Arthroscopic Subscapularis Tendon Repair: A Comprehensive Surgical Guide
Key Takeaway
Arthroscopic subscapularis tendon repair requires meticulous portal placement, precise tendon mobilization, and secure fixation. Recognizing the "comma sign" is critical for identifying retracted tears. The procedure utilizes a four-portal technique, prioritizing subscapularis repair before addressing other rotator cuff pathology. Proper bone bed preparation and advanced suture shuttling techniques ensure robust tendon-to-bone healing, followed by a strict postoperative rehabilitation protocol to protect the repair.
Comprehensive Introduction and Patho-Epidemiology
Historically referred to as the "forgotten tendon" of the rotator cuff, the subscapularis has garnered immense attention over the past two decades as arthroscopic techniques and diagnostic imaging have profoundly evolved. The subscapularis is the largest, strongest, and most biomechanically critical of the rotator cuff muscles, providing more than 50% of the total cuff strength. It functions as the primary internal rotator of the glenohumeral joint and serves as an indispensable dynamic anterior stabilizer. Disruption of the subscapularis tendon severely compromises the delicate biomechanical balance of the shoulder, leading to altered glenohumeral kinematics, superior and anterior humeral head migration, and accelerated degenerative changes.
Epidemiologically, subscapularis tears were previously considered rare, primarily because they were underdiagnosed in the era of open rotator cuff repairs, which predominantly utilized superior or posterior approaches that obscured the anterior compartment. Contemporary arthroscopic data, however, reveals that subscapularis pathology is present in up to 30% of all rotator cuff tears. While isolated subscapularis tears account for approximately 5% to 8% of these lesions, the vast majority occur concomitantly with supraspinatus and infraspinatus tears in the setting of massive, multi-tendon rotator cuff avulsions. The incidence of these tears increases linearly with patient age, mirroring the degenerative pathogenesis seen in the posterosuperior cuff, though traumatic avulsions remain a significant etiology in younger, active populations following forced external rotation or hyperextension injuries.
The pathogenesis of subscapularis tears is multifactorial, encompassing both intrinsic tendon degeneration and extrinsic mechanical impingement. Intrinsic degeneration, characterized by mucoid degeneration, fibrocartilaginous metaplasia, and vascular compromise at the tendon insertion, weakens the structural integrity of the footprint. Extrinsic factors include subcoracoid impingement, where a narrowed coracohumeral distance (typically less than 6 mm) leads to mechanical abrasion of the subscapularis tendon against the coracoid process during internal rotation and forward elevation. Furthermore, the intimate anatomic relationship between the subscapularis and the long head of the biceps tendon (LHBT) means that instability or hypertrophy of the biceps can exert chronic sheer stress on the upper border of the subscapularis, leading to progressive tearing of the superior fascicles.
Advancements in arthroscopic techniques, specifically the systematic approaches pioneered by Burkhart, Tehrany, and Lafosse, have completely revolutionized the management of these lesions. The transition from open subscapularis repair—which often required extensive deltopectoral dissection and morbid tenotomies—to all-arthroscopic management has allowed for precise anatomic restoration with minimized surgical morbidity, reduced postoperative pain, and accelerated rehabilitation. Modern arthroscopic approaches enable the surgeon to visualize the entire footprint, meticulously release capsular adhesions, and achieve robust biomechanical fixation, fundamentally altering the prognostic trajectory for patients with complex anterior shoulder pathology.
Detailed Surgical Anatomy and Biomechanics
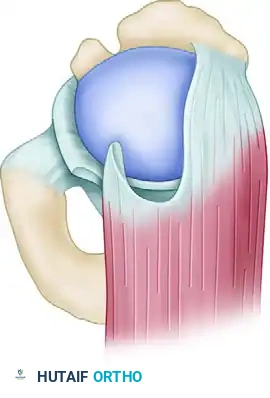
A profound, three-dimensional understanding of anterior shoulder anatomy is the absolute prerequisite for successful arthroscopic subscapularis repair. The subscapularis muscle originates from the subscapular fossa of the anterior scapula and converges laterally to insert onto the lesser tuberosity of the proximal humerus. The footprint is broad and trapezoidal, measuring approximately 40 mm in the superior-to-inferior dimension and 20 mm in the medial-to-lateral dimension. Crucially, the insertion is not purely tendinous; the superior 60% of the footprint consists of a dense, robust tendinous insertion, whereas the inferior 40% is predominantly muscular, inserting directly onto the humeral shaft distal to the lesser tuberosity. This anatomic dichotomy explains why the vast majority of subscapularis tears initiate at the superior border and propagate inferiorly, and why the inferior muscular portion is rarely avulsed entirely.
