Hemi-Epiphysiodesis for Ankle Valgus: A Masterclass in Guided Growth Modulation

Key Takeaway
This masterclass details hemi-epiphysiodesis for ankle valgus, covering crucial surgical anatomy, patient positioning, and step-by-step intraoperative execution. Learn precise techniques for medial malleolar screws and eight-plates, emphasizing fluoroscopic guidance and periosteal preservation. Gain insights into managing complications, ensuring optimal growth modulation, and effective postoperative rehabilitation for pediatric patients.
Comprehensive Introduction and Patho-Epidemiology
Ankle valgus in the growing child presents a fascinating, yet structurally devastating, pediatric deformity that extends far beyond a simple cosmetic concern. This condition represents a progressive biomechanical failure of the tibiotalar articulation that, if left unaddressed, inexorably leads to significant pain, functional limitation, gait aberrations, and ultimately, debilitating early-onset osteoarthritis. Our objective in this masterclass chapter is to meticulously deconstruct the principles of guided growth modulation and detail the execution of medial hemi-epiphysiodesis to correct this alignment during the critical windows of skeletal immaturity.
The pathogenesis of ankle valgus is deeply rooted in a fundamental anatomical discrepancy: a relatively foreshortened fibula. In a physiologically normal ankle, the distal fibula acts as an indispensable lateral buttress. It extends distally beyond the tibial plafond, effectively capturing the talus within the mortise and preventing lateral talar tilt or translation during the dynamic loads of the gait cycle. When the fibula is pathologically short—whether due to congenital dysplasia, neuromuscular imbalance, or prior trauma—this critical buttressing effect is lost. The talus is consequently permitted to subluxate laterally and tilt into a valgus orientation, shifting the mechanical axis of the lower extremity.
Biomechanically, in the anteroposterior (AP) plane, this lateral talar shift causes the weight-bearing axis and the ground reaction force (GRF) to migrate laterally, falling outside the virtual center of the tibiotalar joint. This eccentric loading initiates a destructive and self-perpetuating cycle dictated by the Hueter-Volkmann law. As the fibular epiphysis bears a disproportionate load—far exceeding its customary 15% of body weight—the increased compression paradoxically stimulates broadening of the epiphysis due to hindfoot impingement, while simultaneously inhibiting its longitudinal growth.
Conversely, the lateral displacement of the GRF means the compressive forces on the lateral aspect of the distal tibial physis exceed physiological tolerance. This unremitting mechanical stress suppresses chondrocyte proliferation and hypertrophy in the lateral physis, causing the lateral side to grow at a significantly slower rate than the medial side. The medial physis, experiencing relative tension, continues to grow, resulting in progressive wedging of the distal tibial epiphysis. This wedging further exacerbates the plafond tilt, perpetuating the valgus deformity in a classic positive feedback loop.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and the intricate biomechanics of the pediatric ankle is the absolute prerequisite for successful growth modulation. We must approach the distal tibia and fibula not merely as static bones, but as a dynamic, growing organ system subject to complex mechanical forces.
In a healthy, neutrally aligned ankle, the distal articular surface of the tibia (the plafond) is perfectly horizontal in the coronal plane. Radiographically, this is quantified by a lateral distal tibial angle (LDTA) of approximately 87 to 90 degrees, indicating a neutral to very slight valgus alignment (0 to 3 degrees). The fibula is typically longer than the tibia distally, with its physis normally resting at or just distal to the level of the tibial plafond. The talus is securely sandwiched between the medial and lateral malleoli, stabilized by robust ligamentous structures: the deltoid ligament complex medially, and the talofibular and calcaneofibular ligaments laterally. The physes of both the tibia and fibula lie horizontally, perpendicular to the ground reaction forces, optimizing balanced longitudinal growth.

With the onset and progression of ankle valgus, we observe highly specific pathological changes in the regional anatomy. The plafond tilts laterally, losing its horizontal orientation. Radiographically, we frequently observe widening of the medial clear space. This widening is a critical sign, indicative of chronic attenuation and plastic deformation of the deltoid ligament complex due to unrelenting medial tension. Subject to this chronic traction, the medial malleolus may exhibit delayed, fragmented, or irregular ossification. Furthermore, the lateral tilt of the talus introduces pathological shear forces across the articular cartilage, leading to early attrition and degeneration, typically commencing at the lateral corner of the plafond.

