Hallux Rigidus: Dorsal Cheilectomy, Plantar Release, and Microfracture Masterclass
Key Takeaway
Welcome to the OR, fellows. Today, we're tackling Hallux Rigidus with a comprehensive dorsal cheilectomy, extensive plantar release, and microfracture. This masterclass will guide you through precise anatomy, meticulous surgical steps, critical pearls, and post-operative strategies for optimal patient outcomes. Understand the nuances of first MTP joint arthrosis management.
Comprehensive Introduction and Patho-Epidemiology
Hallux rigidus, representing osteoarthrosis of the first metatarsophalangeal (MTP) joint, is a highly prevalent and functionally debilitating condition that frequently presents to the orthopedic foot and ankle surgeon. Originally described in the surgical literature by Cotterill and Davies-Colley in 1887 as "hallux flexus," the nomenclature has evolved to reflect the pathognomonic stiffness that characterizes the disease. It stands as the second most common deformity of the first ray, superseded only by hallux valgus. Epidemiological data indicate that nearly 10% of the adult population will experience symptomatic hallux rigidus, with a distinct female predilection and a peak onset typically occurring in the fifth and sixth decades of life.
The pathophysiological mechanisms driving hallux rigidus are multifactorial and, in some aspects, remain a subject of academic debate. The classic paradigm implicates repetitive microtrauma or a distinct hyperextension injury—colloquially termed "turf toe"—which disrupts the chondral surface and initiates a degenerative cascade. Historically, metatarsus primus elevatus (an elevated first metatarsal relative to the lesser metatarsals) was considered a primary etiologic factor; however, contemporary weight-bearing radiographic analyses suggest this may be a secondary radiographic artifact rather than a primary driver. Other implicated factors include a disproportionately long first metatarsal, focal osteochondral lesions, and restrictive footwear that places non-physiologic shear stress on the dorsal articular cartilage during the terminal stance phase of gait.

