Advanced Management of Calcific Tendinitis & Shoulder Stiffness

Key Takeaway
Calcific tendinitis and refractory shoulder stiffness present significant clinical challenges. This comprehensive guide details the chronological progression of calcific tendinitis, evidence-based indications for surgical intervention, and the precise execution of closed manipulation. Furthermore, it explores the diagnosis and surgical management of quadrilateral space syndrome, providing orthopedic surgeons with a definitive framework for optimizing patient outcomes through both arthroscopic and open techniques.
Comprehensive Introduction and Patho-Epidemiology
The management of refractory shoulder pathologies—specifically shoulder stiffness (adhesive capsulitis), calcific tendinitis of the rotator cuff, and neurovascular entrapment conditions such as quadrilateral space syndrome (QSS)—represents a complex intersection of biomechanics, cellular biology, and advanced surgical technique. These conditions, while distinct in their primary pathoetiologies, frequently present with overlapping clinical phenotypes: profound glenohumeral pain, functional mechanical restriction, and a significant deterioration in the patient's quality of life. As orthopedic surgeons, distinguishing the precise biological phase and mechanical limitations of these entities is paramount to avoiding iatrogenic harm and optimizing functional outcomes.
Refractory shoulder stiffness, classically manifesting as adhesive capsulitis or "frozen shoulder," is characterized by a profound, progressive restriction of both active and passive glenohumeral range of motion. The patho-epidemiology of primary adhesive capsulitis reveals a strong predilection for the female demographic, typically between the fourth and sixth decades of life. Endocrine dysfunctions, most notably diabetes mellitus (both Type I and Type II) and thyroid disorders, are profound risk factors. The underlying pathophysiology is driven by a cytokine-mediated inflammatory cascade—specifically involving transforming growth factor-beta (TGF-β), platelet-derived growth factor (PDGF), and tumor necrosis factor-alpha (TNF-α)—which triggers aggressive fibroblastic proliferation and subsequent capsular fibroplasia. This results in a thickened, contracted, and highly vascularized capsuloligamentous complex that obliterates the normal axillary recess and rotator interval.
Calcific tendinitis is a reactive, self-limiting condition characterized by the deposition of calcium hydroxyapatite crystals within the substance of the rotator cuff tendons. It predominantly affects the supraspinatus tendon (up to 80% of cases), followed by the infraspinatus and subscapularis. Epidemiologically, it mirrors adhesive capsulitis, frequently affecting females aged 30 to 50 years. However, unlike degenerative rotator cuff tears, calcific tendinitis is a process of active cell-mediated reactive calcification. The condition follows a definitive, predictable biological progression originally described by Sarkar and Uhthoff. Spontaneous resolution is observed in almost all cases, with the length of time required for complete resorption being the only true variable. The pathology is strictly divided into three phases: the precalcification stage (fibrocartilaginous metaplasia), the calcification stage (formative, resting, and highly painful resorptive phases), and the postcalcification phase (collagen remodeling).
Quadrilateral space syndrome (QSS) is an uncommon but clinically significant neurovascular entrapment syndrome involving the dynamic compression of the axillary nerve and the posterior humeral circumflex artery. Epidemiologically, QSS is most frequently identified in overhead athletes, throwing populations, and manual laborers who subject their glenohumeral joints to repetitive abduction and external rotation (ABER). The pathoetiology typically involves anomalous, oblique fibrous bands within the quadrilateral space that act as a tethering mechanism, or alternatively, space-occupying lesions such as paralabral cysts extending from posterior labral tears.
The Biological Continuum of Calcific Tendinitis
To master the surgical indications for calcific tendinitis, the surgeon must deeply understand its chronological progression.
1. Phase I: Precalcification Stage: In this initial stage, the site of predilection for calcification—frequently an area within the tendon experiencing a diminished blood supply or localized hypoxia (the "critical zone")—undergoes fibrocartilaginous metaplasia. Tenocytes transform into chondrocytes. Patients are generally asymptomatic, and the condition is undetectable on standard radiographs.
