Hemiarthroplasty, Total Shoulder Arthroplasty, and Biologic Glenoid Resurfacing for Glenohumeral Arthritis With an Intact Rotator Cuff
Comprehensive Introduction and Patho-Epidemiology
Glenohumeral arthritis encompasses a remarkably heterogeneous group of degenerative, inflammatory, and post-traumatic conditions characterized by the progressive, irreversible loss of articular cartilage, varying degrees of soft tissue contracture, insidious rotator cuff dysfunction, and profound subchondral bone erosion. The successful surgical management of this debilitating condition hinges fundamentally on the structural integrity and functional capacity of the rotator cuff musculature. Therefore, glenohumeral arthritides are classically subdivided in orthopedic literature based on rotator cuff status. This chapter focuses exclusively on the subset of patients presenting with glenohumeral arthritis and a functionally intact or readily reparable rotator cuff. Common etiologies within this specific category include primary osteoarthritis, post-traumatic arthritis, avascular necrosis (osteonecrosis), and specific, well-controlled subsets of inflammatory arthropathy. Understanding the nuanced differences between these etiologies is paramount for preoperative planning, implant selection, and optimizing long-term survivorship of the arthroplasty.
The biologic basis for primary glenohumeral arthritis, while multifactorial, represents a profound and sustained imbalance in the normal homeostatic cycle of cartilage degradation and repair. Mechanical factors, such as congenital glenoid hypoplasia and increased native retroversion, may predispose the joint to accelerated, asymmetric wear, though in a vast majority of idiopathic cases, no distinct pre-existing anatomic anomaly is evident. The final common biochemical pathway involves the upregulated, uncontrolled release of degradative enzymes—specifically matrix metalloproteinases including collagenase, gelatinase, and stromelysin—alongside a cascade of potent inflammatory mediators such as interleukins (IL-1, IL-6) and tumor necrosis factor-alpha (TNF-α). This hostile intra-articular environment overwhelms tissue inhibitors of metalloproteinases (TIMPs), perpetuating rapid chondrocyte apoptosis, progressive cartilage delamination, and the eventual eburnation of the underlying subchondral bone, which manifests radiographically as dense sclerosis and subchondral cyst formation.
In cases of post-traumatic arthritis, catastrophic cartilage damage associated with a single high-energy event (such as a severe fracture-dislocation) or repetitive microtrauma overwhelms the intrinsic, albeit limited, repair mechanisms of the shoulder joint. The natural history of glenohumeral arthritis, regardless of the precipitating etiology, is characterized by progressive stiffness, intractable pain that frequently awakens the patient at night, and profound functional impairment in activities of daily living. Patients with primary osteoarthritis and post-traumatic variants typically develop a progressive, highly characteristic loss of external rotation. This restriction is primarily driven by the severe contracture of the anterior capsule and the coracohumeral ligament. This asymmetric capsular contracture obligates posterior translation of the humeral head during active motion, leading to eccentric posterior glenoid wear, posterior subluxation, and the formation of large, characteristic osteophytes, particularly along the inferior humeral neck (the so-called "goat's beard" osteophyte). Notably, full-thickness rotator cuff tears are distinctly uncommon in primary osteoarthritis, occurring in only 5% to 10% of patients, which fundamentally dictates the surgical algorithm toward anatomic rather than reverse reconstruction.
Conversely, rheumatoid arthritis and other systemic inflammatory arthritides are characterized by a systemic activation of the immune system that drives an influx of lymphocytes and macrophages into the synovial tissue. This results in a hyperplastic, highly vascularized, and invasive pannus that releases destructive cytokines, leading to profound regional osteopenia, central (concentric) glenoid bone erosion, and a significantly higher incidence of concomitant rotator cuff pathology. The prevalence of full-thickness rotator cuff tears in rheumatoid shoulders ranges from 25% to 40%, and substantial partial tearing or intrinsic tendinopathy is nearly ubiquitous due to the chronic inflammatory milieu. When addressing inflammatory arthritis within the context of this chapter, it strictly pertains to the carefully selected, medically optimized subset of patients in whom the rotator cuff remains intact or is readily reparable, allowing for concentric joint kinematics and stability post-reconstruction.