Interestingly, rigorous kinematic and anatomical studies have largely debunked previously held associations between hallux rigidus and generalized first ray hypermobility, Achilles tendon contracture, or baseline pes planus. What is clinically evident, however, is a strong genetic predisposition, particularly in patients presenting with bilateral, insidious-onset disease. Conversely, unilateral presentations are highly correlated with a history of direct trauma to the MTP complex. As the articular cartilage degrades, the joint undergoes characteristic osteoarthritic changes: progressive subchondral bone sclerosis, joint space narrowing, and the formation of robust periarticular osteophytes.
The biomechanical consequence of this degenerative process is profound. The contact distribution of the first MTP joint naturally shifts dorsally during hallux extension. As dorsal osteophytes proliferate, they create a mechanical block to dorsiflexion, leading to dorsal impingement. This impingement not only restricts motion but also exponentially increases focal compressive forces on the remaining dorsal cartilage, accelerating chondral erosion. Left untreated, the natural history is one of inexorable progression toward a rigidly stiff, painful joint that severely compromises the windlass mechanism, altering the patient's entire gait mechanics and frequently leading to secondary pathologies such as transfer metatarsalgia.
Detailed Surgical Anatomy and Biomechanics
A masterful surgical intervention for hallux rigidus demands an intimate, three-dimensional understanding of the first MTP joint's osteology, ligamentous restraints, and neurovascular topography. The first MTP joint functions primarily as a ginglymoidal (hinge) joint, though its shallow articular congruency permits slight degrees of abduction, adduction, and rotation. The articulation consists of the convex, cam-shaped head of the first metatarsal and the concave elliptical base of the proximal phalanx. The plantar aspect of the metatarsal head is defined by the crista, a central bony ridge that separates two longitudinally oriented grooves. These grooves serve as the articulation pathways for the medial (tibial) and lateral (fibular) sesamoids.
The capsuloligamentous complex of the first MTP joint is robust and highly specialized. The plantar plate is a dense, fibrocartilaginous structure that originates from the metatarsal neck and inserts firmly into the plantar base of the proximal phalanx. It houses the sesamoids and acts as the primary static restraint against dorsal subluxation. The medial and lateral collateral ligaments, along with the metatarsosesamoid and phalangeosesamoid suspensory ligaments, provide critical varus-valgus stability. Furthermore, the deep transverse metatarsal ligament (DTML) tethers the first ray's plantar plate to that of the second ray, integrating the hallux into the dynamic stability of the forefoot arch.
The tendinous anatomy is equally critical. The Extensor Hallucis Longus (EHL) tendon courses centrally over the dorsal joint capsule, enclosed within its synovial sheath, inserting at the distal phalanx. Deep to the EHL lies the Extensor Hallucis Brevis (EHB), inserting on the proximal phalanx. Plantarly, the Flexor Hallucis Brevis (FHB) muscle bifurcates, with its medial and lateral heads enveloping the respective sesamoids before inserting into the plantar base of the proximal phalanx. The Flexor Hallucis Longus (FHL) tendon glides smoothly between the sesamoids, deep to the plantar plate, acting as a powerful plantarflexor of the interphalangeal joint and a secondary stabilizer of the MTP joint during the push-off phase of gait.
From a surgical risk perspective, the neurovascular anatomy dictates our approach. The most critical structure at risk during a dorsal approach is the dorsomedial cutaneous nerve, the terminal medial branch of the superficial peroneal nerve. Cadaveric studies demonstrate that this nerve can lie as close as 6 millimeters medial to the EHL tendon at the level of the MTP joint. Iatrogenic transection or traction injury to this nerve results in devastating, recalcitrant neuromas or chronic regional pain syndromes. The dorsal digital nerves and dorsal metatarsal arteries also traverse the operative field and require meticulous blunt dissection and retraction to preserve the delicate soft-tissue envelope of the hallux.
Exhaustive Indications and Contraindications
The decision to proceed with a dorsal cheilectomy, plantar release, and microfracture is predicated on a meticulous correlation of the patient's subjective symptoms, physical examination findings, and radiographic grading. We rely heavily on the Coughlin and Shurnas classification system to guide surgical decision-making. This procedure is the gold standard for patients with Grade 1 and Grade 2 hallux rigidus who have failed exhaustive conservative management, including rigid Morton's extensions, carbon fiber insoles, intra-articular corticosteroid injections, and NSAID therapy.
In select cases, early Grade 3 hallux rigidus—characterized by more significant joint space narrowing but preservation of the plantar cartilage—can be managed with this joint-sparing approach. However, the surgeon must have a frank, documented discussion with the patient regarding the lower success rates and the potential need for future arthrodesis. The primary goal of cheilectomy is to excise the dorsal mechanical block, thereby decompressing the joint and restoring functional, pain-free dorsiflexion. The addition of a plantar release addresses soft-tissue contractures, while microfracture targets focal, full-thickness osteochondral lesions discovered intraoperatively on the metatarsal head.
Contraindications must be strictly observed to prevent catastrophic clinical failures. Absolute contraindications include Coughlin and Shurnas Grade 4 disease, characterized by complete obliteration of the joint space, severe stiffness (ankylosis), and pain throughout the entire arc of motion, including the mid-arc. In these scenarios, joint-sparing procedures will predictably fail, and the patient is best served by a first MTP arthrodesis or, in highly selected older, low-demand patients, an interpositional or excisional arthroplasty.
Furthermore, severe degenerative changes isolated to the sesamoid-metatarsal articulation represent a relative contraindication to isolated dorsal cheilectomy. If the primary pain generator is plantar and related to the sesamoids, a dorsal decompression will not alleviate the patient's symptoms. Inflammatory arthropathies (e.g., rheumatoid arthritis, severe gouty arthropathy with extensive tophi) also contraindicate joint preservation, as the systemic disease process will rapidly destroy any remaining cartilage. Active soft tissue infection or severe peripheral vascular disease precluding wound healing are absolute contraindications for any elective foot surgery.
Indications and Contraindications Summary
| Category | Specific Criteria / Conditions | Rationale / Clinical Note |
|---|---|---|
| Primary Indications | Coughlin & Shurnas Grade 1 & 2 | Dorsal impingement is the primary pain generator; cartilage is largely preserved. |
| Marginal Indications | Early Coughlin & Shurnas Grade 3 | Requires careful patient selection; plantar cartilage must be viable. Moderate risk of progression. |
| Adjunct Indications | Focal Osteochondral Lesions (OCDs) | Indication for concurrent microfracture to stimulate fibrocartilage repair. |
| Absolute Contraindications | Coughlin & Shurnas Grade 4 (Ankylosis) | Complete cartilage loss; cheilectomy will result in persistent, severe mid-arc pain. |
| Absolute Contraindications | Inflammatory Arthropathy (e.g., RA) | Systemic synovial destruction dictates arthrodesis or arthroplasty. |
| Relative Contraindications | Severe Sesamoid-Metatarsal Arthritis | Dorsal decompression does not address plantar pain generators. |