The superior border of the subscapularis is intimately interwoven with the complex capsuloligamentous structures of the rotator interval, specifically the coracohumeral ligament (CHL) and the superior glenohumeral ligament (SGHL). These structures form the medial sling of the biceps pulley. When the superior subscapularis tears and retracts medially, it takes this capsuloligamentous complex with it, forming the pathognomonic "comma sign"—a critical arthroscopic landmark for identifying the superolateral edge of a retracted tendon. Furthermore, the anterior capsule blends seamlessly with the deep articular surface of the subscapularis tendon. In chronic tears, the tendon becomes densely adherent to the anterior capsule and the base of the coracoid, necessitating meticulous, systematic surgical release to restore lateral excursion without tethering.
Biomechanically, the subscapularis works in concert with the infraspinatus and teres minor to create a transverse force couple in the axial plane. This force couple is responsible for compressing the humeral head into the glenoid concavity during active shoulder elevation, effectively counteracting the superior shear forces generated by the deltoid muscle. When the subscapularis is torn, this transverse force couple is uncoupled. The loss of anterior compression allows the humeral head to translate anteriorly and superiorly, leading to abnormal kinematics, secondary impingement of the remaining intact rotator cuff, and eventual eccentric wear of the superior and anterior glenoid cartilage. Restoring this force couple is the primary biomechanical objective of subscapularis repair.
Neurovascular proximity adds a layer of immense complexity to the surgical mobilization of the subscapularis. The axillary nerve and the posterior humeral circumflex artery traverse the quadrilateral space and run dangerously close to the inferior muscular border of the subscapularis. The axillary nerve is located, on average, just 10 to 15 mm distal to the inferior-most aspect of the subscapularis footprint on the lesser tuberosity, and it courses medially along the anterior surface of the muscle belly. Consequently, any sharp dissection or aggressive electrocautery at the inferior margin of the subscapularis carries a catastrophic risk of axillary nerve denervation. Surgeons must rely on superior, anterior, and posterior releases, utilizing lateral traction to bluntly free the inferior adhesions, thereby safeguarding these critical neurovascular structures.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic subscapularis repair hinges on a meticulous correlation of patient symptomatology, functional deficits, and advanced imaging findings. Patients typically present with localized anterior shoulder pain, pronounced weakness in internal rotation, and a noticeable increase in passive external rotation compared to the contralateral shoulder. Provocative clinical testing is paramount. The Lift-Off test (Gerber) specifically isolates the lower, muscular portion of the subscapularis, while the Belly-Press and Bear-Hug tests are highly sensitive for detecting tears involving the upper tendinous insertion, which constitute the majority of lesions. A positive finding on any of these tests, coupled with MRI evidence of structural failure, forms the foundation for surgical indication.
Surgical intervention is highly indicated for acute, traumatic subscapularis tears in active individuals, regardless of tear size, to prevent rapid medial retraction and irreversible fatty infiltration of the muscle belly. For degenerative tears, surgery is indicated when patients fail a comprehensive course of conservative management (physical therapy, non-steroidal anti-inflammatory drugs, and judicious corticosteroid injections) and continue to experience unacceptable pain and functional limitation. Furthermore, in the setting of massive, multi-tendon rotator cuff tears, repairing the subscapularis is considered an absolute necessity to restore the transverse force couple and dynamic anterior stability, even if the posterosuperior cuff is deemed irreparable.