Detailed Surgical Anatomy and Biomechanics
Osseous Anatomy and Proximal Humeral Geometry
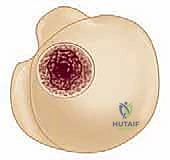
The precise, anatomic restoration of normal osseous relationships is the paramount objective in anatomic shoulder arthroplasty. The proximal humerus exhibits highly variable geometry that correlates broadly with patient size, gender, and ethnicity, yet it maintains several remarkably constant proportional relationships that are foundational to modern prosthetic design. The mean humeral head radius of curvature is approximately 24 mm, with a physiological range spanning from 19 to 28 mm. The mean humeral head thickness is about 19 mm, ranging from 15 to 24 mm. Crucially, the ratio of humeral head thickness to the humeral head radius of curvature remains remarkably constant at approximately 0.7 to 0.9, regardless of patient height or humeral shaft diameter. This proportional constancy is a critical principle in intraoperative templating, ensuring that the selected implant restores the native volume of the resected articular segment without overstuffing the joint, which would otherwise lead to stiffness and accelerated glenoid wear.
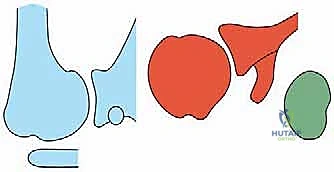
The center of the humeral head does not coincide with the projected central axis of the humeral shaft. This spatial discrepancy, defined biomechanically as the humeral head offset, averages 7 to 9 mm in the medial direction and 2 to 4 mm in the posterior direction relative to the central intramedullary canal. Failure to anatomically restore this offset during arthroplasty fundamentally alters the resting length and moment arms of the rotator cuff musculature. Such biomechanical alterations lead to eccentric glenoid loading, accelerated polyethylene wear, obligate translation during active elevation, and suboptimal functional outcomes. Furthermore, the humeral neck-shaft angle—defined as the angle subtended by the central intramedullary axis and the base of the articular segment—shows substantial individual variation. The average neck-shaft angle is 130 to 135 degrees, but it exhibits a wide clinical range from 120 to 145 degrees, necessitating modular or variable-angle prosthetic systems to accurately replicate native anatomy.
Humeral retroversion is another highly variable anatomic parameter, averaging 20 to 30 degrees relative to the transepicondylar axis of the distal humerus, but exhibiting a wide population range of 20 to 55 degrees. Accurately reproducing the patient's native retroversion is essential for maintaining anterior-posterior stability and optimizing the tension of the subscapularis repair. The vertical distance between the highest point of the humeral articular surface and the highest point of the greater tuberosity is approximately 8 mm. This head-to-tuberosity height demonstrates relatively small inter-specimen variability and serves as a critical, easily identifiable intraoperative landmark. Restoring this 8 mm differential prevents subacromial impingement (if the prosthetic head is placed too low) or excessive rotator cuff tension and potential secondary cuff failure (if the head is placed too high).

Soft Tissue Constraints and Neurovascular Structures
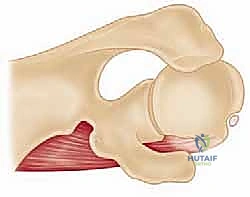
The ligamentous and musculotendinous structures surrounding the glenohumeral joint dictate its dynamic stability, obligate kinematics, and safe surgical exposure. The pertinent musculotendinous anatomy includes the deltoid, pectoralis major, the conjoined tendon (coracobrachialis and short head of the biceps), the rotator cuff, and the long head of the biceps. In the arthritic shoulder with an intact cuff, the anterior and inferior capsular ligaments—particularly the middle glenohumeral ligament (MGHL) and the anterior band of the inferior glenohumeral ligament (AB-IGHL)—become profoundly contracted and fibrotic. This anterior tethering not only restricts external rotation but acts as a pathologic fulcrum, driving the humeral head posteriorly during active elevation and directly exacerbating the asymmetric posterior glenoid wear commonly seen in Walch B-type glenoids.
Neurovascular structures in the vicinity of the shoulder are abundant, complex, and highly vulnerable during the standard surgical exposure and retractor placement required for arthroplasty. The axillary artery and its branches—especially the anterior humeral circumflex, posterior humeral circumflex, and subscapular arteries—must be meticulously protected. The anterior humeral circumflex artery, along with its accompanying veins (the "three sisters"), is a key landmark at the inferior border of the subscapularis and is routinely ligated to minimize intraoperative hemorrhage. The entire brachial plexus traverses the anterior aspect of the shoulder, making it susceptible to traction neuropraxias resulting from overzealous arm positioning (excessive extension and external rotation) or aggressive medial retractor placement.

