Glenohumeral Arthrodesis: A Masterclass in Salvage Shoulder Reconstruction

Key Takeaway
Glenohumeral arthrodesis is a demanding salvage procedure for severe shoulder dysfunction. This masterclass details patient selection, meticulous surgical anatomy, beach chair positioning, an S-shaped incision, precise glenoid and humeral head decortication, and fixation with a contoured 4.5mm pelvic reconstruction plate. We emphasize achieving 30° abduction, 30° forward flexion, and 30° internal rotation for optimal hand function.
Comprehensive Introduction and Patho-Epidemiology
Glenohumeral arthrodesis remains one of the most technically demanding and biologically challenging salvage procedures in the armamentarium of the reconstructive shoulder surgeon. In an era dominated by the exponential rise and success of reverse total shoulder arthroplasty (RTSA) and advanced tendon transfer techniques, the indications for primary shoulder fusion have precipitously narrowed. However, despite these incredible advancements, glenohumeral arthrodesis endures as a critical, often limb-saving intervention for a carefully selected, highly complex patient demographic. It is a procedure that demands an uncompromising understanding of shoulder girdle biomechanics, meticulous preoperative planning, and precise intraoperative execution to achieve a stable, pain-free platform for the upper extremity.
The pathophysiology driving the necessity for a glenohumeral fusion is typically characterized by catastrophic failure of the dynamic stabilizers of the shoulder, severe bone loss, or insurmountable joint destruction. Patients presenting with flail shoulders secondary to devastating upper trunk brachial plexus injuries, advanced anterior poliomyelitis, or isolated complete axillary nerve paralysis often suffer from intractable pain due to inferior subluxation and capsular stretching. In these scenarios, the glenohumeral joint ceases to function as a dynamic articulation and instead becomes a source of profound morbidity, rendering the distal extremity functionally useless despite potentially intact elbow and hand mechanics.
The ultimate, overarching goal of glenohumeral arthrodesis is to convert a painful, unstable, or flail articulation into a fixed, functional strut. By rigidly coupling the humerus to the scapula, we effectively transfer the fulcrum of upper extremity motion entirely to the scapulothoracic articulation. This functional redirection relies entirely on the integrity of the periscapular musculature—specifically the trapezius, levator scapulae, and serratus anterior. When successfully executed, this fixed platform allows the patient to leverage scapulothoracic motion to position the hand in space, enabling essential activities of daily living (ADLs), most notably the ability to bring the hand to the midline anteriorly to reach the mouth, face, and contralateral shoulder.
Epidemiologically, the incidence of glenohumeral arthrodesis is exceedingly low, typically reserved for tertiary or quaternary referral centers specializing in complex nerve injuries, orthopedic oncology, and revision arthroplasty. The patient population is bimodal, encompassing young adult males who have sustained high-energy trauma resulting in brachial plexus avulsions, and older adults facing massive, irreparable rotator cuff tears complicated by profound infection or severe bone loss precluding revision arthroplasty. Mastery of this procedure is therefore an essential competency for the advanced reconstructive surgeon, as it represents the definitive endpoint in the reconstructive algorithm when all other joint-preserving or arthroplasty options have been exhausted.
Detailed Surgical Anatomy and Biomechanics
Osteology and Fusion Surfaces
Before a scalpel touches skin, the surgeon must possess a three-dimensional, internalized map of the shoulder girdle's osteology, recognizing the severe limitations inherent in the scapular anatomy. The scapula is a notoriously thin, membranous bone; the only regions providing sufficient cortical density and volume for robust hardware fixation are the glenoid fossa, the base of the coracoid process, the lateral border, and the spine of the scapula. We must meticulously respect these limitations during hardware placement to prevent catastrophic pullout. The proximal humerus, conversely, generally offers excellent cancellous bone stock for the placement of large-diameter lag screws, provided there is no pre-existing cystic degeneration or tumor-related osteolysis.
To maximize the probability of achieving a solid, mature arthrodesis, the surgeon must look beyond the traditional glenohumeral articulation. The surface area of the native glenoid is simply insufficient to guarantee reliable bony bridging, particularly in the presence of massive shear forces. Therefore, the contemporary technique mandates an extra-articular extension of the fusion mass. We must meticulously decorticate not only the glenoid face and the corresponding articular surface of the humeral head but also the undersurface of the acromion and the superior aspect of the greater tuberosity.