2. Phase II: Calcification Stage: This stage is subdivided into three distinct biological events. First, the Phase of Formation, where calcium is actively deposited into matrix vesicles that coalesce. The deposits are dry, chalky, and granular. Second, the Resting Phase, where active deposition ceases, and the patient may be asymptomatic with well-marginated, dense radiographic deposits. Third, the Resorptive Phase, which is the most clinically significant. Vascular channels rapidly appear at the periphery of the deposit, bringing macrophages and multinucleated giant cells to phagocytize the calcium. The intense inflammatory response and increased intratendinous pressure cause excruciating pain. The calcium resembles thick cream or toothpaste.
3. Phase III: Postcalcification Phase: During this final healing phase, the granulation tissue matures into organized collagen. Fibroblasts align the new collagen along the mechanical stress lines, effectively reconstituting the tendon's structural integrity.
Detailed Surgical Anatomy and Biomechanics
A rigorous understanding of glenohumeral surgical anatomy and the biomechanical consequences of capsular contracture is the absolute foundation of both closed manipulation and arthroscopic intervention. The glenohumeral joint relies on a delicate balance between unconstrained mobility and dynamic/static stability.
The Capsuloligamentous Complex in Shoulder Stiffness
In the setting of adhesive capsulitis, the primary anatomical targets for release are the coracohumeral ligament (CHL), the rotator interval, the middle glenohumeral ligament (MGHL), and the inferior glenohumeral ligament (IGHL) complex.
* The Rotator Interval and CHL: The rotator interval is a triangular anatomic space bordered superiorly by the anterior margin of the supraspinatus, inferiorly by the superior margin of the subscapularis, medially by the coracoid process, and laterally by the transverse humeral ligament. The CHL originates from the base of the coracoid and intimately blends with the superior glenohumeral ligament (SGHL) and the joint capsule. Biomechanically, the CHL is the primary restraint to inferior translation of the adducted shoulder and external rotation in neutral abduction. In shoulder stiffness, contracture of the CHL and rotator interval is the primary culprit for the pathognomonic loss of external rotation with the arm at the side.
* The IGHL Complex: The IGHL consists of an anterior band, a posterior band, and the interposed axillary pouch. It acts as a hammock supporting the humeral head. The anterior band is the primary restraint to anterior translation when the arm is abducted to 90 degrees and externally rotated. In adhesive capsulitis, the axillary pouch becomes obliterated by dense, cross-linked collagen adhesions, severely restricting elevation and abduction.
Microvascular Anatomy of the Rotator Cuff
The predilection for calcific tendinitis in the supraspinatus tendon is intimately linked to its microvascular anatomy. Codman originally described the "critical zone," a region approximately 1.0 to 1.5 cm proximal to the tendon's insertion on the greater tuberosity. Microangiographic studies have demonstrated that this zone is relatively hypovascular, particularly when the arm is adducted, due to the transient compression of the anastomotic vessels between the osseous and tendinous circulations over the humeral head. This localized hypoxia creates a microenvironment conducive to the fibrocartilaginous metaplasia characteristic of the precalcification phase.
Anatomy of the Quadrilateral Space
The quadrilateral space is an anatomic interval in the posterior shoulder through which the axillary nerve and the posterior humeral circumflex artery (PHCA) exit the axilla to innervate and supply the deltoid and teres minor.
* Superior Border: Teres minor (and the inferior margin of the subscapularis anteriorly).
* Inferior Border: Teres major.
* Medial Border: Long head of the triceps brachii.
* Lateral Border: Surgical neck of the humerus.
Biomechanically, when the arm is placed in the ABER position, the teres minor and teres major undergo dynamic approximation. If anomalous fibrous bands are present, this muscular convergence acts as a guillotine, acutely compressing the axillary nerve and PHCA against the surgical neck of the humerus.
