Glenoid Augmentation with Autologous Iliac Crest Bone Graft: A Masterclass in Anterior Shoulder Instability Management
Key Takeaway
Join our masterclass on glenoid bone grafting for anterior shoulder instability with bone loss. We'll meticulously cover patient selection, preoperative planning, and the precise deltopectoral approach. Learn to expertly harvest tricortical iliac crest graft, prepare the glenoid, and secure the graft, emphasizing critical anatomical landmarks and neurovascular protection to restore stability and prevent recurrence.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues, to the operating theater. Today, we are tackling a challenging but critical procedure in the realm of shoulder reconstruction: anterior glenoid augmentation utilizing an autologous iliac crest bone graft (ICBG) for the management of recurrent shoulder instability complicated by significant bone loss. This intervention transcends standard soft tissue repair; it represents a fundamental structural restoration of the glenohumeral articulation. Precision, thorough preoperative planning, and meticulous surgical execution are paramount to achieving a stable, functional, and durable joint.
Anterior shoulder instability represents a complex cascade of pathological events initiated by injury to the intricate network of the capsule, ligaments, and labrum that dynamically and statically stabilize the glenohumeral joint. While a structurally intact glenoid possesses a characteristic pear-like morphology that provides a broad, stable, concave platform for the humeral head, high-energy traumatic events or chronic, recurrent dislocations inevitably lead to progressive anterior glenoid rim erosion or frank fracture. This bony attrition fundamentally alters the biomechanical environment of the shoulder, rendering isolated soft-tissue stabilization procedures, such as an arthroscopic Bankart repair, highly susceptible to failure.
The epidemiological profile of patients requiring this advanced reconstruction typically includes young, high-demand, or contact athletes, as well as individuals with a history of failed prior stabilization surgeries. In these populations, the sheer kinetic energy transferred across the joint during athletic endeavors or subsequent dislocation events rapidly accelerates bone loss. Recognizing the critical threshold of this bone loss is the cornerstone of modern shoulder instability management. When the structural deficit exceeds the compensatory capacity of the soft tissues, anatomical restoration with a structural bone graft becomes not merely an option, but an absolute biomechanical necessity.
Historically, the Eden-Hybinette procedure laid the foundation for utilizing iliac crest autograft in shoulder stabilization. Today, refined techniques, advanced fixation methods, and a deeper understanding of glenohumeral kinematics have elevated this procedure to a masterclass level. Unlike the Latarjet procedure, which relies on a combined sling effect and coracoid transfer, the ICBG augmentation is a pure anatomic reconstruction of the glenoid arc. This chapter will exhaustively detail the patho-anatomy, preoperative evaluation, precise surgical technique, and postoperative protocols required to master this indispensable procedure.
Detailed Surgical Anatomy and Biomechanics
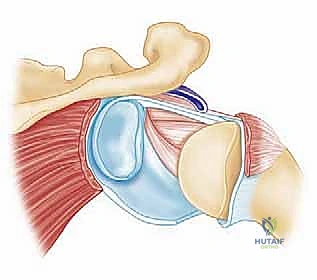
Shoulder stability is orchestrated by a complex, synchronized symphony of both dynamic and static stabilizers. Understanding the interplay of these forces is essential for any reconstructive shoulder surgeon. Dynamic stabilizers encompass the rotator cuff musculature (supraspinatus, infraspinatus, teres minor, and subscapularis), the long head of the biceps tendon, coordinated scapulothoracic rhythm, and intact neuromuscular proprioception. These muscular forces generate crucial "concavity compression," a biomechanical phenomenon where the dynamic contraction of the cuff compresses the convex humeral head securely into the concave glenoid vault and its surrounding labral bumper.
The static stabilizers form the unyielding foundation of the joint. These include the bony architecture of the glenoid and humeral head, the fibrocartilaginous labrum, and the glenohumeral capsule with its distinct ligamentous thickenings. Among these, the inferior glenohumeral ligament (IGHL) complex is paramount. Originating from the inferior aspect of the glenoid labrum, the IGHL serves as the primary anterior restraint when the arm is in the vulnerable position of abduction and external rotation. It is anatomically divided into an anterior band, a posterior band, and an intervening axillary pouch, functioning much like a hammock to cradle the humeral head.
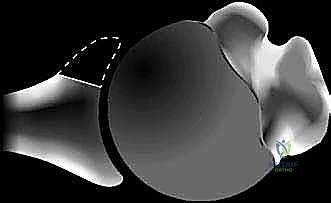
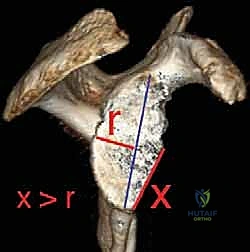
When traumatic events compromise the anterior glenoid bone, the critical concavity depth and surface area are precipitously lost. Biomechanical studies have demonstrated that even a 20% loss of anterior glenoid width significantly decreases the force required to translate the humeral head anteriorly. The morphological consequence of this erosion is the classic "inverted pear" glenoid, a pathognomonic sign where the inferior transverse diameter of the glenoid becomes narrower than the superior diameter.