By incorporating the acromiohumeral articulation into the fusion construct, we exponentially increase the biological surface area available for osteogenesis. This "double fusion" technique provides a superior biomechanical construct, neutralizing superior migration forces and providing a broad, vascularized bed for bone graft incorporation. The scapular spine serves as the critical posterior anchor point for our reconstruction plate, providing a broad, strong cortical surface that can withstand the significant cantilever forces exerted by the weight of the upper extremity.
Muscular Intervals and Soft Tissue Considerations
The surgical approach for glenohumeral arthrodesis relies heavily on the mastery of the deltopectoral interval and the nuanced management of the surrounding musculature. Identifying and developing the plane between the deltoid muscle laterally and the pectoralis major medially is the foundational step of the anterior exposure. The management of the deltoid muscle itself is entirely dependent on its preoperative neurologic status. If the deltoid is innervated and functional, it must be meticulously elevated subperiosteally from the anterior and lateral acromion to preserve its origin and neurovascular pedicle.
Conversely, if the deltoid is denervated—a frequent clinical reality in severe brachial plexus injuries or isolated axillary nerve palsies—the surgical strategy shifts. In these instances, the surgeon may elect to split the deltoid directly between its anterior and lateral heads. This aggressive approach provides a vastly superior, unencumbered exposure of the proximal humerus and glenohumeral joint without the concern of sacrificing functional muscle tissue. Regardless of the approach, the rotator cuff musculature (subscapularis, supraspinatus, infraspinatus, and teres minor) is systematically resected to fully expose the articular surfaces. Because the goal is absolute rigidity, the dynamic function of the cuff is obsolete, and its tendinous insertions act only as barriers to bony apposition.
The long head of the biceps tendon, if present and intact, must be addressed. Given the extensive alteration of the proximal humeral anatomy and the resection of the rotator cuff, the biceps tendon becomes a significant source of postoperative pain and potential mechanical irritation. It is routinely identified distally in the bicipital groove, sharply tenotomized from its superior labral origin, and tenodesed to the upper border of the pectoralis major tendon or the conjoint tendon. Finally, the absolute prerequisite for this procedure is the functional integrity of the periscapular muscles. The trapezius, levator scapulae, and serratus anterior are the sole drivers of the newly established scapulothoracic mechanism; their paralysis represents an absolute contraindication to the procedure.
Neurovascular Topography and Surgical Risks
The neurovascular topography of the shoulder girdle presents several critical hazard zones during a glenohumeral arthrodesis. The axillary nerve is arguably the most vulnerable structure during this procedure. Exiting the quadrangular space, it wraps intimately around the surgical neck of the humerus, providing motor innervation to the deltoid and teres minor. During subperiosteal elevation of the deltoid, placement of retractors on the inferior humeral neck, or the drilling and insertion of the most distal plate screws, the surgeon must maintain acute spatial awareness of the axillary nerve's trajectory to prevent devastating iatrogenic injury.
The brachial plexus and the axillary artery and vein lie anterior and inferior to the glenohumeral joint, generally protected by the bulk of the pectoralis major and the coracobrachialis. However, during the release of the inferior capsule, resection of the subscapularis, or the placement of inferiorly directed lag screws from the humerus into the glenoid neck, aggressive retraction or errant drill trajectories can easily compromise these vital structures. Meticulous dissection, the use of blunt retractors (such as Darrach or blunt Hohmann retractors), and direct visualization are mandatory when working in the inferior and medial quadrants of the joint.
Superficially, the cephalic vein serves as the primary landmark for the deltopectoral interval. While every effort should be made to preserve the vein by retracting it laterally with the deltoid (to preserve venous drainage of the flap) or medially with the pectoralis, it may be ligated if it severely impedes exposure or is inadvertently injured. Furthermore, the anterior and posterior circumflex humeral arteries, which form an anastomotic ring around the surgical neck of the humerus, are frequently encountered during the inferior capsular release and must be preemptively identified and electrocoagulated to maintain a pristine, bloodless surgical field.
Exhaustive Indications and Contraindications
The decision to proceed with a glenohumeral arthrodesis requires a rigorous, multidisciplinary evaluation of the patient's pathology, functional deficits, and psychological readiness. This is an irreversible salvage procedure; therefore, the indications must be absolute, and all alternative reconstructive options must have been systematically ruled out.