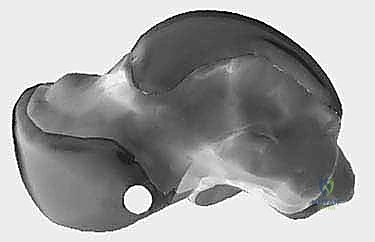

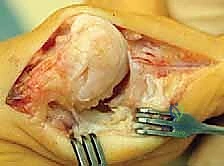
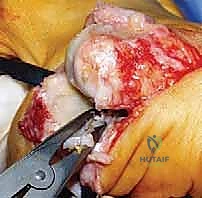
(Note: Massive, uncontained osteochondral defects may occasionally require advanced techniques such as osteochondral autograft transplantation, as illustrated above, rather than simple microfracture.)
Pre-Operative Planning, Templating, and Patient Positioning
Surgical success is architected in the pre-operative planning phase. A comprehensive clinical evaluation begins with a detailed history, focusing on the character of the pain (impingement vs. mid-arc), previous trauma, and occupational demands. The physical examination must meticulously isolate the first MTP joint. The surgeon assesses the exact arc of motion, noting the point at which pain is elicited. A positive "grind test" (axial compression with circumduction) indicating mid-arc pain suggests advanced global arthritis, potentially steering the plan away from cheilectomy. Palpation of the sesamoids during passive hallux dorsiflexion is crucial to rule out primary sesamoiditis or sesamoid arthrosis.
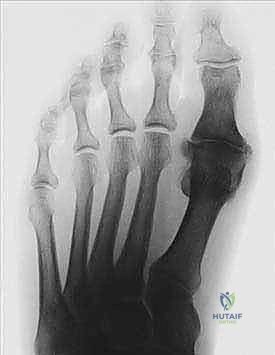
Standard weight-bearing imaging is mandatory. We require anteroposterior (AP), lateral, and oblique views of the foot. The AP view evaluates joint space narrowing, subchondral sclerosis, and the presence of medial or lateral osteophytes. The lateral view is paramount for assessing the size and morphology of the dorsal osteophyte and the degree of dorsal joint space preservation. If sesamoid pathology is suspected clinically, a dedicated axial sesamoid view is obtained to evaluate the crista and the sesamoid-metatarsal articulation.