This "inverted pear" morphology completely disrupts the normal mechanism of concavity-compression. The glenoid can no longer effectively capture the humeral head, leading to persistent, low-energy instability—often occurring with minimal trauma or even during sleep. Furthermore, the loss of the anterior bony buttress places exponential stress on any soft-tissue repair, leading to stretching, attenuation, and inevitable failure of Bankart repairs. The primary objective of the iliac crest bone grafting procedure is to restore the native glenoid arc, reconstitute the bony buttress, and re-establish the foundation for effective concavity-compression.
Exhaustive Indications and Contraindications
Before committing to a complex structural reconstruction, a rigorous clinical and radiographic evaluation is mandatory to confirm the indications and rule out contraindications. The diagnostic compass begins with a meticulous history and physical examination. The Apprehension Test is the hallmark of anterior instability; however, the surgeon must differentiate true apprehension (the patient's imminent fear of subluxation) from mere anterior shoulder pain. The Relocation Test, characterized by the relief of apprehension upon applying a posteriorly directed force on the proximal humerus, solidifies the diagnosis.
Furthermore, the Load and Shift Test is critical for quantifying the degree of glenohumeral translation and assessing for multidirectional laxity, which requires a distinct treatment algorithm. Evaluation of the subscapularis via the Belly Press Test and Lift-Off Sign is vital, as subscapularis insufficiency can exacerbate anterior instability and complicate the surgical approach. Finally, a thorough neurological assessment, particularly of the axillary nerve, must be documented, as chronic instability or prior surgical interventions can lead to subtle neuropathies.
The decision to proceed with an autologous iliac crest bone graft hinges heavily on the quantification of bone loss. While the Latarjet procedure is a highly effective alternative, ICBG is specifically indicated in cases of massive glenoid bone loss (>25-30%), revision scenarios where the coracoid has already been harvested or is hypoplastic, or when the surgeon wishes to avoid the anatomical distortions associated with a Latarjet.
| Parameter | Indications for Autologous ICBG Augmentation | Absolute & Relative Contraindications |
|---|---|---|
| Bone Loss Threshold | Anterior glenoid bone loss > 20-25% of the inferior glenoid diameter. | Minimal bone loss (< 15%) amenable to isolated soft-tissue Bankart repair. |
| Morphology | Presence of an "inverted pear" glenoid on 3D CT reconstruction. | Multidirectional instability without discrete structural bone loss. |
| Clinical History | Recurrent instability with failed prior soft-tissue stabilization (e.g., failed Bankart). | Active local or systemic infection (Absolute). |
| Associated Lesions | Engaging Hill-Sachs lesion (bipolar bone loss) requiring increased glenoid arc. | Severe glenohumeral osteoarthritis (Outerbridge Grade III/IV) (Absolute). |
| Patient Profile | High-demand contact athletes (rugby, American football, martial arts). | Medical non-compliance or inability to adhere to strict postoperative rehabilitation protocols (Relative). |
| Anatomical Factors | Previous failed Latarjet or hypoplastic/fractured coracoid process. | Advanced physiological age with low functional demands (Relative). |
Pre-Operative Planning, Templating, and Patient Positioning
Surgical success is dictated long before the initial incision is made. Preoperative planning requires a comprehensive radiographic series. Plain radiographs, including a true anteroposterior (AP) view of the glenoid (Grashey view), an axillary lateral, and a Stryker notch view, provide the initial assessment of glenohumeral congruity, Hill-Sachs lesions, and obvious anterior rim fractures. However, plain films are insufficient for precise surgical templating.
A definitive assessment demands a high-resolution CT arthrogram or a non-contrast CT with 3D reconstructions with digital subtraction of the humeral head. This imaging modality is the gold standard for quantifying glenoid bone loss. We employ established measurement techniques, such as the Pico method or Gerber’s index, utilizing the en face view of the glenoid. By drawing a best-fit circle over the inferior intact posterior glenoid and measuring the anterior defect relative to this circle, we can accurately calculate the percentage of bone loss and determine the exact dimensions (length, width, and depth) of the required iliac crest graft.

