

Welcome, colleagues and fellows, to the operating theater. Today, we are tackling one of the most challenging yet profoundly rewarding pathologies in reconstructive shoulder surgery: glenohumeral arthritis in the setting of an irreparable rotator cuff defect. This condition demands a nuanced understanding of altered shoulder biomechanics, meticulous preoperative templating, and precise, unforgiving surgical execution. Our ultimate goal is the restoration of comfort and functional independence for patients whose quality of life has been severely compromised by chronic pain and pseudoparalysis.
Comprehensive Introduction and Patho-Epidemiology
Glenohumeral arthritis in the presence of an irreparable rotator cuff tear represents an end-stage degenerative cascade that fundamentally alters the kinematics of the shoulder joint. To understand the pathology, we must first define our terms with academic rigor. Glenohumeral arthritis is characterized by the irreversible loss of the normal hyaline articular cartilage covering the humeral head and the glenoid fossa. While this can stem from various etiologies—including primary osteoarthritis, rheumatoid arthritis, neurotrophic arthropathy, septic arthritis, or avascular necrosis—the presence of a massive, unrepairable rotator cuff defect introduces a unique and devastating mechanical variable.
A specific and highly complex presentation of this combination is rotator cuff tear arthropathy (CTA). In this condition, the articular cartilage loss is directly compounded by chronic rotator cuff deficiency. The defining characteristic of CTA is the progressive superior migration of the humeral head, leading to chronic abrasion of the unprotected proximal humerus against the undersurface of the coracoacromial arch. This progressive, unmitigated friction creates a distinct clinical and radiographic picture, originally described by Charles Neer, characterized by "femoralization" of the humeral head and "acetabularization" of the coracoacromial arch.
An irreparable rotator cuff defect is defined clinically and intraoperatively as a scenario where a durable, tension-free footprint restoration of the detached cuff tendons to the tuberosities cannot be achieved, despite maximal soft tissue mobilization. These defects arise when the chronic loads applied to the tendon insertion vastly exceed the intrinsic strength of the degenerated tendon-bone interface. Over time, the retracted tendons undergo irreversible fatty infiltration and muscle atrophy (Goutallier stage 3 or 4), rendering them functionally inert even if anatomically approximated.
When the superior rotator cuff (primarily the supraspinatus) is deficient, a critical biomechanical destabilization occurs. The normal "spacer effect" of the supraspinatus tendon is lost, effectively decreasing the functional radius of the proximal humeral convexity. Without the compressive, inferiorly directed force vector of the intact rotator cuff, the humeral head translates superiorly under the unopposed active pull of the deltoid muscle. This superior migration continues until the uncovered humeral head directly contacts and articulates with the acromion and coracoacromial ligament, a hallmark sign of cuff tear arthropathy that dictates our surgical decision-making.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel touches the skin, a profound, three-dimensional understanding of the relevant surgical anatomy and the altered biomechanics of the cuff-deficient shoulder is paramount. The glenohumeral joint is a diarthrodial, ball-and-socket articulation characterized by a massive mismatch in articular surface area. The glenoid fossa is a shallow, pear-shaped concavity, approximately one-quarter the size of the humeral head, relying heavily on the fibrocartilaginous labrum and the dynamic compression of the rotator cuff for stability. The humeral head is a smooth, spherical convexity designed for extreme ranges of motion at the expense of intrinsic bony stability.