The classic indication is the flail, painful shoulder secondary to devastating neurologic injury. Patients with upper trunk brachial plexus palsies (C5-C6 avulsions) who have failed nerve grafting or tendon transfers, or those with late-stage anterior poliomyelitis, often present with profound instability and pain due to capsular traction. In orthopedic oncology, en bloc resection of periarticular malignant tumors (e.g., proximal humeral osteosarcoma or chondrosarcoma) that necessitates the sacrifice of the deltoid, rotator cuff, and axillary nerve leaves the patient with a functionally useless arm. In these scenarios, an intercalary allograft or vascularized fibular graft combined with a glenohumeral arthrodesis provides a durable, stable limb.
Infectious and degenerative pathologies also represent significant indications. Severe, destructive septic arthritis of the glenohumeral joint in a young, active laborer where total shoulder arthroplasty is contraindicated due to the risk of recurrent infection is a prime candidate for fusion. Furthermore, glenohumeral arthrodesis serves as the ultimate salvage for failed total shoulder arthroplasty or reverse total shoulder arthroplasty. When faced with catastrophic glenoid bone loss, massive periprosthetic osteolysis, or chronic periprosthetic joint infection (PJI) where reimplantation is impossible, a resection arthroplasty followed by a delayed fusion utilizing massive structural bone grafting may be the only viable alternative to amputation.
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Primary Indications | Flail shoulder (Brachial plexus injury, Polio, Axillary nerve palsy) | Eliminates pain from inferior subluxation; provides stable strut for hand function. |
| Post-tumor resection | Reconstruction after sacrifice of deltoid/rotator cuff; combined with massive allograft. | |
| Intractable Septic Arthritis | Eradicates joint space; avoids hardware in high-risk infectious environments (vs arthroplasty). | |
| Failed Arthroplasty Salvage | End-stage option for catastrophic bone loss or chronic periprosthetic joint infection (PJI). | |
| Absolute Contraindications | Paralysis of Periscapular Musculature | Trapezius, levator scapulae, or serratus anterior failure prevents any postoperative arm elevation. |
| Progressive Neurologic Disorders | Conditions like ALS or muscular dystrophy where future periscapular paralysis is inevitable. | |
| Contralateral Shoulder Arthrodesis | Bilateral fusions severely restrict ADLs, specifically personal hygiene and perineal care. | |
| Relative Contraindications | Poor Patient Compliance / Psychological Unreadiness | Requires extensive, grueling postoperative rehabilitation and acceptance of permanent ROM loss. |
| Advanced Age with Low Functional Demand | Resection arthroplasty (pseudarthrosis) may be better tolerated with fewer surgical risks. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and Diagnostic Modalities
Success in glenohumeral arthrodesis is predicated upon exhaustive preoperative planning. Standard orthogonal radiographs, including true anteroposterior (Grashey), scapular Y, and axillary lateral views, are mandatory to assess gross deformity, subluxation, and baseline bone stock. However, plain radiography is insufficient for the granular planning required for complex fusions. A high-resolution Computed Tomography (CT) scan with 3D reconstructions is indispensable. The CT scan allows the surgeon to meticulously quantify glenoid bone loss, evaluate the cortical thickness of the scapular spine, and anticipate the exact volume and morphology of structural bone graft required, particularly in revision arthroplasty scenarios.
In cases where the etiology of the shoulder dysfunction is neurologic, or if there is any ambiguity regarding the functional status of the shoulder girdle musculature, a comprehensive Electromyogram (EMG) and Nerve Conduction Study (NCS) must be obtained. The EMG is critical for confirming the absolute paralysis of the deltoid and rotator cuff (justifying the fusion) while simultaneously verifying the robust, intact innervation of the trapezius and serratus anterior (the prerequisite for functional success). Proceeding with an arthrodesis without confirming periscapular muscle viability is a recipe for a catastrophic functional failure.
Hardware Templating and Graft Preparation
Preoperative templating is essential for anticipating hardware needs and minimizing intraoperative delays. The workhorse implant for a primary glenohumeral arthrodesis is a heavy-duty, 10-hole to 14-hole, 4.5-mm pelvic reconstruction plate. This specific plate offers the ideal balance of robust biomechanical strength and malleability, allowing it to be contoured to the complex, multi-planar anatomy of the scapular spine, acromion, and proximal humerus.