Exhaustive Indications and Contraindications
Surgical intervention for these advanced shoulder pathologies must be guided by strict, evidence-based criteria. Premature surgical intervention in self-limiting conditions (like the formative phase of calcific tendinitis) can lead to catastrophic stiffness, whereas delayed intervention in refractory adhesive capsulitis prolongs patient suffering and muscle atrophy.
| Pathology | Primary Surgical Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Refractory Shoulder Stiffness | - Failure of 3-6 months of conservative therapy (PT, intra-articular corticosteroids). - Plateau in ROM improvement. - Severe functional deficit affecting ADLs. |
- Severe osteopenia/osteoporosis (risk of fracture during MUA). - Active joint infection. - Recent proximal humerus fracture. |
- Uncontrolled diabetes mellitus. - Poor patient compliance with post-op PT. - Concomitant severe osteoarthritis. |
| Calcific Tendinitis | - Unrelenting symptom progression despite non-op care. - Constant, severe pain interfering with sleep (resorptive phase). - Chronic mechanical impingement (resting phase). |
- Asymptomatic incidental radiographic finding. - Early formative phase without a trial of conservative care. - Active systemic infection. |
- Massive, irreparable rotator cuff tears in the same shoulder. - Patient inability to tolerate post-op immobilization if tendon repair is required. |
| Quadrilateral Space Syndrome | - Refractory neurovascular symptoms > 6 months. - Positive angiographic/MRA evidence of dynamic PHCA occlusion. - MRI evidence of a compressive paralabral cyst. |
- Cervical radiculopathy mimicking QSS. - Thoracic outlet syndrome. - Parsonage-Turner syndrome (brachial neuritis). |
- Mild, intermittent symptoms controllable with activity modification. - Lack of teres minor fatty infiltration/edema on MRI. |
Nuances in Surgical Decision Making
For calcific tendinitis, we firmly believe that only patients actively in the resorptive phase, or those with chronic, mechanically obstructive resting-phase deposits, should have treatment directed specifically at the calcium deposit itself. For patients in other phases, the clinical focus should follow treatment protocols directed at the primary pathological condition (e.g., subacromial impingement). Gschwend et al. listed strict indications for operative treatment: unrelenting symptom progression, constant severe pain, and complete absence of clinical improvement after a dedicated course of conservative therapy.
For shoulder stiffness, when conservative modalities—including structured physical therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), and intra-articular corticosteroid injections—fail to yield clinical improvement after an adequate trial, closed manipulation under anesthesia (MUA) or arthroscopic capsular release becomes a viable and highly effective intervention.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is essential to mitigate intraoperative complications and ensure comprehensive pathology resolution.
Imaging Modalities and Templating
- Calcific Tendinitis: Standard radiographic evaluation must include true anteroposterior (Grashey), scapular Y, and axillary lateral views. The morphology of the deposit dictates the biological phase: cloudy, ill-defined borders suggest the resorptive phase, whereas dense, well-circumscribed borders indicate the resting phase.
FIGURE 46-13 A: Preoperative AP radiograph demonstrating a large, dense, well-marginated calcium deposit within the supraspinatus tendon, characteristic of the resting phase prior to acute resorption.
- Shoulder Stiffness: While the diagnosis is primarily clinical, MRI or MR arthrography is invaluable for ruling out concomitant pathology (e.g., full-thickness rotator cuff tears) and assessing capsular thickness. Thickening of the CHL (>4 mm) and the joint capsule in the axillary recess are hallmark MRI findings of adhesive capsulitis.
- Quadrilateral Space Syndrome: Diagnosis requires a high index of suspicion. MRI is critical to evaluate for teres minor atrophy or edema (the "J-sign") and to rule out space-occupying paralabral cysts. Conventional or MR angiography with the arm in the ABER position is utilized to demonstrate dynamic occlusion of the posterior humeral circumflex artery.
Patient Positioning and Anesthesia
For advanced arthroscopic management of these conditions, the patient may be positioned in either the beach-chair or lateral decubitus position, depending on surgeon preference and the specific pathology.
* Beach-Chair Position: Preferred for calcific tendinitis excision and concurrent acromioplasty, as it allows for an anatomical orientation of the subacromial space and easy conversion to an open approach if necessary. It is also excellent for MUA, as the scapula is stabilized by the table.
* Lateral Decubitus Position: Offers superior visualization of the axillary pouch and inferior capsule during an arthroscopic 360-degree capsular release for stiffness. It provides longitudinal traction, which opens the subacromial space. This position is also mandatory for the posterior open approach to quadrilateral space decompression.