The rotator cuff is a complex musculotendinous unit comprising the subscapularis, supraspinatus, infraspinatus, and teres minor. In a healthy shoulder, these muscles function as a dynamic force couple. The coronal plane force couple balances the superior pull of the deltoid with the inferior pull of the inferior cuff, keeping the humeral head centered on the glenoid during elevation. The transverse plane force couple balances the anterior pull of the subscapularis with the posterior pull of the infraspinatus and teres minor. When massive, irreparable tearing occurs, these force couples are uncoupled. The loss of the coronal force couple leads to superior migration, while the loss of the transverse force couple (especially if the anterior subscapularis or posterior infraspinatus is involved) leads to anterosuperior or posterosuperior escape.
The coracoacromial arch acts as the secondary, and in the case of CTA, the primary superior stabilizer of the glenohumeral joint. It consists of the undersurface of the acromion, the coracoid process, and the strong coracoacromial ligament spanning between them. In cuff tear arthropathy, the proximal humerus relies entirely on this arch to provide a fulcrum for the deltoid to elevate the arm. If this arch is iatrogenically compromised (e.g., by a prior aggressive acromioplasty or coracoacromial ligament release), the humeral head will undergo anterosuperior escape upon deltoid contraction—a devastating functional deficit that renders conventional hemiarthroplasty completely contraindicated and necessitates a constrained reverse total shoulder arthroplasty (rTSA).

Navigating the neurovascular landscape during exposure is critical. The axillary nerve is arguably the most vulnerable structure during shoulder arthroplasty. Arising from the posterior cord (C5-C6), it courses anterior to the subscapularis, passes inferior to the glenohumeral joint capsule, and exits through the quadrilateral space. It is highly susceptible to traction injury during inferior capsular release or aggressive retraction of the deltoid. The musculocutaneous nerve, entering the conjoint tendon 3-5 cm distal to the coracoid, is at risk during medial retraction. The suprascapular nerve, passing through the suprascapular and spinoglenoid notches, can be tethered or injured during extensive posterior capsular releases or glenoid preparation.

Exhaustive Indications and Contraindications
The decision to proceed with glenohumeral arthroplasty in the setting of an irreparable rotator cuff tear requires a meticulous evaluation of the patient's symptoms, physiological age, functional demands, and remaining bone stock. Historically, Cuff Tear Arthropathy (CTA) hemiarthroplasty using a large-diameter humeral head to articulate with the acromion was the standard of care. Today, Reverse Total Shoulder Arthroplasty (rTSA) is the gold standard for patients with true pseudoparalysis, as it medialize and distalizes the center of rotation, tensioning the deltoid and restoring active elevation without relying on the rotator cuff.
Indications for arthroplasty in this population center on debilitating, refractory pain that has failed exhaustive conservative management, including targeted physical therapy, non-steroidal anti-inflammatory drugs, and judicious intra-articular corticosteroid injections. A primary indication is the presence of "pseudoparalysis"—the inability to actively elevate the arm above 90 degrees despite a neurologically intact deltoid, caused entirely by the loss of a stable mechanical fulcrum. Furthermore, severe radiographic evidence of glenohumeral joint destruction, superior humeral migration, and acetabularization of the acromion solidify the surgical indication.
Contraindications must be respected to avoid catastrophic failure. Absolute contraindications include active or recent deep glenohumeral infection, neuropathic (Charcot) arthropathy, and a non-functioning deltoid muscle (e.g., due to severe axillary nerve palsy). Without a functioning deltoid, even a reverse prosthesis will fail to restore active elevation and will likely result in a highly unstable joint. Relative contraindications include severe physiological age or medical comorbidities that preclude safe anesthesia, profound glenoid bone loss that cannot be addressed with structural grafting or augmented baseplates, and a history of non-compliance with postoperative rehabilitation protocols.
Below is a detailed breakdown of indications and contraindications for arthroplasty in the cuff-deficient shoulder:
| Category | Specific Condition | Clinical Significance & Arthroplasty Consideration |
|---|---|---|
| Absolute Indications | End-stage CTA with intractable pain | Primary driver for surgical intervention; rTSA highly effective for pain relief. |
| Absolute Indications | Pseudoparalysis with intact deltoid | rTSA is the only arthroplasty option that restores the mechanical fulcrum for elevation. |
| Absolute Indications | Anterosuperior escape | Indicates complete loss of the coracoacromial arch; rTSA is mandatory to capture the humerus. |
| Relative Indications | Elderly patient with low demands | CTA Hemiarthroplasty may be considered if elevation is preserved and pain is the only symptom, though rTSA is generally preferred. |
| Absolute Contraindications | Active joint infection | High risk of prosthetic joint infection (PJI); requires two-stage revision protocol. |
| Absolute Contraindications | Absent/Paralyzed Deltoid | Arthroplasty (especially rTSA) will fail functionally and is at high risk for dislocation. |
| Relative Contraindications | Severe Glenoid Bone Loss | May require complex structural bone grafting or custom augmented baseplates; increases surgical complexity and failure risk. |
| Relative Contraindications | Young, high-demand laborer | High risk of early component loosening or polyethylene wear; joint-preserving salvage procedures (e.g., superior capsular reconstruction) may be considered first. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful arthroplasty. Standardized radiographs are mandatory, including a true anteroposterior (Grashey) view, an axillary lateral view, and a scapular Y view. These allow for the initial assessment of superior migration, acromial wear, and gross glenoid morphology. However, plain films are insufficient for definitive planning in complex cuff-deficient shoulders.