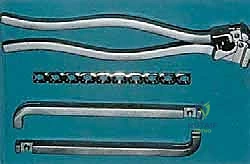
The surgical team must ensure the availability of specialized contouring equipment, including handheld bending irons, a heavy-duty plate press, and bending templates. The surgeon should use the 3D CT reconstructions to mentally template the plate's trajectory, anticipating the required twists and bends to transition from the transverse plane of the scapular spine to the coronal/sagittal plane of the humeral shaft. Furthermore, the surgeon must plan for bone grafting. While local autograft from the resected humeral head is often sufficient for primary cases, revision cases or tumor reconstructions will require preoperative planning for the harvest of massive iliac crest autograft, vascularized fibular grafts, or the procurement of structural allografts.
Patient Positioning and OR Ergonomics
The patient is positioned in the beach chair configuration, which provides unparalleled access to the anterior, superior, and posterior aspects of the shoulder girdle simultaneously. The back of the operative table is elevated to approximately 30 to 45 degrees. This specific angle is critical; it utilizes gravity to gently retract the soft tissues inferiorly, relaxes the anterior cervical and periscapular musculature, and provides an ergonomic working angle for the surgeon when addressing the superior aspect of the joint and the scapular spine.
A crucial, often overlooked step in positioning is the placement of a firm, folded sheet or specialized scapular bump medial to the medial border of the scapula. This maneuver effectively protracts the scapula, elevating it away from the thoracic cage and significantly improving access to the posterior aspect of the scapular spine for plate application. The operative arm must be draped completely free, from the clavicle down to the fingertips. This allows the surgeon to freely manipulate the upper extremity intraoperatively to achieve and rigorously maintain the precise angles of flexion, abduction, and internal rotation required for the optimal fusion position. If intraoperative fluoroscopy is utilized, the C-arm should be positioned at the head of the bed, capable of swinging in for true AP and axillary views without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Exposure
The surgical approach utilizes an extensile, S-shaped or "sabercut" incision designed to provide panoramic exposure of the entire shoulder girdle. The incision begins posteriorly, directly over the medial aspect of the spine of the scapula. It is carried laterally, tracing the subcutaneous border of the scapular spine toward the acromion. As the incision reaches the posterolateral corner of the acromion, it curves anteriorly, following the lateral border of the acromion. Finally, it extends distally down the anterolateral aspect of the arm, following the anterior border of the deltoid for approximately 10 to 15 centimeters.

Following the skin incision, dissection is carried down through the subcutaneous tissues to the deep fascia. Meticulous hemostasis is achieved using electrocautery. Skin flaps are elevated to expose the underlying deep structures. Posteriorly, the trapezius insertion onto the superior aspect of the scapular spine is identified. Using a periosteal elevator and electrocautery, a subperiosteal dissection is performed along the entire length of the scapular spine and the superior surface of the acromion. It is imperative to stay strictly subperiosteal to minimize bleeding and preserve the integrity of the overlying soft tissues, which will be required for robust closure over the bulky hardware.

Deep Dissection and Joint Exposure
Anteriorly, the deltopectoral interval is identified by locating the cephalic vein. The interval is developed, retracting the pectoralis major medially and the deltoid laterally. If the deltoid is functional, its anterior and lateral origins are carefully elevated off the acromion as a continuous subperiosteal sleeve, preserving its neurovascular supply from the axillary nerve. If the deltoid is definitively denervated, a direct muscle-splitting approach between the anterior and lateral heads provides rapid, direct access to the proximal humerus.