Surgically, the medial approach to the distal tibia requires meticulous navigation of the local neurovascular topography. The primary structures of concern are the saphenous nerve and the great saphenous vein. These structures reliably course anterior to our standard incision lines for both transmalleolar screw and tension-band plate techniques. The surgical approach is predominantly subcutaneous, demanding careful preservation of the periosteal sleeve. Disruption of the periosteum, particularly over the physis, can incite the formation of an unintended physeal bar, transforming a reversible growth modulation into a permanent growth arrest. There are no major muscular intervals to dissect through directly on the medial aspect of the distal tibia, making the approach straightforward but unforgiving of careless soft tissue handling.
Exhaustive Indications and Contraindications
The decision to intervene surgically via hemi-epiphysiodesis hinges on a delicate calculus involving the magnitude of the deformity, the patient's symptomatology, and, most critically, the amount of remaining skeletal growth. The natural history of structural ankle valgus is insidious; it does not spontaneously resolve and typically accelerates during the adolescent growth spurt.
Parents routinely report chronic, progressively severe flatfoot deformities accompanied by asymmetric, rapid shoewear. The child often complains of activity-related pain, typically localized laterally beneath the fibula due to subfibular impingement of the calcaneus or talus. Medial pain is also common, manifesting as a deep ache secondary to chronic tension on the attenuated deltoid ligament. Crucially, conservative measures such as corrective shoes, orthotics, or bracing have absolutely no beneficial effect on the natural history of the skeletal deformity. While a University of California Biomechanics Laboratory (UCBL) insert might provide transient symptomatic relief by supporting the arch, it will not induce any skeletal remodeling or halt the progression of the valgus tilt.
Surgical intervention is indicated when there is progressive deformity documented on serial weight-bearing radiographs, accompanied by evolving, activity-restricting pain. The ideal candidate has at least 12 to 24 months of remaining longitudinal growth, allowing sufficient time for the tethered medial physis to act as a hinge while the lateral physis "catches up."
| Parameter | Indications for Hemi-Epiphysiodesis | Contraindications for Hemi-Epiphysiodesis |
|---|---|---|
| Growth Potential | Open physes with > 1-2 years of growth remaining. | Skeletally mature (closed physes) or < 6 months growth. |
| Deformity Magnitude | Mild to moderate valgus (LDTA < 80-85 degrees). | Severe, rigid deformity requiring acute osteotomy. |
| Physeal Health | Healthy, functioning lateral distal tibial physis. | Existing lateral physeal bar or global physeal arrest. |
| Symptomatology | Progressive pain, gait disturbance, subfibular impingement. | Asymptomatic, non-progressive physiological valgus. |
| Associated Conditions | Neuromuscular (CP, Spina Bifida), skeletal dysplasias. | Active local infection, uncorrectable rigid hindfoot coalition. |


Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is the crucible in which surgical success is forged. The foundation of this planning relies on high-quality, standardized imaging. We mandate weight-bearing anteroposterior (AP) and lateral radiographs of the ankles, as well as weight-bearing views of the feet to meticulously assess subtalar alignment. Subtalar valgus or instability can masquerade as, or severely exacerbate, an ankle valgus deformity. Furthermore, full-length weight-bearing AP radiographs of the lower extremities are imperative if there is any clinical suspicion of concomitant genu valgum, as a malaligned mechanical axis originating from the knee will impose eccentric loads on the ankle, compromising our local correction.
Templating requires a precise calculation of the patient's remaining growth potential. We utilize established methodologies, such as the Multiplier Method or the Greulich and Pyle atlas for bone age, to estimate the timing and duration of the intervention. The surgeon must decide between the two primary modalities of guided growth: the transmalleolar cannulated screw or the tension-band plate (e.g., eight-Plate). The tension-band plate is increasingly favored due to its lower risk of permanent physeal damage and its function as a flexible hinge rather than a rigid tether.


In the operating theater, precise patient positioning and fluoroscopic setup are non-negotiable. The patient is positioned supine on a radiolucent operating table. A small bump may be placed under the ipsilateral hip to internally rotate the leg, bringing the medial malleolus into a true AP profile. The C-arm fluoroscope must be draped and positioned to allow seamless, unimpeded transitions between AP, mortise, and lateral projections without compromising the sterile field.
A thigh or calf tourniquet is highly recommended to ensure a bloodless field, which is particularly critical for identifying and protecting the saphenous neurovascular bundle during the initial dissection. Before skin preparation, the surgeon should palpate and mark the medial malleolus, the joint line, and the anticipated level of the physis, confirming these landmarks with a preliminary fluoroscopic image.

