Masterclass in Hammer Toe Correction: PIP Arthroplasty & Arthrodesis Techniques

Key Takeaway
This masterclass offers an exhaustive, intraoperative guide to hammer toe correction. We delve into detailed anatomy, patient positioning, and step-by-step surgical execution for both PIP joint resection arthroplasty and arthrodesis, including K-wire and implant techniques. Fellows will gain insights into neurovascular risks, meticulous dissection, hardware application, and crucial pearls for avoiding pitfalls and managing complications, ensuring optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater and to this definitive exploration of one of the most ubiquitous, yet biomechanically complex, pathologies encountered in forefoot surgery: the hammer toe deformity. This condition extends far beyond a simple cosmetic grievance; it is a profound disruption of the sagittal plane mechanics of the lesser rays that can lead to debilitating pain, profound functional limitation, and severe soft tissue compromise. As orthopedic surgeons, our objective is not merely the excision of bone to achieve an aesthetically straight digit, but rather the meticulous restoration of the intricate dynamic balance between the intrinsic and extrinsic musculature of the foot.
The hammer toe deformity is defined by a primary sagittal plane flexion contracture localized specifically at the proximal interphalangeal (PIP) joint of a lesser digit. It is imperative to distinguish this specific pathomorphology from other adjacent lesser toe deformities to ensure the correct surgical algorithm is applied. A mallet toe, by contrast, presents with an isolated flexion contracture at the distal interphalangeal (DIP) joint, leaving the PIP joint relatively unaffected. A claw toe represents a more globally devastating biomechanical failure, characterized by a primary, rigid dorsiflexion contracture at the metatarsophalangeal (MTP) joint, invariably accompanied by secondary flexion contractures at both the PIP and DIP joints.

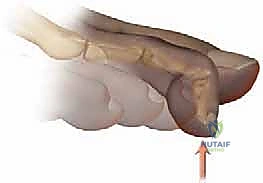
While a hammer toe may occasionally present with a mild, secondary extension deformity at the MTP joint, the clinical hallmark and primary driver of the patient's symptomatology remains the PIP flexion contracture. The natural history of this deformity is one of progressive rigidity. Initially presenting as a flexible deformity that can be passively reduced to neutral alignment, chronic biomechanical forces eventually lead to structural adaptations. The joint capsule, collateral ligaments, and plantar plate undergo fibrotic contracture, transitioning the digit into a fixed, rigid state.
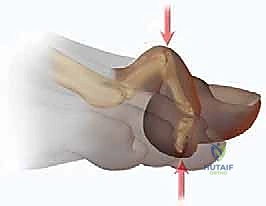
Epidemiologically, hammer toe deformities exhibit a strong predilection for the female population, a disparity heavily correlated with the utilization of restrictive, narrow toe-box footwear and high-heeled shoes. The pathogenesis is multifactorial, encompassing intrinsic anatomic predispositions (such as a long second metatarsal or inherent ligamentous laxity) and extrinsic mechanical forces. When the digits are chronically crowded and forced into passive flexion within a non-accommodative shoe box, the extensor digitorum longus (EDL) loses its mechanical advantage. This persistent mechanical disadvantage, particularly when coupled with MTP dorsiflexion, initiates a vicious cycle of intrinsic-extrinsic muscle imbalance that ultimately culminates in fixed structural deformity and the formation of painful, hyperkeratotic lesions over the dorsal PIP joint and the distal tuft of the phalanx.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical incision, an exhaustive comprehension of the micro-anatomy and biomechanics of the lesser rays is absolutely paramount. The lesser digits are unforgiving anatomic territories; they are densely packed with critical neurovascular and tendinous structures where even minor iatrogenic trauma can precipitate catastrophic outcomes, including ischemic necrosis or debilitating chronic pain.
Osteology and Articular Mechanics
The lesser toes (digits two through four) are composed of three distinct articulating segments: the distal, middle, and proximal phalanges. The fifth digit frequently presents as an anatomical variant, possessing only two phalanges (proximal and distal) in up to 15% to 20% of the patient population. The foundation of the lesser ray is the metatarsophalangeal (MTP) joint, a complex condyloid articulation permitting flexion, extension, abduction, and adduction. The stability of the MTP joint relies heavily on the integrity of the plantar plate, a robust fibrocartilaginous structure, along with the true and accessory collateral ligaments.
The proximal interphalangeal (PIP) joint, the primary site of pathology in a hammer toe, functions as a true hinge joint. Its motion is strictly limited to the sagittal plane (flexion and extension). The articular geometry features a bicondylar proximal phalanx head articulating with the biconcave base of the middle phalanx. Stability is conferred by the collateral ligaments, the joint capsule, and the delicate plantar plate of the PIP joint. The distal interphalangeal (DIP) joint mirrors the PIP joint in both structure and function, acting as a terminal hinge.
Musculotendinous Architecture
The dynamic stability of the lesser toes is governed by a precise, fragile equilibrium between the extrinsic musculature (originating in the leg) and the intrinsic musculature (originating within the foot). The primary extrinsic extensor, the Extensor Digitorum Longus (EDL), courses dorsally and trifurcates over the proximal phalanx. The central slip inserts onto the base of the middle phalanx, while the lateral slips converge to insert onto the distal phalanx. The EDL is primarily an MTP joint dorsiflexor; its ability to extend the PIP and DIP joints is highly dependent on the MTP joint being in a neutral or flexed position.