Proper patient positioning is critical to facilitate simultaneous access to both the shoulder and the iliac crest. We strongly advocate for the beach chair position utilizing an attachable hydraulic articulated arm holder, such as the Spider Limb Positioner. The head of the operating table is elevated to approximately 30 to 45 degrees. This semi-upright orientation provides unparalleled visualization of the anterior glenohumeral joint while allowing gravity to assist in retracting the soft tissues.
A well-padded bump is strategically placed beneath the ipsilateral buttock and hip. This maneuver elevates the anterior superior iliac spine (ASIS) and the iliac crest, rendering them prominent and easily accessible for a minimally traumatic graft harvest. The arm holder is indispensable; it allows the surgical assistant to safely and dynamically manipulate the arm throughout the procedure—facilitating exposure during the approach, aiding in joint reduction, and allowing for intraoperative assessment of stability and range of motion once the graft is secured. Both the entire forequarter and the ipsilateral hemipelvis are meticulously prepped and draped in a standard sterile fashion.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution involves two distinct, yet seamlessly integrated, operative fields: the deltopectoral approach for glenohumeral exposure and the anterior iliac crest approach for graft harvesting. We typically begin with the shoulder exposure to accurately assess the defect in vivo before harvesting the graft.
Navigating the Deltopectoral Interval
We initiate the procedure with a precise 5- to 7-cm curvilinear incision along the anterior axillary fold, beginning at the inferior border of the pectoralis major tendon and extending superiorly toward the coracoid process. This incision follows Langer's lines to optimize postoperative cosmesis. Using a no. 15 blade, full-thickness skin flaps are sharply developed and extended superiorly to the coracoid and medially/laterally to expose the underlying fascia.
The deltopectoral interval is identified by locating the cephalic vein, which serves as the primary anatomical landmark navigating the cleavage plane between the deltoid laterally and the pectoralis major medially. We prefer to incise the investing fascia sharply on the medial aspect of the cephalic vein, retracting the vein laterally with the deltoid to preserve its venous drainage and minimize postoperative edema. Meticulous hemostasis of the medially based crossing vessels is achieved with electrocautery.
Once the interval is opened, the deep surfaces of the deltoid and pectoralis muscles are freed from underlying adhesions. A four-quadrant self-retaining retractor, such as a Kolbel retractor, is positioned to maintain broad exposure. The conjoined tendon (short head of the biceps and coracobrachialis) is identified and retracted medially, taking immense care to protect the musculocutaneous nerve, which typically enters the coracobrachialis 3 to 5 cm distal to the coracoid tip.

Subscapularis Management and Capsular Exposure
Management of the subscapularis is a critical decision point. While a formal tenotomy provides excellent exposure, it carries a higher risk of postoperative weakness and fatty infiltration. Therefore, we strongly advocate for a subscapularis split (the Latarjet approach) or an L-shaped tenotomy leaving the inferior third intact. The split is performed horizontally at the junction of the middle and inferior thirds of the muscle belly, extending from the lesser tuberosity medially to the glenoid neck.

Deep to the subscapularis, the underlying capsule is carefully dissected free. A vertical capsulotomy is performed roughly 1 cm lateral to the glenoid rim. If necessary, a T-shaped extension can be added horizontally to enhance superior and inferior visualization. Tagging sutures (e.g., #2 FiberWire) are placed in the medial and lateral capsular leaflets to maintain control and facilitate the subsequent repair.