A non-contrast fine-cut Computed Tomography (CT) scan with three-dimensional reconstructions is the gold standard for evaluating glenoid bone stock. In chronic CTA, the glenoid often exhibits preferential superior and posterior wear (Walch classification modifications). Advanced 3D templating software is now routinely utilized to virtually position the glenoid baseplate (in rTSA) or assess the native version and inclination. This software allows the surgeon to anticipate the need for eccentric reaming, augmented baseplates, or structural bone grafting to achieve neutral version and secure fixation. Magnetic Resonance Imaging (MRI) is less critical for bone planning but is invaluable for assessing the degree of fatty infiltration in the remaining rotator cuff musculature (Goutallier staging) and confirming the status of the teres minor, which dictates postoperative external rotation capacity.

Patient positioning is a critical intraoperative step. The beach chair position is overwhelmingly preferred for shoulder arthroplasty. The patient is positioned with the backrest elevated to approximately 45 to 60 degrees, with the hips and knees flexed to prevent sciatic nerve stretch and venous pooling. The operative shoulder must be positioned completely off the edge of the table to allow for unrestricted extension and adduction of the arm, which is absolute necessary for adequate humeral exposure and preparation. A specialized head positioner is used to maintain neutral cervical alignment, and all bony prominences are meticulously padded.
Anesthesia typically involves a combination of regional and general techniques. An interscalene brachial plexus block provides excellent perioperative analgesia, significantly reducing the requirement for volatile anesthetics and systemic opioids. General anesthesia with an endotracheal tube is standard, ensuring airway security during positioning and allowing for controlled hypotension if necessary to minimize blood loss. The anesthesiologist must be aware of the surgical steps, particularly during cementing or component impaction, to monitor for embolic events.
Step-by-Step Surgical Approach and Fixation Technique
The standard workhorse approach for glenohumeral arthroplasty is the deltopectoral approach. This internervous plane utilizes the interval between the deltoid (axillary nerve) and the pectoralis major (medial and lateral pectoral nerves). The skin incision begins at the tip of the coracoid process and extends distally and laterally toward the deltoid tuberosity, following the path of the cephalic vein.

Upon incising the superficial fascia, the cephalic vein is identified. It is typically retracted laterally with the deltoid to preserve its venous drainage, though medial retraction is acceptable if the anatomy dictates. The deltopectoral interval is developed bluntly. The clavipectoral fascia is then incised lateral to the conjoint tendon. At this stage, a self-retaining retractor is placed. It is imperative to identify and protect the axillary nerve, which can be palpated by sweeping a finger down the anterior surface of the subscapularis and hooking it under the inferior capsule.