Conversely, the Flexor Digitorum Longus (FDL) serves as the primary extrinsic flexor, traversing the plantar aspect of the digit to insert onto the base of the distal phalanx. The intrinsic muscles—comprising the lumbricals, interossei, Flexor Digitorum Brevis (FDB), and Extensor Digitorum Brevis (EDB)—are the true modulators of fine digit control. The lumbricals, originating from the FDL tendons, pass plantar to the deep transverse metatarsal ligament to insert into the medial aspect of the extensor hood. They are unique in their function: flexing the MTP joint while simultaneously extending the PIP and DIP joints. In a hammer toe deformity, the chronic MTP dorsiflexion effectively neutralizes the lumbricals' mechanical advantage, exacerbating the PIP flexion contracture driven by the unopposed pull of the FDB.
Neurovascular Safe Zones and Vulnerabilities
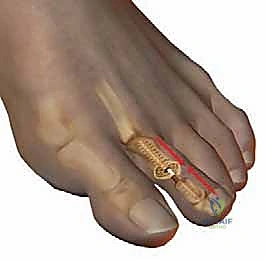
A meticulous approach to the neurovascular anatomy is the hallmark of a master foot and ankle surgeon. Each lesser digit is supplied by four primary neurovascular bundles: two dorsal and two plantar. The dorsal digital nerves and arteries course superficially within the subcutaneous tissue, located dorsomedially and dorsolaterally. These structures are exquisitely vulnerable during the initial skin incision and subsequent superficial dissection.