Step-by-Step Surgical Approach and Fixation Technique
The execution of medial hemi-epiphysiodesis demands meticulous soft-tissue handling and precise radiographic targeting. We will detail both the tension-band plate technique and the transmalleolar screw technique, as both remain valuable tools in the orthopedic surgeon's armamentarium.
The Tension-Band Plate (Eight-Plate) Technique
The tension-band plate technique utilizes a non-locking, figure-of-eight plate that acts as a flexible hinge, allowing the screws to diverge as the lateral physis grows. A 1.5 to 2.0 cm longitudinal incision is made directly over the medial aspect of the distal tibial physis. Blunt dissection is employed to identify and retract the saphenous vein and nerve anteriorly.
It is absolutely critical to split the deep fascia longitudinally and expose the periosteum without stripping it. We operate strictly extra-periosteally. A Keith needle or a smooth K-wire is inserted into the medial physis under direct fluoroscopic guidance in both the AP and lateral planes to serve as the central reference point. The eight-plate is then threaded over this central reference wire, ensuring the plate sits flush against the metaphyseal and epiphyseal bone contours.


Once the plate is perfectly centered—straddling the physis equally—guide pins are inserted through the proximal (metaphyseal) and distal (epiphyseal) holes of the plate. Fluoroscopy must confirm that these pins are parallel to the joint line in the AP plane and centrally located in the lateral plane, strictly avoiding penetration into the joint space or the physis itself. Cannulated drills are used to prepare the tracts, and self-tapping, cannulated screws (typically 4.5mm) are inserted. The screws do not need to be fully seated to the plate initially; they are designed to toggle and diverge as growth occurs.


The Transmalleolar Screw Technique
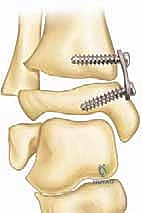
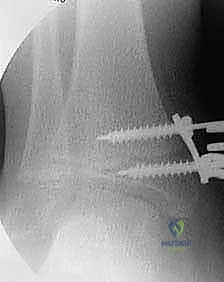
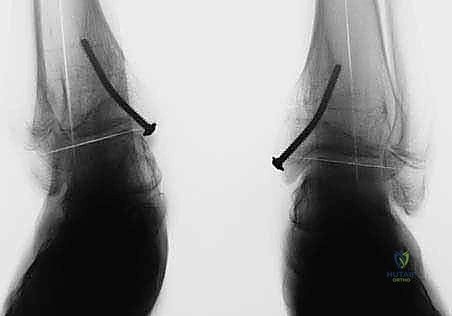
The transmalleolar screw technique involves placing a single, fully threaded cannulated screw across the medial physis to act as a rigid tether. A 5-mm transverse stab incision is made just distal to the tip of the medial malleolus. A guide pin is introduced and driven proximally and laterally, aiming to cross the medial physis at an angle of approximately 45 degrees to the longitudinal axis of the tibia.


Fluoroscopic verification in multiple planes is paramount. The pin must traverse the medial portion of the physis, engaging the metaphysis securely, while remaining entirely within the osseous corridor. It must not violate the articular surface of the medial malleolus or the tibiotalar joint. Once the trajectory is confirmed, the cortex is over-drilled, and a fully threaded cannulated screw (typically 4.5mm or 6.5mm depending on patient size) is advanced over the wire. The threads must fully cross the physis to ensure adequate compression and growth arrest on the medial side. The screw head is buried deep to the deltoid ligament to prevent soft tissue irritation.
Complications, Incidence Rates, and Salvage Management
While guided growth is generally a low-morbidity procedure, it is not devoid of complications. The most significant and common complication is overcorrection into ankle varus. This is not a failure of the implant, but rather a failure of postoperative surveillance. Because the intervention relies on the patient's intrinsic growth, the rate of correction is variable. If the hardware is left in place too long, the once valgus ankle will inexorably drift into a pathological varus alignment. This necessitates rigorous radiographic follow-up every 3 to 4 months. If overcorrection occurs, immediate hardware removal is mandated, and in severe cases, a reverse guided growth procedure (lateral hemi-epiphysiodesis) may be required.
Hardware failure is another distinct possibility, particularly in heavy patients or those with severe neuromuscular spasticity. For the transmalleolar screw, the immense shear forces across the physis can lead to screw bending or outright breakage. If a screw breaks within the physis, it can inadvertently cause a permanent physeal bar. For the tension-band plate, screw pullout or plate migration can occur if the screws are not adequately engaged in the epiphyseal and metaphyseal bone.
Permanent physeal arrest is the most devastating local complication. This typically arises from iatrogenic injury during the surgical approach—specifically, aggressive periosteal stripping over the perichondrial ring of LaCroix—or from placing the epiphyseal screw of a tension-band plate directly across the physis. If a permanent medial physeal bar forms before the lateral side has fully corrected, the patient will require a formal bar excision or, more likely, a definitive supramalleolar osteotomy at skeletal maturity.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Overcorrection (Varus) | 5 - 15% | Prevention: Strict clinical/radiographic follow-up every 3-4 months. Management: Prompt hardware removal. If severe, lateral hemi-epiphysiodesis. |
| Hardware Failure (Breakage/Pullout) | 2 - 5% | Prevention: Use appropriately sized implants; prefer plates over screws in heavy/spastic patients. Management: Revision fixation; removal of broken hardware if accessible without physeal damage. |
| Permanent Physeal Arrest | < 1% | Prevention: Extra-periosteal dissection; precise fluoroscopic screw placement avoiding the physis. Management: Physeal bar excision (if < 50% area) or corrective supramalleolar osteotomy at maturity. |
| Rebound Deformity | 10 - 20% | Prevention: Slightly overcorrect (1-2 degrees varus) before removal in younger children. Management: Re-implantation of guided growth hardware if significant growth remains. |
| Infection / Wound Dehiscence | 1 - 2% | Prevention: Meticulous hemostasis, prophylactic antibiotics, careful closure. Management: Oral/IV antibiotics; surgical debridement and hardware removal if deep infection occurs. |




Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a medial hemi-epiphysiodesis is remarkably accelerated compared to traditional osteotomies, highlighting one of the primary advantages of guided growth. Because we have not compromised the structural integrity of the long bone, prolonged immobilization is neither necessary nor desirable.
In the immediate postoperative phase (Days 0-14), the patient is typically placed in a soft, bulky dressing or a removable walking boot for comfort and soft tissue protection. Weight-bearing as tolerated (WBAT) with crutches or a walker is permitted immediately. The primary goals during this phase are pain control, reduction of edema, and the initiation of gentle, active range-of-motion (ROM) exercises for the ankle and subtalar joints to prevent stiffness.
By weeks 2 to 4, assuming the surgical incisions have healed impeccably, the patient is transitioned out of the boot and encouraged to resume normal ambulation in supportive athletic shoes. Formal physical therapy may be instituted if the patient demonstrates persistent gait deviations, muscle weakness (particularly in the gastrocnemius-soleus complex or peroneal musculature), or restricted dorsiflexion. Therapy focuses on proprioceptive training, aggressive Achilles stretching, and progressive strengthening.
The most critical phase of postoperative management is the radiographic surveillance. The patient must return for clinical examination and weight-bearing AP and lateral radiographs of the ankle every 3 to 4 months. The surgeon meticulously measures the lateral distal tibial angle (LDTA) on each visit. Once neutral alignment (an LDTA of approximately 88-90 degrees) is achieved, the hardware must be surgically removed to prevent overcorrection into varus. In younger children with substantial growth remaining, a deliberate, slight overcorrection (1 to 2 degrees of varus) may be targeted prior to hardware removal to anticipate and mitigate the known phenomenon of rebound valgus growth.

Summary of Landmark Literature and Clinical Guidelines
The evolution of guided growth for angular deformities is a testament to the continuous refinement of pediatric orthopedic principles. Historically, the management of ankle valgus relied heavily on the Phemister technique of permanent bone block epiphysiodesis or the Blount staple technique. While Blount staples introduced the concept of reversibility, their rigid nature frequently led to staple migration, backing out, or asymmetrical compression, leading to unpredictable results.
The paradigm shifted dramatically with the introduction of the tension-band plate concept by Peter Stevens in the early 2000s. The eight-plate technique revolutionized the field by utilizing a non-locking plate with a central pivot point, allowing the epiphyseal and metaphyseal screws to diverge as the contralateral physis continued to grow. This flexible hinge construct significantly reduced the incidence of hardware failure and permanent physeal arrest compared to rigid staples or transmalleolar screws. Contemporary literature strongly supports the use of tension-band plates as the gold standard for guided growth at the distal tibia.
Clinical guidelines emphasize that the etiology of the valgus deformity significantly influences the rate of correction and the risk of rebound. Patients with idiopathic or constitutional valgus tend to correct predictably and maintain alignment post-removal. Conversely, syndromic patients—particularly those with neuromuscular disorders like Cerebral Palsy or skeletal dysplasias like Multiple Hereditary Exostoses—exhibit a slower rate of correction, a higher incidence of hardware failure, and a profound propensity for rebound deformity once the hardware is removed. In these complex populations, surgeons must maintain heightened vigilance, utilize more robust fixation if necessary, and counsel families extensively regarding the likelihood of requiring multiple interventions throughout the child's growing years.