* Anesthesia: A regional interscalene nerve block combined with general anesthesia is the gold standard. The block provides profound intraoperative muscle relaxation (crucial for MUA) and excellent postoperative analgesia, facilitating immediate aggressive physical therapy.
Step-by-Step Surgical Approach and Fixation Technique
Closed Manipulation and Arthroscopic Capsular Release for Stiffness
The primary objective of closed manipulation is the controlled, sequential rupture of the contracted capsuloligamentous complex. The procedure must be performed with meticulous care to avoid catastrophic iatrogenic complications. The surgeon must utilize short lever arms, stabilizing the scapula firmly against the thoracic wall to isolate glenohumeral motion.
The manipulation typically follows a precise sequence:
1. Elevation in the Scapular Plane: The surgeon stabilizes the scapula and smoothly elevates the arm to rupture the inferior capsule and axillary pouch adhesions.
2. External Rotation at Varying Degrees of Abduction: With the arm adducted to 0 degrees, gentle external rotation releases the CHL and rotator interval. At 90 degrees of abduction, external rotation releases the anterior band of the IGHL.
3. Internal Rotation: Performed at 90 degrees of abduction to release the posterior capsule.
Surgical Warning: Aggressive manipulation utilizing a long lever arm (e.g., grasping the distal forearm or wrist) places the humerus at severe risk for an iatrogenic spiral fracture. Always apply manipulative forces as proximally as possible, ideally at the surgical neck or proximal humerus.
In contemporary practice, MUA is frequently preceded or replaced by an Arthroscopic 360-Degree Capsular Release. Through standard posterior and anterior portals, electrocautery is used to systematically release the rotator interval, the CHL, the MGHL, and the anterior band of the IGHL. The release is carried inferiorly through the axillary pouch, staying strictly on the glenoid side to avoid injury to the axillary nerve, which lies millimeters inferior to the capsule. The posterior capsule is then released from the 6 o'clock to the 9 o'clock position.
Arthroscopic Excision of Calcific Tendinitis
Currently, we prefer an all-arthroscopic technique when surgery is warranted for calcific tendinitis. Following a standard diagnostic glenohumeral arthroscopy, the subacromial space is entered. A thorough bursectomy is performed to clear the visual field.
Localization of the calcific deposit can sometimes be challenging if it is entirely intratendinous. High-resolution intraoperative ultrasound can be utilized to identify deposits that are not readily visible on the bursal surface. Alternatively, a spinal needle is introduced percutaneously to systematically puncture the tendon. The extrusion of "toothpaste-like" or chalky material confirms the exact location of the deposit.
Once localized, a longitudinal incision is made in the direction of the tendon fibers over the deposit. The removal of calcium deposits is performed meticulously with a mechanical shaver, a curette, or a motorized burr on a non-aggressive setting. The goal is the decompression and maximal evacuation of the deposit without excessively violating the structural integrity of the rotator cuff.
If a significant tendinous defect is created during the excision (>1 cm), side-to-side margin convergence or a formal suture anchor repair of the rotator cuff is mandated to prevent tear propagation. Acromioplasty is performed concurrently for patients with definitive preoperative or intraoperative evidence of subacromial stenosis or mechanical impingement.
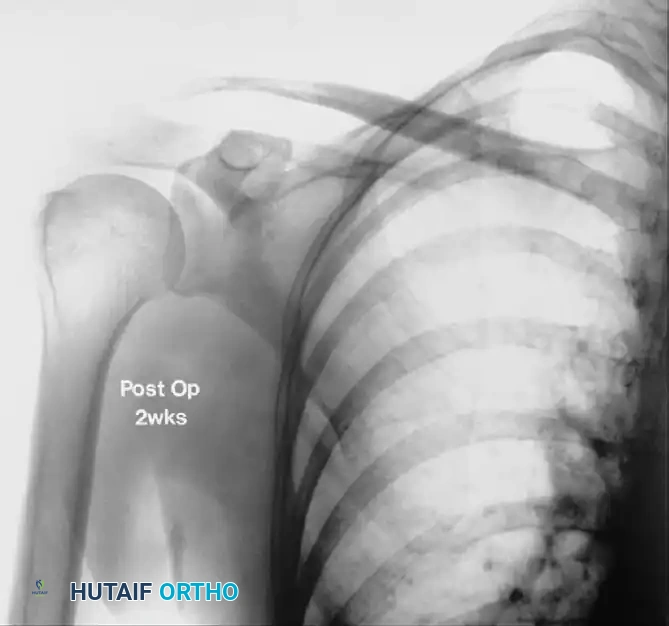
FIGURE 46-13 B: Radiograph taken 2 weeks after arthroscopic excision, demonstrating complete resolution of the calcific deposit and restoration of the subacromial interval.