The plantar digital nerves and arteries are larger, providing the dominant arterial inflow to the digit. They run deep along the plantar-medial and plantar-lateral borders of the flexor tendon sheath. Surgical dissection must remain strictly within the designated safe zones—typically directly over the dorsal midline of the extensor tendon for PIP approaches—utilizing blunt dissection techniques to gently sweep the neurovascular bundles laterally and medially. Failure to respect these boundaries can result in digital ischemia ("white toe" on the table) or the formation of painful, intractable postoperative neuromas.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for a hammer toe deformity must be predicated on a rigorous clinical evaluation, failed conservative management, and a clear understanding of the patient's physiological status. Surgery is never indicated for purely cosmetic reasons; the primary goals are the alleviation of pain, the eradication of recurrent ulcerations, and the restoration of a plantigrade, functional forefoot.
Clinical Evaluation and Surgical Decision Making
The preoperative physical examination must systematically isolate the pain generator and assess the flexibility of the deformity. The "push-up test" (loading the metatarsal heads to simulate weight-bearing) is critical for evaluating the MTP joint's contribution to the deformity. If the PIP deformity is fully correctable passively, it is deemed flexible, and soft-tissue procedures (e.g., flexor-to-extensor transfer) may suffice. However, the vast majority of symptomatic patients present with a fixed, rigid deformity necessitating osseous resection (arthroplasty or arthrodesis).
Furthermore, the vascular status of the limb must be unequivocally established. Palpation of the dorsalis pedis and posterior tibial pulses is mandatory. In patients with a history of diabetes, smoking, or absent palpable pulses, non-invasive vascular studies (Ankle-Brachial Index, Toe-Brachial Index, and transcutaneous oximetry) are strictly required. Proceeding with elective forefoot surgery in the presence of compromised macro- or microvascular perfusion is a direct route to ischemic necrosis and subsequent amputation.
Indications and Contraindications Matrix
| Category | Specific Criteria | Rationale |
|---|---|---|
| Absolute Indications | Severe, recalcitrant pain at the PIP joint or distal tuft failing >3 months of conservative care. | Mechanical deformity requires structural correction once soft tissues have permanently contracted. |
| Absolute Indications | Recurrent or impending ulceration over the dorsal PIP joint or plantar metatarsal head. | Prophylaxis against deep space infection and osteomyelitis, particularly in the diabetic population. |
| Relative Indications | Difficulty with shoe wear accommodation leading to secondary functional limitations. | Improving quality of life and mobility in active patients. |
| Absolute Contraindications | Peripheral Arterial Disease (ABI < 0.5, TBI < 0.3, or flat waveform). | High probability of postoperative digital ischemia, wound dehiscence, and gangrene. |
| Absolute Contraindications | Active, untreated local or systemic infection. | Risk of seeding the surgical site and hardware (if utilizing K-wires or implants). |
| Relative Contraindications | Severe peripheral neuropathy (Charcot neuroarthropathy). | High risk of non-compliance, hardware failure, and unrecognized postoperative complications. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the invisible foundation upon which a successful surgical outcome is built. This phase demands a synthesis of radiographic analysis, appropriate patient positioning, and the selection of the optimal anesthetic modality to ensure both surgical exposure and patient safety.
Radiographic Templating and Analysis
Standard weight-bearing radiographs of the foot (anteroposterior, lateral, and oblique views) are non-negotiable. The AP view allows for the assessment of the overall metatarsal parabola, the presence of concurrent hallux valgus (which must often be addressed simultaneously to prevent recurrence of the lesser toe deformity), and the length of the involved proximal phalanx.

The surgeon must evaluate the MTP joint for signs of subluxation, dislocation, or degenerative arthrosis. If the MTP joint is subluxated, a simple PIP arthroplasty will fail; a concurrent Weil osteotomy or extensive MTP soft-tissue release must be templated. The lateral radiograph confirms the apex of the deformity at the PIP joint and helps estimate the amount of proximal phalangeal condylar resection required to decompress the joint and achieve tension-free linear alignment.
Positioning, Anesthesia, and Tourniquet Application
The patient is positioned supine on the operating table. A small bump may be placed under the ipsilateral hip to internally rotate the lower extremity to a neutral position, ensuring the dorsal aspect of the foot faces directly upwards. Proper lighting and magnification (loupes) are highly recommended given the delicate neurovascular structures involved.

Anesthesia typically consists of monitored anesthesia care (MAC) supplemented by a highly effective regional block. A Mayo block or a targeted ankle block utilizing a long-acting local anesthetic (e.g., 0.5% bupivacaine) provides excellent intraoperative anesthesia and prolonged postoperative analgesia. Hemostasis is critical for visualization. A pneumatic calf or ankle tourniquet is routinely utilized, inflated to roughly 100 mmHg above the patient's systolic blood pressure, following exsanguination of the foot via elevation or an Esmarch bandage.
Step-by-Step Surgical Approach and Fixation Technique
The surgical correction of a fixed hammer toe deformity requires a methodical, stepwise approach. The choice between a PIP arthroplasty (resection of the proximal phalanx head with soft tissue interposition) and a PIP arthrodesis (fusion of the joint) depends on the severity of the deformity, the specific digit involved, and the patient's functional demands. Generally, arthrodesis provides superior long-term stability and is preferred for the second and third digits, while arthroplasty is often sufficient for the fourth and fifth digits.
Incision, Exposure, and Joint Preparation
The procedure begins with a dorsal longitudinal incision centered over the PIP joint, extending from the distal third of the proximal phalanx to the proximal third of the middle phalanx. Alternatively, a transverse elliptical incision can be utilized to excise the redundant, hyperkeratotic skin overlying the joint, though this requires meticulous closure to avoid tension.