The two most pertinent nerves at risk during the standard deltopectoral approach are the axillary nerve and the musculocutaneous nerve. The axillary nerve, a terminal branch of the posterior cord composed primarily of motor fibers from the C5 and C6 roots, descends along the anterior surface of the subscapularis muscle. It courses inferior to the joint capsule, passing through the quadrilateral space to innervate the teres minor and deltoid. It is particularly at risk during the inferior capsular release and must be actively palpated and protected with a blunt retractor. The musculocutaneous nerve, a terminal branch of the lateral cord, lies anterior and lateral to the axillary nerve. It typically pierces the conjoined tendon approximately 5 cm distal to the tip of the coracoid process; however, this course is highly variable, and its entry point can be as proximal as 2 cm. Vigorous medial retraction of the conjoined tendon can cause a neuropraxia of this nerve, leading to devastating postoperative deficits in elbow flexion.
Exhaustive Indications and Contraindications
The decision algorithm for selecting between hemiarthroplasty, total shoulder arthroplasty (TSA), and hemiarthroplasty with biologic glenoid resurfacing remains one of the most vigorously debated topics in contemporary orthopedic surgery. The relative indications must be meticulously individualized according to patient age, functional demands, physiologic bone stock, and the specific morphology of the glenoid deformity. Concentricity of the joint without fixed posterior or superior subluxation drastically improves prosthetic performance and longevity in all circumstances. Therefore, correcting fixed posterior subluxation, restoring native version, and achieving balanced soft-tissue tension are paramount objectives, regardless of the chosen implant modality.
Total shoulder arthroplasty is universally considered the gold standard for older patients (typically >65 years) with end-stage osteoarthritis, an intact rotator cuff, and sufficient glenoid bone stock to support a rigidly fixed polyethylene component. TSA consistently provides superior, more predictable pain relief, improved range of motion, and enhanced functional restoration compared to hemiarthroplasty alone. However, the recognized "Achilles heel" of TSA is the ultra-high-molecular-weight polyethylene (UHMWPE) glenoid component, which is subject to aseptic loosening, edge-loading wear, and eventual failure over time. This risk is exponentially magnified in young, highly active patients or heavy manual laborers who subject the joint to massive shear and compressive forces that exceed the fatigue strength of the cement-bone interface.
For patients deemed too young or too active for a traditional polyethylene glenoid (typically <55 years of age), hemiarthroplasty alone or hemiarthroplasty combined with biologic glenoid resurfacing may be strongly indicated. Hemiarthroplasty relies on the native glenoid cartilage (or eburnated subchondral bone) to articulate with the metallic or ceramic prosthetic humeral head. While it entirely eliminates the risk of catastrophic glenoid component loosening, it frequently results in progressive glenoid erosion, persistent deep aching pain, and the eventual need for revision to a TSA. To mitigate this, biologic resurfacing techniques utilize interpositional grafts—such as lateral meniscal allograft, capsular or fascia lata autograft/allograft, acellular dermal allograft, or Achilles tendon allograft—to provide a biologic, friction-reducing cushion over the reamed glenoid surface. While theoretically appealing and successful in short-term cohorts, the long-term durability and definitive superiority of biologic resurfacing over simple concentric hemiarthroplasty (the "ream and run" procedure) have yet to be unequivocally confirmed in high-level, multicenter prospective trials.