Surgical Decompression of Quadrilateral Space Syndrome
Surgical decompression is traditionally performed through a posterior open approach. The patient is placed in the lateral decubitus position. An 8-10 cm longitudinal incision is made parallel to the posterior border of the deltoid. The fascia is incised, and the interval between the teres minor and teres major is identified and bluntly developed.
Careful deep dissection reveals the neurovascular bundle (axillary nerve and posterior humeral circumflex artery) exiting the quadrilateral space. The offending anomalous oblique fibrous bands are meticulously lysed with dissecting scissors, completely freeing the neurovascular bundle. If a paralabral cyst is identified as the compressive etiology, it must be decompressed, and the underlying posterior labral pathology should be addressed, often requiring a concurrent or staged arthroscopic labral repair. Lysis of these fibrous bands through a posterior approach consistently yields good to excellent results, with a high rate of return to pre-injury activity levels.
Complications, Incidence Rates, and Salvage Management
Surgical interventions for refractory shoulder pathologies carry inherent risks. Meticulous technique and strict adherence to anatomical boundaries are required to minimize these complications.
| Complication | Associated Procedure | Incidence Rate | Pathomechanism & Salvage Management |
|---|---|---|---|
| Iatrogenic Spiral Fracture | Closed Manipulation (MUA) | 0.5% - 2% | Mechanism: Excessive torque using a long lever arm (distal humerus/forearm) in osteopenic bone. Salvage: Immediate cessation of MUA. Open reduction and internal fixation (ORIF) with a locking plate or intramedullary nail. |
| Axillary Nerve Injury | Arthroscopic Capsular Release / QSS Decompression | 1% - 3% | Mechanism: Thermal injury from electrocautery during inferior capsulotomy (if drifting lateral to the glenoid rim) or direct laceration during QSS decompression. Salvage: Observation and EMG at 6 weeks. If no recovery by 3-6 months, nerve exploration, neurolysis, or nerve grafting. |
| Iatrogenic Rotator Cuff Tear | Calcific Tendinitis Excision | 2% - 5% | Mechanism: Over-aggressive debridement of the supraspinatus tendon during calcium evacuation, leaving a mechanically incompetent tendon. Salvage: Immediate intraoperative recognition and formal rotator cuff repair using suture anchors. |
| Severe Postoperative Flare / Stiffness | Calcific Tendinitis Excision | 5% - 10% | Mechanism: Incomplete removal of calcium crystals leading to a massive inflammatory cascade in the subacromial space. Salvage: Aggressive NSAIDs, oral corticosteroid taper, subacromial steroid injection, and intensive physical therapy. |
| Glenohumeral Dislocation | Closed Manipulation (MUA) | < 1% | Mechanism: Uncontrolled capsular rupture leading to anterior or inferior instability. Salvage: Immediate closed reduction. We occasionally obtain intraoperative AP and axillary radiographs immediately after MUA to definitively rule out periarticular fractures or iatrogenic dislocations. |
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following surgical intervention for these conditions is arguably the most critical determinant of long-term success. The surgeon must communicate specific, phased protocols to the physical therapy team.
Rehabilitation Post-Manipulation and Capsular Release
Without immediate and aggressive rehabilitation, the rapid recurrence of capsular contracture is inevitable. To optimize the rehabilitation timeline, we strategically perform manipulations during the earlier part of the week. This scheduling ensures that the patient can initiate aggressive, supervised physical therapy the very next day without the interruption of a weekend.