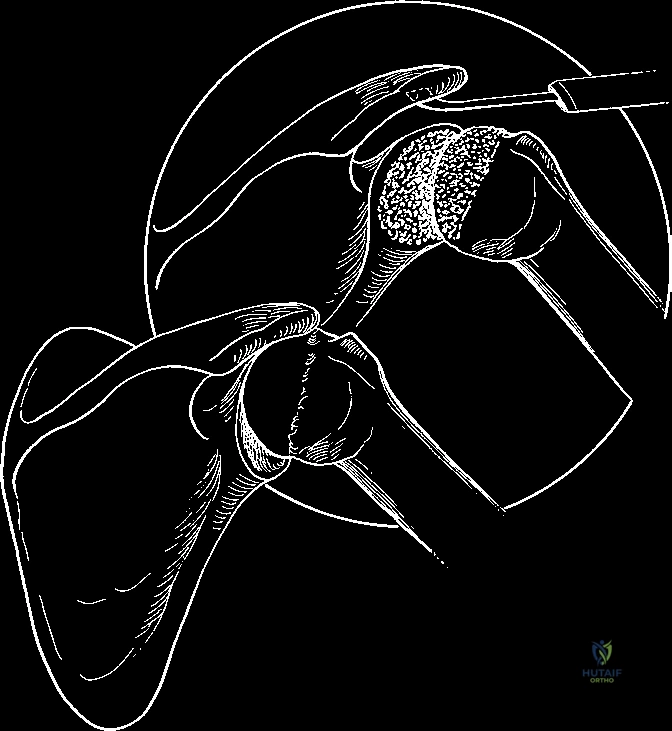
Once the proximal humerus is exposed, the long head of the biceps tendon is identified in the bicipital groove, tenotomized, and tenodesed to the pectoralis major. The underlying rotator cuff tendons—subscapularis anteriorly, supraspinatus superiorly, and infraspinatus/teres minor posteriorly—are systematically identified and excised. A complete capsulectomy is performed, releasing the humerus from the glenoid. A humeral head retractor or a Darrach retractor is placed carefully into the joint to subluxate the humeral head laterally, providing unencumbered visualization of the glenoid fossa.
Joint Preparation and Decortication
The preparation of the bony surfaces is the most critical biological step of the procedure. The goal is to create broad, flat, bleeding surfaces of healthy cancellous bone that maximize contact area. Using a high-speed burr, sharp osteotomes, and heavy curettes, the articular cartilage and subchondral bone plate of the glenoid fossa are completely removed down to bleeding cancellous bone. The concavity of the glenoid is flattened to accept the humeral head.

Attention is then turned to the proximal humerus. The articular surface of the humeral head is aggressively decorticated. Importantly, the decortication must extend superiorly to include the greater tuberosity. Simultaneously, the undersurface of the acromion is decorticated using a burr. This prepares the joint for the essential "double fusion" technique, where the humeral head is fused to the glenoid, and the greater tuberosity is fused to the undersurface of the acromion, drastically increasing the fusion mass and biomechanical stability.

Positioning, Plate Contouring, and Rigid Fixation
Achieving the optimal position of fusion is paramount for postoperative function. The historically accepted position, pioneered by Rowe, advocated for higher degrees of abduction. However, modern consensus dictates a more functional, relaxed position to prevent excessive scapular winging and allow the arm to rest comfortably at the side. The target position is 30 degrees of abduction, 30 degrees of forward flexion, and 30 degrees of internal rotation. This specific orientation allows the patient's hand to reach the mouth for feeding while enabling the arm to clear the torso during ambulation.
With the arm held rigidly in the target position by an assistant, preliminary fixation is achieved using two large-diameter (6.5-mm or 7.3-mm) cannulated lag screws. These screws are passed from the lateral cortex of the proximal humerus, across the decorticated joint space, and into the dense bone of the glenoid neck and coracoid base. These lag screws provide the primary interfragmentary compression across the arthrodesis site.
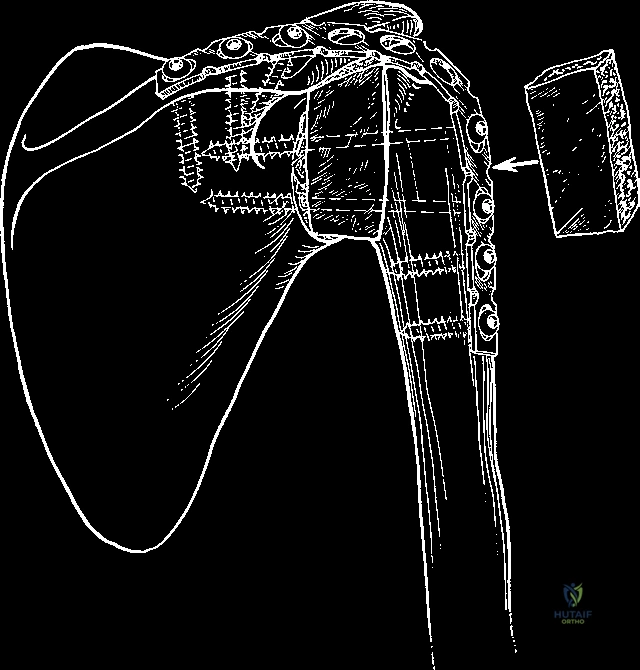
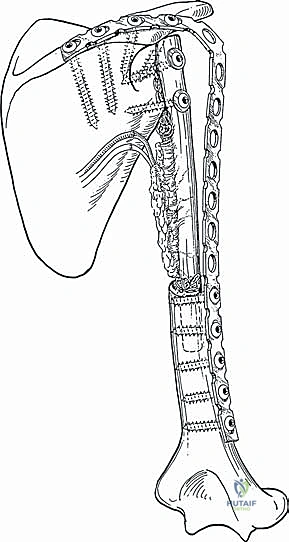
Following lag screw placement, the 4.5-mm pelvic reconstruction plate is meticulously contoured. This is a highly complex, three-dimensional bend. The plate must lie flat along the posterior aspect of the scapular spine, twist 90 degrees to contour over the superior aspect of the acromion, and then curve distally to sit flush against the lateral cortex of the humeral shaft.