Dissection is carried sharply through the dermis. Subcutaneous tissues are bluntly swept medially and laterally to identify and protect the dorsal neurovascular bundles. The extensor tendon apparatus is then identified. A longitudinal tenotomy is performed directly through the central slip of the extensor tendon, exposing the underlying PIP joint capsule.

A transverse capsulotomy is executed, and the collateral ligaments are sharply released from their attachments on the proximal phalanx head. This allows for acute plantarflexion of the middle phalanx, effectively "shotgunning" the PIP joint and providing circumferential exposure of the proximal phalangeal condyles.

Osseous Resection: Arthroplasty vs. Arthrodesis
If performing a standard PIP arthroplasty, a microsaw or a double-action bone rongeur is used to resect the head of the proximal phalanx just proximal to the surgical neck. The resection must be perpendicular to the long axis of the shaft. The plantar aspect of the remaining shaft is then smoothed with a rasp to prevent plantar pressure points.


If an arthrodesis is planned, the articular cartilage of the base of the middle phalanx must also be meticulously denuded using a rongeur or a small curette, exposing bleeding subchondral bone. For a more stable construct, a "peg-in-hole" technique can be employed, where the proximal phalanx is shaped into a conical peg, and a corresponding receptacle is drilled into the base of the middle phalanx.

Fixation Strategies and MTP Joint Management
Following osseous resection, the toe is provisionally reduced. If residual deformity persists at the MTP joint, a sequential release is mandatory. This begins with an extensor tendon Z-lengthening, followed by a dorsal MTP capsulotomy, and, if necessary, release of the MTP collateral ligaments.
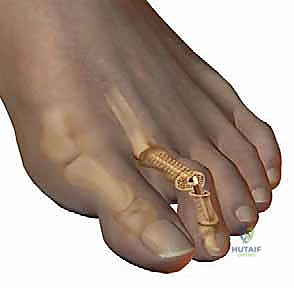
For fixation of the PIP arthrodesis (or temporary stabilization of an arthroplasty), a smooth Kirschner wire (typically 0.045 or 0.062 inches) is the gold standard. The K-wire is driven axially in an antegrade fashion through the central axis of the middle and distal phalanges until it exits the tip of the toe.


The drill is then moved to the distal end of the wire. The PIP joint is reduced, ensuring perfect rotational alignment, and the K-wire is driven retrograde into the medullary canal of the proximal phalanx. If MTP stability is a concern, the wire can be advanced across the MTP joint into the metatarsal shaft.


Once fixation is secure, the tourniquet is deflated to confirm digital perfusion. The extensor tendon is repaired using a fine absorbable suture (e.g., 4-0 Vicryl). The skin is closed with non-absorbable monofilament sutures (e.g., 4-0 or 5-0 Nylon) in a simple interrupted or horizontal mattress fashion.