* Phase I (Days 1-14): Supervised physical therapy sessions are mandated daily. The primary, non-negotiable goal is the immediate restoration and maintenance of early, full range of motion. Continuous Passive Motion (CPM) machines may be utilized in the recovery room. Pain control is paramount; indwelling interscalene catheters can be left in place for 48-72 hours to facilitate pain-free stretching.
* Orthotic Management: In a subset of patients with severe preoperative stiffness, we recommend the use of an abduction orthosis worn strictly at night for 3 weeks. This positioning places the inferior capsule on stretch, effectively preventing the significant axillary pouch adhesions from returning and cross-linking during the vulnerable early inflammatory phase.
* Phase II (Weeks 3-6): Transition to active-assisted and active range of motion. Initiation of light isometric strengthening of the rotator cuff and periscapular musculature.
Rehabilitation Post-Calcific Tendinitis Excision
The rehabilitation protocol is heavily dependent on the structural integrity of the tendon post-excision.
* Intact Tendon (No Repair): Patients are placed in a simple sling for comfort only. Immediate active and passive ROM is encouraged to prevent secondary adhesive capsulitis. Strengthening begins at 2-3 weeks as pain allows.
* Repaired Tendon: If a formal rotator cuff repair was required to close the defect, the patient follows a standard rotator cuff protocol: 4-6 weeks of strict immobilization in an abduction sling, followed by progressive passive, active-assisted, and eventually active ROM. Strengthening is delayed until 8-12 weeks to allow for biological tendon-to-bone or side-to-side healing.
Rehabilitation Post-Quadrilateral Space Decompression
- Phase I (Weeks 0-4): The arm is supported in a sling. Passive and active-assisted ROM is permitted, but the ABER position (abduction and external rotation) is strictly avoided to prevent tension on the healing tissues and the decompressed neurovascular bundle.
- Phase II (Weeks 4-8): Progressive restoration of full ROM. Initiation of periscapular stabilization exercises and deltoid/teres minor strengthening.
- Phase III (Months 2-4): Gradual return to sports-specific activities, including throwing programs for overhead athletes, provided that neurovascular symptoms have completely resolved.
Summary of Landmark Literature and Clinical Guidelines
The evolution of treatment for these refractory shoulder conditions is deeply rooted in landmark orthopedic literature.
For Calcific Tendinitis, the biological framework established by Sarkar and Uhthoff remains the undisputed gold standard for understanding the pathology. Their histological analyses proved that the condition is an active cell-mediated process rather than a degenerative one. Regarding nonoperative management, alternative modalities have gained traction. An ultrasound-guided percutaneous needling technique (barbotage), used in conjunction with a subacromial corticosteroid injection, has been reported to be successful in approximately 70% of patients. Furthermore, Extracorporeal Shock Wave Therapy (ESWT) has been advocated. Several comparative studies have reported greater pain relief with ESWT than with placebo; however, it is notable that in one major study, half of the patients treated with ESWT eventually required surgical intervention. Long-term follow-up studies unequivocally confirm the benign natural history of this disorder. Although surgically treated patients have superior short-term results, at 5+ years, there are no statistically significant differences in functional outcomes between operative and nonoperative cohorts.
Clinical Pearl: While corticosteroids provide profound short-term pain relief, they have been suggested to prematurely abort the resorptive phase. By suppressing the macrophage-mediated inflammatory response, corticosteroids may return the lesion to a state of dormancy, effectively setting into motion the biological factors necessary for future recurrence.
For Shoulder Stiffness, the classic studies by Neviaser delineated the pathology of adhesive capsulitis, highlighting the obliteration of the axillary fold. Modern comparative literature evaluating MUA versus arthroscopic capsular release suggests that while both are highly effective, arthroscopic release provides a more controlled, precise sectioning of the contracted tissues with a significantly lower risk of iatrogenic fracture, making it the preferred modality in patients with osteopenia or prolonged, severe contractures.
For Quadrilateral Space Syndrome, the original descriptions by Cahill and Palmer established the foundation for diagnosis, emphasizing the dynamic nature of the compression and the necessity of ABER positioning during angiography. Modern literature heavily supports the posterior open approach for lysis of fibrous bands, demonstrating predictable relief of the neurovascular tethering and restoration of function in high-demand athletes.