Glenoid Preparation
With the joint open, a Fukuda retractor is placed to subluxate the humeral head posteriorly, providing a direct, en face view of the anterior glenoid defect. The remaining anterior labrum and any fibrous scar tissue filling the bony defect are sharply excised.
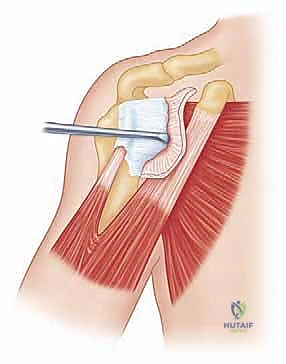
The anterior glenoid neck must be meticulously prepared to create a flat, bleeding cancellous bone bed. This is achieved using a high-speed burr or a sharp osteotome to decorticate the anterior neck. The prepared surface must be perfectly flat to ensure maximum cortical contact and subsequent osteointegration of the iliac crest graft. Any convexity will lead to a rocking motion of the graft, predisposing the construct to nonunion and failure.
Iliac Crest Bone Graft Harvest
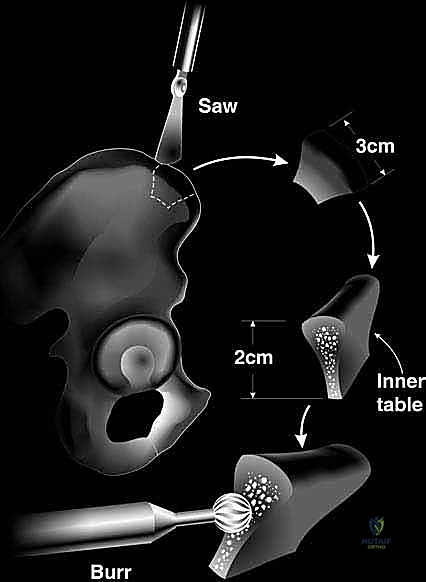
Attention is then turned to the ipsilateral iliac crest. An incision is made approximately 2 cm posterior to the ASIS to avoid injury to the lateral femoral cutaneous nerve (LFCN). The dissection is carried down through the subcutaneous tissue to the fascia over the iliac crest. The fascia is incised sharply, and the gluteal muscles are elevated subperiosteally off the outer table, while the iliacus is elevated off the inner table.

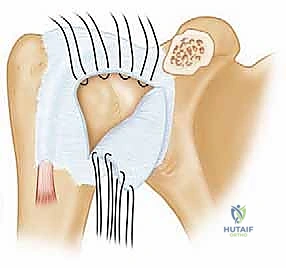
Using an oscillating saw and sharp osteotomes, a tricortical bone block is harvested. The dimensions are dictated by our preoperative CT templating and intraoperative measurements of the glenoid defect, typically measuring approximately 2.5 cm in length, 1.5 cm in depth, and 1.5 cm in width. The inner table of the ilium will eventually articulate with the humeral head, as its natural concavity closely mimics the native glenoid arc.

Graft Preparation and Contouring
Once harvested, the graft is brought to the back table for meticulous contouring. The inner table (concave side) is preserved to match the articular surface. The cancellous surface of the graft, which will interface with the decorticated glenoid neck, is flattened using a rasp or burr to ensure absolute congruity.
Two parallel drill holes are created in the graft using a 2.5 mm drill bit, spaced approximately 1 cm apart. These holes are overdrilled with a 3.5 mm bit to allow for a lag effect during screw fixation. The outer cortical surface of the graft is lightly countersunk to ensure the screw heads do not protrude into the soft tissues or impinge on the joint capsule.

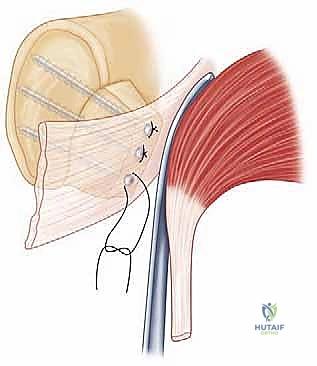
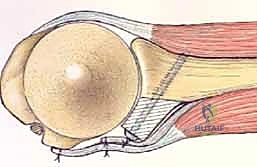
Graft Fixation and Capsular Repair
The contoured graft is introduced into the shoulder and positioned against the prepared anterior glenoid neck. It is absolutely critical that the lateral edge of the graft is positioned perfectly flush with, or 1 to 2 mm medial to, the native glenoid articular cartilage. If the graft overhangs laterally, it will cause rapid, catastrophic abrasion of the humeral head cartilage, leading to early-onset osteoarthritis.
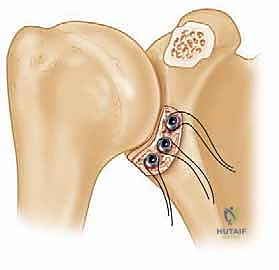
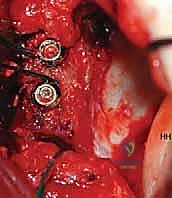
The graft is provisionally held in place with two Kirschner wires. The position is verified both visually and palpably. Once the position is deemed perfect, the K-wires are overdrilled into the native glenoid vault.
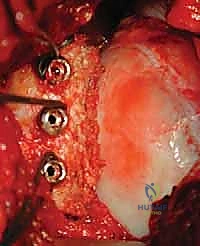
Two 3.5 mm or 3.75 mm fully threaded, cannulated titanium or stainless steel screws are inserted over the wires. The screws must achieve bicortical purchase in the posterior glenoid vault to ensure maximum pull-out strength. The screws are tightened sequentially to provide rigid,
Clinical & Radiographic Imaging Archive