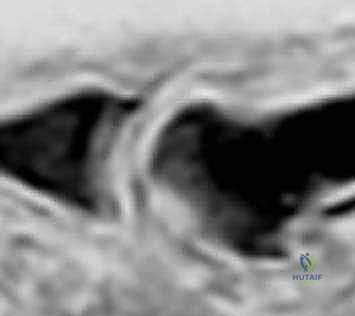
While plain radiography is usually sufficient, Magnetic Resonance Imaging (MRI) is an invaluable adjunct when the clinical pain is disproportionate to radiographic findings. MRI provides high-resolution, multi-planar evaluation of the articular cartilage, subchondral bone marrow edema (suggestive of impending structural failure), and the integrity of the plantar plate. Crucially for our masterclass procedure, MRI accurately sizes and localizes occult osteochondral lesions on the metatarsal head, allowing the surgeon to pre-emptively plan for a microfracture or marrow stimulation technique.
On the day of surgery, meticulous patient positioning optimizes surgical flow. The patient is placed supine on the operating table. It is critical to position the patient such that the foot extends slightly off the distal edge of the table; this allows the surgeon to freely manipulate the hallux through an unrestricted arc of plantarflexion and dorsiflexion during the procedure, which is essential for evaluating the adequacy of the resection and release. A small bump placed under the ipsilateral hip internally rotates the lower extremity, bringing the first ray into a perfectly neutral, upward-facing position. A well-padded thigh tourniquet is applied to ensure a pristine, bloodless surgical field, and regional anesthesia (such as a popliteal or ankle block) is typically administered in conjunction with monitored anesthesia care or general anesthesia.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach requires precision to maximize exposure while respecting the delicate dorsal soft-tissue envelope. We utilize a 5-centimeter dorsal longitudinal incision centered over the first MTP joint, placed just medial to the palpable border of the Extensor Hallucis Longus (EHL) tendon. Subcutaneous dissection is performed bluntly with dissecting scissors. This is the critical danger zone. The surgeon must meticulously identify and gently retract the dorsomedial cutaneous nerve, which frequently crosses the operative field from proximal-lateral to distal-medial. The EHL tendon is mobilized within its sheath and retracted laterally, exposing the dorsal joint capsule.
A longitudinal or inverted U-shaped capsulotomy is performed. The capsule is sharply elevated off the dorsal metatarsal neck and the base of the proximal phalanx, exposing the pathology. The hallmark dorsal osteophyte, often appearing as a prominent "lipping" of the metatarsal head, will be immediately visible. Hypertrophic synovium is aggressively debrided using a rongeur and a motorized shaver to fully visualize the articular surfaces.


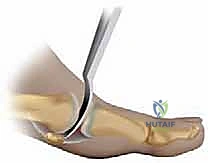
The cheilectomy is then executed. Using a microsagittal saw or a sharp, broad osteotome, the dorsal 20% to 30% of the metatarsal head is resected. The cut is initiated dorsally on the metatarsal neck, just proximal to the osteophyte, and directed distally and slightly plantarly to exit at the dorsal margin of the viable articular cartilage. It is imperative to avoid resecting more than 30% of the head, as this risks destabilizing the joint or compromising the insertion of the collateral ligaments. The dorsal base of the proximal phalanx is also inspected, and any corresponding osteophytes are excised. The resected corners are meticulously contoured and smoothed with a surgical rasp to prevent future soft-tissue irritation.

Following the bony resection, we proceed to the plantar release. Over time, hallux rigidus causes the plantar plate and sesamoid complex to become contracted and adherent to the plantar metatarsal head. Using a McGlamry elevator or a curved Freer elevator, the surgeon carefully sweeps plantarly between the metatarsal head and the plantar plate. This maneuver breaks up adhesions and mobilizes the sesamoids. The adequacy of the cheilectomy and plantar release is confirmed by passively dorsiflexing the hallux; we strive for a minimum of 70 to 80 degrees of impingement-free intraoperative dorsiflexion.
Finally, the articular surface is closely inspected for focal osteochondral defects. If a full-thickness chondral lesion is identified, a microfracture technique is employed. The base of the lesion is debrided of all unstable cartilage flaps down to the calcified cartilage layer using a curette, creating stable, vertical margins. A specialized arthroscopic awl or a 0.045-inch Kirschner wire is then used to create multiple perforations into the subchondral bone, spaced approximately 2 to 3 millimeters apart and 4 millimeters deep. The tourniquet is temporarily deflated to confirm the egress of marrow fat droplets and blood into the defect, ensuring adequate penetration to stimulate a fibrocartilaginous healing response. The capsule is then meticulously repaired with absorbable sutures, and the skin is closed.
Complications, Incidence Rates, and Salvage Management
While dorsal cheilectomy with microfracture is highly successful in appropriately selected patients, complications can and do occur. The most dreaded intraoperative complication is injury to the dorsomedial cutaneous nerve. Neuropraxia occurs in approximately 5-10% of cases due to traction, but frank transection results in a devastating neuroma. Management of a painful neuroma initially involves targeted steroid injections and desensitization therapy, but recalcitrant cases require surgical excision and implantation of the nerve stump deep into the intrinsic musculature.
Infection is a risk inherent to any open procedure, occurring in less than 2% of first MTP joint surgeries. Superficial infections are managed aggressively with oral antibiotics and local wound care. Deep space infections involving the joint capsule or bone are surgical emergencies requiring immediate formal irrigation, debridement, and culture-directed intravenous antibiotic therapy. Delayed wound healing is more common in diabetic patients or chronic smokers and demands meticulous postoperative monitoring.