Management of the subscapularis is a critical decision point. In the setting of an irreparable supraspinatus/infraspinatus, the subscapularis may be intact, partially torn, or completely deficient. If intact, it must be mobilized for joint access. Options include a subscapularis peel off the lesser tuberosity, a tenotomy 1 cm medial to the insertion, or a lesser tuberosity osteotomy. For rTSA, many surgeons prefer a peel or tenotomy, as robust repair is less critical for stability than in anatomic TSA, though repair is still attempted to enhance internal rotation strength. Following subscapularis mobilization, a thorough 360-degree capsular release is performed to mobilize the proximal humerus, paying strict attention to protecting the axillary nerve inferiorly.

Humeral preparation begins with dislocation of the humeral head into the deltopectoral interval, achieved by extension, adduction, and external rotation of the arm. Osteophytes are removed to identify the true anatomic neck. The humeral cut is made using an extramedullary or intramedullary cutting guide. The version of the cut is typically 20 to 30 degrees of retroversion relative to the forearm axis. In rTSA, the cut is often more horizontal (e.g., 135 to 145 degrees neck-shaft angle) compared to the anatomic 135-150 degrees, depending on the specific implant design.


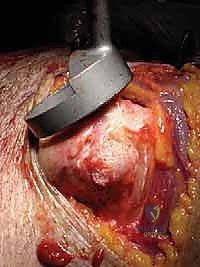
Once the humerus is resected and protected with a cut protector, attention turns to the glenoid. Deep retractors (e.g., a Fukuda retractor posteriorly, a Darrach anteriorly) are placed. The labrum is completely excised. For a CTA hemiarthroplasty, the glenoid is simply debrided of loose cartilage and left alone, or concentrically reamed to match the humeral component. For a rTSA, the glenoid is the foundation of the reconstruction. A central guide pin is placed, aiming for inferior tilt to prevent baseplate superior tilt and subsequent scapular notching. The glenoid is reamed to bleeding subchondral bone.


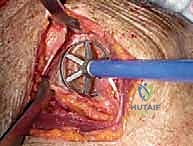
The baseplate is then impacted and secured with locking and non-locking screws, achieving rigid primary fixation. The glenosphere is then impacted onto the baseplate via a Morse taper. Attention returns to the humerus, where the canal is prepared with sequential broaches. The trial humeral stem and epiphyseal components are inserted.

Trialing is arguably the most critical step to ensure stability and appropriate deltoid tension. The joint is reduced, and stability is assessed through a full range of motion. We look for adequate conjoint tendon tension, lack of impingement between the humeral component and the scapular pillar (which leads to notching), and stability in adduction and internal rotation.


Once trialing is satisfactory, the definitive humeral stem is implanted (cemented or press-fit, depending on bone quality and stem design), and the final polyethylene liner is impacted. The joint is reduced one final time. The subscapularis is repaired if possible using heavy non-absorbable sutures through transosseous drill holes. The deltopectoral interval is closed over a suction drain, followed by layered closure of the subcutaneous tissue and skin.


Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, glenohumeral arthroplasty in the cuff-deficient shoulder carries a distinct and significant complication profile. The altered biomechanics and often compromised soft tissue envelope make these patients particularly vulnerable. Thorough preoperative counseling regarding these risks is mandatory.
Instability remains a primary concern, particularly in rTSA. Dislocation occurs in approximately 2% to 5% of primary reverse arthroplasties. It is often multifactorial, stemming from inadequate deltoid tensioning, failure to repair the subscapularis, or impingement of the humeral cup against the scapular neck during adduction. If closed reduction fails or if instability is recurrent, revision surgery to upsize the glenosphere, increase the humeral liner thickness, or address mechanical impingement is required.
Infection is a devastating complication, occurring in 1% to 3% of cases. Cutibacterium acnes (C. acnes) is a particularly insidious pathogen in shoulder arthroplasty, often presenting months to years postoperatively with vague pain, stiffness, and subtle radiographic loosening, without systemic signs of infection. Diagnosis requires multiple deep tissue cultures held for at least 14 days. Management typically involves a two-stage revision protocol: explantation, radical debridement, placement of an antibiotic-loaded cement spacer, intravenous antibiotics, and subsequent reimplantation once the infection is eradicated.
Scapular notching is a complication unique to rTSA, where the medial edge of the humeral polyethylene cup abrades the inferior scapular neck during adduction. While modern implant designs (lateralized glenospheres, lower neck-shaft angles) have reduced its incidence from historical highs of >50% to roughly 10-20%, severe notching can lead to polyethylene wear debris, osteolysis, and eventual baseplate failure. Another unique complication is an acromial or scapular spine stress fracture, occurring in 1-3% of rTSA patients due to the sudden increase in deltoid tension.
| Complication | Estimated Incidence | Etiology/Risk Factors | Salvage/Management Strategy |
|---|---|---|---|
| Instability / Dislocation | 2% - 5% | Inadequate deltoid tension, mechanical impingement, subscapularis failure. | Closed reduction under anesthesia; Revision to thicker liner or larger glenosphere if recurrent. |
| Periprosthetic Joint Infection (PJI) | 1% - 3% | C. acnes colonization, prior surgeries, hematoma formation. | Two-stage revision with antibiotic spacer; lifelong suppression in high-risk/elderly patients. |
| Scapular Notching | 10% - 20% | Superior baseplate placement, medialized center of rotation, impingement in adduction. | Observation for low grades; Revision arthroplasty with lateralized/inferiorized baseplate for severe osteolysis. |
| Acromial Stress Fracture | 1% - 3% | Over-tensioning of the deltoid, severe osteoporosis. | Conservative management (sling immobilization) initially; ORIF if significantly displaced and symptomatic. |
| Nerve Injury (Axillary) | < 1% | Traction during inferior capsular release or excessive deltoid retraction. | Observation and EMG at 3 months; nerve exploration/grafting if no recovery by 6 months. |

Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be carefully tailored to the specific type of arthroplasty performed (CTA hemiarthroplasty vs. rTSA) and the intraoperative status of the soft tissues, particularly the subscapularis repair. Communication between the operative surgeon and the physical therapy team is absolutely critical to prevent early failure.
Phase I (Weeks 0-4) focuses on strict protection of the surgical repair while allowing for early, safe mobilization to prevent adhesive capsulitis. The patient is immobilized in a standard shoulder sling. For rTSA, if the subscapularis was repaired, external rotation is strictly limited to neutral or 10 degrees to protect the repair. Passive range of motion (PROM) exercises in forward elevation and scaption are initiated immediately, usually limited to 90-120 degrees based on intraoperative stability testing. Active use of the hand, wrist, and elbow is encouraged to prevent distal edema.
Phase II (Weeks 4-8) marks the transition to active-assisted range of motion (AAROM) and the gradual weaning of the sling. The sling is typically discontinued around week 4 to 6. Patients begin using pulleys, wand exercises, and wall-walks to actively assist their elevation. In rTSA, the focus begins to shift toward recruiting and strengthening the anterior and middle deltoid, which now acts as the primary elevator of the arm. Isometrics for the deltoid and periscapular stabilizers are introduced.
Phase III (Weeks 8-12 and beyond) involves the progression to full active range of motion (AROM) and graduated resistance training. Theraband exercises and light weights are incorporated. The ultimate goal is maximizing active forward elevation and functional internal/external rotation. It is important to counsel patients that maximal medical improvement following complex shoulder arthroplasty often takes 12 to 18 months. Patients are generally advised to avoid heavy lifting (greater than 15-20 lbs) and repetitive overhead impact activities indefinitely to protect the longevity of the prosthesis.

Detailed Chapters & Topics
Dive deeper into specialized chapters regarding hemiarthroplasty-and-total-shoulder-arthroplasty-for-glenohumeral-arthritis-with-an-irreparable-rotator-cuff