Once perfectly contoured, the plate is secured. Screws are first placed into the scapular spine, ensuring bicortical purchase where possible, though caution must be exercised to avoid penetrating the suprascapular nerve in the suprascapular notch. The plate is then secured to the humeral shaft. If necessary, articulated tensioning devices can be used to apply additional compression across the fusion site before placing the final humeral screws.
Any remaining voids around the fusion site, particularly between the acromion and the humerus, are densely packed with autogenous cancellous bone graft harvested from the resected humeral head or the iliac crest. The wound is copiously irrigated, and the deltoid (if elevated) and trapezius are meticulously repaired over the hardware to provide robust soft tissue coverage.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, glenohumeral arthrodesis is fraught with potential complications, largely due to the massive biomechanical forces exerted on the relatively small fusion mass and the extensive soft tissue dissection required. The surgeon must be prepared to identify and manage these complications aggressively.
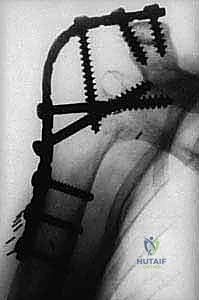
Nonunion and delayed union represent the most significant modes of mechanical failure, with historical incidence rates ranging from 5% to 15%. Risk factors include inadequate decortication, failure to achieve rigid intraoperative compression, smoking, and prior radiation therapy (in oncologic cases). A nonunion typically presents with persistent, localized pain, hardware failure (screw breakage or plate fracture), and a progressive loss of the carefully established fusion angle. Management of a symptomatic nonunion requires a major revision surgery, involving complete hardware removal, aggressive takedown of the fibrous pseudarthrosis, repeat decortication, application of massive structural iliac crest bone grafting, and revision internal fixation with dual orthogonal plating.
Hardware prominence and irritation are exceedingly common, particularly over the spine of the scapula and the acromion, where the soft tissue envelope is inherently thin. Up to 30% of patients may require symptomatic hardware removal once a solid, mature bony fusion has been radiographically and clinically confirmed (typically 12 to 18 months postoperatively). Deep periprosthetic infection is a catastrophic complication, occurring in 2% to 5% of cases, often necessitating aggressive surgical debridement, hardware removal (if the fusion is not yet solid, replacing it with an external fixator), and prolonged targeted intravenous antibiotic therapy.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion / Pseudarthrosis | 5% - 15% | Poor bone stock, inadequate compression, smoking, infection, prior radiation. | Revision open reduction, dual plating, massive autogenous iliac crest bone grafting. |
| Hardware Prominence/Pain | 20% - 30% | Thin soft tissue envelope over scapular spine/acromion; bulky 4.5mm plates. | Elective hardware removal only after CT confirmation of solid, mature arthrodesis (12-18 mos). |
| Hardware Failure (Fracture) | 5% - 10% | Fatigue failure of plate prior to bony union; noncompliance with immobilization. | Revision fixation, optimization of biomechanical construct, bone grafting. |
| Deep Joint Infection | 2% - 5% | Extensive exposure, prolonged OR time, immunocompromise, prior septic arthritis. | Aggressive I&D, potential hardware removal, temporary external fixation, IV antibiotics. |
| Neurologic Injury | < 2% | Iatrogenic traction or laceration of axillary or suprascapular nerves during exposure/drilling. | Observation for neuropraxia; nerve exploration/grafting if neurotmesis is suspected. |
Phased Post-Operative Rehabilitation Protocols
Phase I: Maximum Protection and Immobilization (Weeks 0-6)