Indications and Contraindications Matrix
| Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Total Shoulder Arthroplasty (TSA) | End-stage OA/RA with intact cuff; Age >65; Concentric glenoid or correctable eccentric wear. | Active infection; Neuropathic joint (Charcot); Absent/irreparable rotator cuff; Deltoid paralysis. | Age <50 (due to high risk of glenoid loosening); Heavy laborers; Severe uncorrectable glenoid bone loss. |
| Hemiarthroplasty | AVN with pristine glenoid cartilage; Young/active patients (<50) with OA; Severe uncorrectable glenoid bone loss. | Active infection; Neuropathic joint. | Inflammatory arthritis (high risk of rapid glenoid medialization); Pre-existing severe concentric glenoid wear. |
| Biologic Glenoid Resurfacing | Young, high-demand patients (<50) with OA and an intact cuff; Revision of failed hemiarthroplasty for glenoid pain. | Active infection; Inflammatory arthropathy (RA); Irreparable rotator cuff. | Older, low-demand patients (better served by TSA); Severe glenoid retroversion requiring massive bone grafting. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Evaluation and Imaging Modalities
Patients with glenohumeral arthritis typically present with a protracted history of insidious shoulder pain and restricted motion spanning several years, frequently punctuated by a recent, acute exacerbation or "flare." Pain is characteristically exacerbated by overhead activity, reaching away from the body, and profoundly interferes with sleep, often forcing the patient to sleep in a recliner. Physical examination reveals generalized atrophy of the shoulder girdle (particularly the spinati), posterior joint line tenderness, and a symmetrical loss of active and passive range of motion. A disproportionate loss of external rotation with the arm at the side is a clinical hallmark of primary osteoarthritis. Importantly, intact neurologic function must be rigorously documented; concurrent neck pain, distal radiation, or paresthesias should prompt a thorough investigation into cervical radiculopathy or spinal stenosis prior to any shoulder intervention.
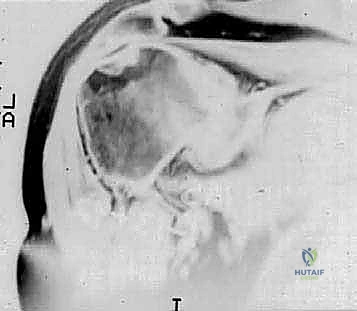
Glenohumeral arthritis is definitively a radiographic diagnosis, and standard imaging protocols are mandatory. A standard trauma series is insufficient; orthogonal views must include a true anteroposterior (Grashey) view in both internal and external rotation, and a high-quality axillary view. Radiographic hallmarks of primary osteoarthritis include profound subchondral sclerosis, expansive cyst formation, inferior humeral osteophytes, and asymmetric posterior joint space narrowing. The axillary view is absolutely critical for assessing the degree of posterior humeral head subluxation and the specific patterns of glenoid wear, which heavily influence surgical decision-making.

Computed Tomography (CT) scanning, preferably with advanced 3D reconstruction capabilities, is the current gold standard for quantifying glenoid version, assessing volumetric bone loss, and classifying the glenoid morphology according to the modified Walch classification system. Walch Type A represents a centered humeral head with concentric wear (A1 minor, A2 major central erosion). Type B denotes posterior subluxation (B1), posterior subluxation with biconcave posterior erosion (B2), or monoconcave posterior wear with severe retroversion (B3). Type C indicates profound glenoid hypoplasia with increased retroversion (>15 degrees) but without posterior subluxation. Type D represents anterior subluxation. Magnetic Resonance Imaging (MRI) is utilized selectively, primarily in patients with rheumatoid arthritis or those with clinical suspicion of a concomitant rotator cuff tear (e.g., profound weakness in external rotation or elevation), to confirm the structural integrity of the cuff prior to committing to an anatomic arthroplasty.
Digital Templating and Patient Positioning
The advent of sophisticated 3D digital templating software has revolutionized preoperative planning in shoulder arthroplasty. Surgeons can now import the patient's CT data to create a virtual 3D model of the scapula and humerus. This allows for precise measurement of glenoid version and inclination relative to the Friedman line (the axis from the medial border of the scapula to the center of the glenoid). Virtual implant placement enables the surgeon to determine the optimal size, configuration (pegged vs. keeled), and seating of the glenoid component. In cases of severe B2 or B3 glenoids, the software can simulate asymmetric anterior reaming to correct version, or template the use of augmented glenoid components (e.g., posterior step or wedge augments) to preserve subchondral bone while restoring the joint line.

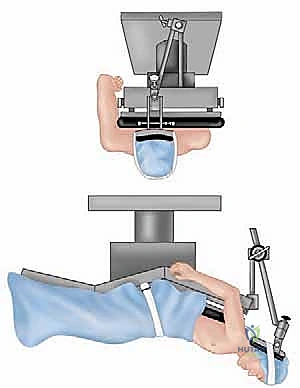
Patient positioning is a critical, often underappreciated aspect of a successful shoulder
Clinical & Radiographic Imaging Archive