The most common long-term complication is the recurrence of symptoms or the progressive advancement of osteoarthritis. Studies indicate that up to 10-15% of patients will eventually require a salvage procedure within 5 to 10 years. Progressive joint space narrowing, recurrent osteophyte formation, and the return of intractable pain indicate failure of the joint-sparing approach. In these scenarios, the definitive salvage procedure is a first MTP joint arthrodesis. Arthrodesis provides reliable, permanent pain relief at the cost of joint motion.


Iatrogenic hallux varus or valgus can occur if the capsular repair is imbalanced or if excessive bone is resected, destabilizing the collateral ligament origins. Transfer metatarsalgia to the lesser rays may develop if the first ray is inadvertently shortened or if the patient avoids loading the first MTP joint due to chronic pain.
Complications and Salvage Management Table
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| Dorsomedial Nerve Injury | 5% - 10% (Neuropraxia) | Meticulous blunt dissection; direct visualization and retraction. | Gabapentinoids; Steroid injection; Surgical neurectomy and muscle implantation. |
| Recurrent Hallux Rigidus / OA | 10% - 15% at 10 years | Strict adherence to surgical indications; adequate initial resection (30%). | First MTP Joint Arthrodesis (Gold Standard Salvage). |
| Superficial/Deep Infection | < 2% | Pre-op antibiotics; meticulous hemostasis; sterile technique. | Oral/IV antibiotics; Operative I&D for deep capsular involvement. |
| Iatrogenic Instability (Varus/Valgus) | < 1% | Avoid resecting >30% of MT head; anatomic capsular repair. | Soft tissue reconstruction; Arthrodesis if accompanied by severe arthritis. |
| Transfer Metatarsalgia | 2% - 5% | Preserve metatarsal length; encourage early weight-bearing on the first ray. | Orthotics with metatarsal pads; Weil osteotomies of lesser rays if recalcitrant. |
Phased Post-Operative Rehabilitation Protocols
The success of a cheilectomy and plantar release is heavily dependent on the patient's adherence to a rigorous, phased postoperative rehabilitation protocol. The primary goal in the early postoperative period is to maintain the extensive range of motion achieved in the operating room while allowing the soft tissue envelope to heal.
Phase 1: Tissue Healing and Early Motion (Weeks 0-2)
Immediately postoperatively, the patient is placed in a bulky, compressive soft dressing and provided with a rigid-soled postoperative shoe. Weight-bearing is permitted as tolerated, but patients are strictly instructed to heel-weight-bear to minimize stress on the dorsal incision and the healing capsule. Elevation and cryotherapy are critical during the first 72 hours to control edema. At the two-week mark, the patient returns to the clinic for suture removal. Once the wound is confirmed to be sealed, the most critical aspect of rehab begins: aggressive, daily passive range of motion (PROM) exercises. The patient is taught to manually grasp the hallux and push it into maximum dorsiflexion and plantarflexion multiple times a day.
Phase 2: Restoring Mechanics and Active Motion (Weeks 2-6)
During this phase, the patient transitions from the rigid postoperative shoe to a wide-toebox, stiff-soled athletic shoe. Active range of motion (AROM) exercises are initiated. Physical therapy is highly recommended to assist with joint mobilization, scar tissue massage, and gait retraining. The focus shifts to restoring the windlass mechanism. Patients are encouraged to perform toe crunches, marble pickups, and towel curls to strengthen the intrinsic foot musculature and the flexor hallucis longus. If a microfracture was performed, high-impact activities are strictly avoided to allow the fibrocartilage clot to mature, though normal walking is encouraged.

Phase 3: Return to Unrestricted Activity (Weeks 6 and Beyond)
By the sixth week, patients typically exhibit significant reductions in swelling and pain. They are cleared to gradually resume normal activities, including low-impact cardiovascular
