a subscapularis tear requires a high index of suspicion, as the clinical presentation can often mimic other shoulder pathologies. While most subscapularis tears seen in the community setting are degenerative in nature, the classic scenario for an acute traumatic tear involves a forced external rotation injury while the arm is abducted or adducted. This eccentric tensile load can be particularly devastating to a "tendon at risk" that has already undergone degenerative changes or is subject to subcoracoid stenosis.

In contrast to patients with typical posterosuperior rotator cuff tears, who primarily complain of difficulty with overhead tasks, patients with subscapularis tears face a different functional deficit. They often bear the burden of diminished function with tasks performed in front of the body and below the level of the shoulder. Classic complaints include an inability to open a tight jar, difficulty tucking in a shirt behind the back, or weakness when washing under the contralateral arm. The typical patient complains of chronic, deep anterior shoulder pain and a profound loss of internal rotation strength during activities of daily living.
A comprehensive physical examination is mandatory, beginning with an evaluation of the cervical spine to rule out radiculopathy. Specific provocative maneuvers for the subscapularis include:
* Lift-off test: The patient places the dorsum of their hand against their lower back and attempts to lift it away. A positive test (inability to lift the hand) indicates that at least 75% of the subscapularis tendon is torn. This test can be limited by pain or restricted internal rotation.
* Napoleon test (Modified Belly-Press): The patient presses their hand against their abdomen. If the wrist flexes to 90 degrees and the elbow drops posteriorly, the test is positive, indicating a complete tear. An intermediate test (wrist flexed 30-60 degrees) suggests more than 50% tearing. A negative test occurs when the patient can maintain a straight wrist with the elbow forward.
* Bear hug test: The patient places the palm of the affected arm on the contralateral shoulder, and the examiner attempts to pull the hand off. A positive test (inability to maintain the hand on the shoulder) is the most sensitive clinical indicator for an upper subscapularis injury, particularly partial articular-sided tears.

Advanced Imaging Modalities
Radiographic evaluation begins with a standard, high-quality plain film series. We routinely obtain five specific views of the shoulder: anteroposterior (AP) in internal rotation, AP in external rotation, a true AP (Grashey) with a 30-degree caudal tilt, a supraspinatus outlet view, and an axillary view. Plain films are scrutinized for proximal humeral migration (indicative of massive cuff failure), acromial morphology, glenohumeral or acromioclavicular joint degenerative changes, and anterior humeral translation, which is often best appreciated on the axillary view in the setting of chronic subscapularis disruption.

Magnetic Resonance Imaging (MRI) without contrast is the gold standard for evaluating the extent of subscapularis pathology. The MRI provides critical information regarding the specific location, depth, and retraction of the subscapularis tendon tear, as well as assessing the degree of fatty infiltration (Goutallier classification) within the muscle belly. Furthermore, MRI is essential for identifying coexisting pathology, such as supraspinatus tears, medial subluxation or tearing of the long head of the biceps tendon, paralabral ganglion cysts, and anterior labral tears.

Tears of the subscapularis tendon are best appreciated on the axial and sagittal oblique sequences. On axial T2-weighted images, the normal dark signal of the tendon is replaced by high signal fluid, and the coracohumeral interval can be accurately measured to assess for subcoracoid stenosis. Signal characteristics consistent with fluid extending partially through the tendon indicate partial-thickness tears, whereas a complete discontinuity and medial retraction of the tendon stump confirm a full-thickness tear. The sagittal oblique views are particularly useful for assessing the superior-to-inferior extent of the tear and the volume of the muscle belly.
Exhaustive Indications and Contraindications
Operative Rationale
The primary rationale for surgical intervention in subscapularis tears is the restoration of the anterior restraint and the re-establishment of the transverse force couple. The role of nonoperative treatment in patients with symptomatic subscapularis tears is exceedingly limited. Most patients who present to orthopedic surgeons with subscapularis tears have harbored the pathology for an extended period, and the majority have already attempted and failed exhaustive nonoperative modalities, including physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and corticosteroid injections.
For the active patient, a subscapularis tear represents a progressive biomechanical deficit that will inevitably lead to further joint destruction if left untreated. However, for patients who are exceptionally poor surgical candidates due to advanced age, severe medical comorbidities, or those who place very low functional demands on their shoulders, nonoperative management remains a viable, albeit palliative, option. In these cases, nonoperative treatment typically consists of activity modification, gentle stretching to prevent adhesive capsulitis, and progressive strengthening of the intact deltoid and periscapular musculature.
Surgical repair is indicated for acute traumatic tears in active individuals, symptomatic chronic tears that have failed conservative management, and cases where subcoracoid impingement is causing progressive partial-thickness tearing. Even in the presence of chronic, massive tears with significant fatty degeneration, repair is often attempted. The subscapularis can function through a tenodesis effect, acting as a static anterior barrier that prevents anterosuperior escape of the humeral head, thereby providing a stable fulcrum for the remaining musculature to elevate the arm.
| Indications for Surgery | Contraindications for Surgery |
|---|---|
| Acute traumatic full-thickness tears | Advanced glenohumeral osteoarthritis (unless concurrent arthroplasty) |
| Symptomatic partial tears failing conservative care | Fixed, uncorrectable superior humeral head escape |
| Subcoracoid impingement with tendon damage | Severe, unmanageable medical comorbidities |
| Concomitant biceps instability requiring intervention | Active joint infection or severe soft tissue compromise |
| Chronic retracted tears (for tenodesis effect) | Inability to comply with strict postoperative rehabilitation |

Pre-Operative Planning, Templating, and Patient Positioning
Anesthesia and Operating Room Setup
Meticulous preoperative planning is the foundation of a successful arthroscopic subscapularis repair. The patient's history, physical examination findings, plain radiographs, and MRI must be comprehensively reviewed by the operative team prior to entering the suite. The surgeon must have a clear mental template of the tear pattern, the degree of retraction, the status of the biceps tendon, and the measured coracohumeral interval to anticipate the need for a coracoplasty.
On the day of surgery, the anesthesiologist administers general anesthesia with endotracheal intubation to ensure airway security during lateral positioning. A regional interscalene nerve block is highly recommended and routinely performed preoperatively to provide preemptive analgesia, significantly reducing intraoperative volatile anesthetic requirements and providing profound postoperative pain relief. Protective eyewear is applied to the patient to prevent inadvertent corneal abrasions during positioning and draping.
The operating room must be configured to allow fluid management systems, arthroscopic towers, and radiofrequency ablation units to be easily accessible without cluttering the sterile field. A dedicated assistant is essential for managing the limb position, passing instruments, and maintaining optimal visualization during the complex mobilization and repair steps required for retracted subscapularis tears.
Lateral Decubitus versus Beach Chair Positioning
While subscapularis repair can be performed in either the beach chair or lateral decubitus position, we strongly prefer the lateral decubitus position for its superior joint distraction, which dramatically improves visualization of the anterior and inferior joint spaces. The patient is carefully rotated into the lateral decubitus position, and an axillary roll is placed to protect the dependent brachial plexus. The patient is meticulously padded with pillows beneath and between the legs to prevent pressure necrosis and neuropraxia.

The patient is secured in place using a vacuum beanbag device
Clinical & Radiographic Imaging Archive