The K-wire is bent at the tip of the toe and cut to prevent proximal migration, and a sterile, compressive forefoot dressing is meticulously applied.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following hammer toe correction are not uncommon. The orthopedic surgeon must be intimately familiar with the identification and immediate management of these adverse events. The most feared intraoperative complication is vascular compromise, presenting as a blanched, avascular digit ("white toe") upon tourniquet deflation.
If a white toe is encountered, the surgeon must act swiftly. The digit should be placed in a dependent position, and warm saline should be applied to induce vasodilation. If the digit is pinned in severe extension, the K-wire may be placing undue traction on the neurovascular bundles; the pin must be immediately withdrawn or repositioned. Pharmacologic adjuncts, such as topical nitroglycerin paste or a local injection of phentolamine, can be utilized to break arterial vasospasm. If perfusion is not restored, an immediate vascular surgery consultation is mandated.
Other complications include infection (superficial pin tract or deep osteomyelitis), hardware failure, nonunion of the arthrodesis site, and recurrence of the deformity. A "floating toe" complication can occur if the MTP joint is over-released or if the plantar plate is compromised, leading to a toe that fails to purchase the ground during the stance phase of gait.
Complications and Salvage Protocol Matrix
| Complication | Estimated Incidence | Prevention & Salvage Management |
|---|---|---|
| Vascular Compromise ("White Toe") | 1% - 3% | Prevention: Avoid excessive traction; respect NV bundles. Salvage: Remove K-wire, warm saline, dependent position, topical nitroglycerin, phentolamine injection. |
| Pin Tract Infection | 5% - 10% | Prevention: Meticulous pin care protocols; avoid tension at skin interface. Salvage: Oral antibiotics (first-generation cephalosporin); early pin removal if deep infection suspected. |
| Recurrence of Deformity | 10% - 20% | Prevention: Ensure adequate bone resection; address concurrent MTP pathology. Salvage: Revision arthrodesis; flexor tendon transfer; Weil osteotomy. |
| Nonunion (Arthrodesis) | 5% - 15% | Prevention: Meticulous joint preparation down to bleeding subchondral bone; rigid fixation. Salvage: Often asymptomatic; if painful, revision arthrodesis with bone grafting. |
| Floating Toe Syndrome | 2% - 5% | Prevention: Avoid over-lengthening the extensor apparatus; preserve plantar plate integrity. Salvage: Flexor-to-extensor transfer; MTP plantar capsulorrhaphy. |
Phased Post-Operative Rehabilitation Protocols
The success of a hammer toe reconstruction is as dependent on the postoperative rehabilitation protocol as it is on the surgical execution. A structured, phased approach ensures the protection of the surgical repair while mitigating the risks of profound stiffness and disuse atrophy.
Phase I: Maximum Protection (Weeks 0-4)
Immediately postoperatively, the patient is placed in a rigid, flat-bottomed postoperative shoe or a controlled ankle motion (CAM) boot. Weight-bearing is generally restricted to heel-touch or strict flat-foot weight-bearing to minimize sheer forces across the forefoot. The foot must be elevated strictly above the level of the heart for the first 48 to 72 hours to control edema, which is the primary driver of postoperative pain and wound healing complications.
If a percutaneous K-wire is utilized, pin care is initiated after the first postoperative dressing change (typically at 1 week). Patients are instructed to clean the pin site daily with a dilute betadine or chlorhexidine solution and apply a sterile dressing. The K-wire remains in place for 4 to 6 weeks, depending on the stability of the arthrodesis or arthroplasty site.
Phase II: Transition and Mobilization (Weeks 4-8)
At the 4-to-6-week mark, clinical and radiographic evaluations are performed. If an arthrodesis was performed, radiographs should demonstrate early consolidating callus. The percutaneous K-wire is removed in the clinic setting (a procedure typically well-tolerated without local anesthesia).
Once the hardware is removed, the patient is transitioned into a wide toe-box, stiff-soled athletic shoe. Active and passive range-of-motion exercises are initiated, focusing primarily on the MTP joint to prevent extension contractures. The patient is instructed to perform manual plantarflexion stretching of the MTP joint multiple times daily. Taping the toe in slight plantarflexion (buddy taping to the adjacent normal digit) can assist in maintaining alignment and reducing edema.
Phase III: Return to Function (Weeks 8+)
By the 8-week mark, most patients can begin a gradual return to their baseline activities and preferred footwear, though high-heeled shoes and narrow toe boxes should be permanently discouraged to prevent recurrence. Edema