However, not all subscapularis tears are amenable to arthroscopic repair. Advanced fatty infiltration and muscle atrophy—specifically Goutallier stage 3 (equal fat and muscle) or stage 4 (more fat than muscle)—are strong relative contraindications, as the degenerated muscle is unlikely to regain functional contractility even if anatomic healing is achieved. Additionally, fixed anterior or superior glenohumeral escape with advanced cuff tear arthropathy (Hamada Grade 3 or higher) renders isolated tendon repair futile, as the glenohumeral joint biomechanics are irreversibly destroyed. In such advanced degenerative states, alternative salvage procedures, such as reverse total shoulder arthroplasty, are more appropriate.
| Category | Indications for Arthroscopic Repair | Contraindications for Arthroscopic Repair |
|---|---|---|
| Absolute | Acute traumatic avulsion in an active patient | Active joint infection or osteomyelitis |
| Absolute | Concomitant subscapularis tear in a massive cuff tear | Severe glenohumeral osteoarthritis (Cuff Tear Arthropathy) |
| Relative | Symptomatic partial or full-thickness degenerative tears failing conservative care | Advanced fatty infiltration (Goutallier Stage 3 or 4) |
| Relative | Subcoracoid impingement with associated upper border tearing | Chronic, fixed anterosuperior humeral head escape |
| Relative | Biceps instability secondary to subscapularis/pulley failure | Medical comorbidities precluding general anesthesia |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive preoperative planning begins with high-quality imaging. Magnetic Resonance Imaging (MRI), preferably a non-contrast 3-Tesla scan or an MR arthrogram, is the gold standard for evaluating the subscapularis. The surgeon must meticulously analyze the axial and sagittal oblique sequences to assess the integrity of the footprint on the lesser tuberosity, the degree of medial tendon retraction, and the presence of subcoracoid stenosis. Crucially, the sagittal T1-weighted images must be scrutinized to evaluate the degree of fatty infiltration in the subscapularis muscle belly according to the Goutallier classification, as this is the single most important prognostic indicator for functional recovery and structural healing.
In addition to evaluating the tendon itself, the surgeon must preoperatively assess the status of the long head of the biceps tendon (LHBT). Medial subluxation or frank dislocation of the LHBT into the glenohumeral joint is a pathognomonic sign of a complete superior subscapularis tear and failure of the biceps pulley. Preoperative identification of biceps pathology dictates that a biceps tenodesis or tenotomy must be incorporated into the surgical plan. Furthermore, measuring the coracohumeral distance on axial MRI is essential; a distance of less than 6 mm suggests subcoracoid impingement, alerting the surgeon to the potential need for a concomitant arthroscopic coracoplasty to protect the repaired tendon from mechanical abrasion.
Patient positioning and anesthesia are critical components of the preoperative setup that directly influence intraoperative success. The procedure is typically performed under general anesthesia, supplemented with an ultrasound-guided interscalene regional nerve block. This multimodal analgesic approach minimizes intraoperative anesthetic requirements, provides profound muscle relaxation (which is essential for mobilizing retracted tendons), and ensures excellent immediate postoperative pain control. Strict attention must be paid to protecting all bony prominences and peripheral nerves during positioning to prevent positioning-related neuropathies.
The surgeon may choose either the lateral decubitus or the beach chair position, though the beach chair position is overwhelmingly preferred by most shoulder surgeons for isolated or complex subscapularis repairs. The beach chair position allows for unhindered, dynamic manipulation of the arm throughout the procedure. The ability to freely internally and externally rotate the arm, as well as vary the degree of forward elevation, is absolutely critical for visualizing the lesser tuberosity footprint, exposing hidden partial tears, and assessing the tension on the repaired tendon in real-time. A pneumatic arm holder is highly recommended to maintain the arm in precise positions, freeing the surgical assistant to manage traction sutures and instrumentation.
Step-by-Step Surgical Approach and Fixation Technique
Portal Placement and Diagnostic Arthroscopy
Optimal portal placement is the absolute cornerstone of a successful arthroscopic subscapularis repair. A dedicated four-portal technique, as popularized by Burkhart and Tehrany, is utilized to ensure adequate viewing angles and appropriate trajectory for instrumentation in the confined anterior compartment. The standard posterior portal is established first and is used primarily for arthroscopic viewing, providing a panoramic view of the subscapularis tendon and its bone bed on the lesser tuberosity. An anterior portal is then established via an outside-in technique using a spinal needle through the rotator interval, ensuring the trajectory is perfectly perpendicular to the lesser tuberosity for optimal anchor placement.
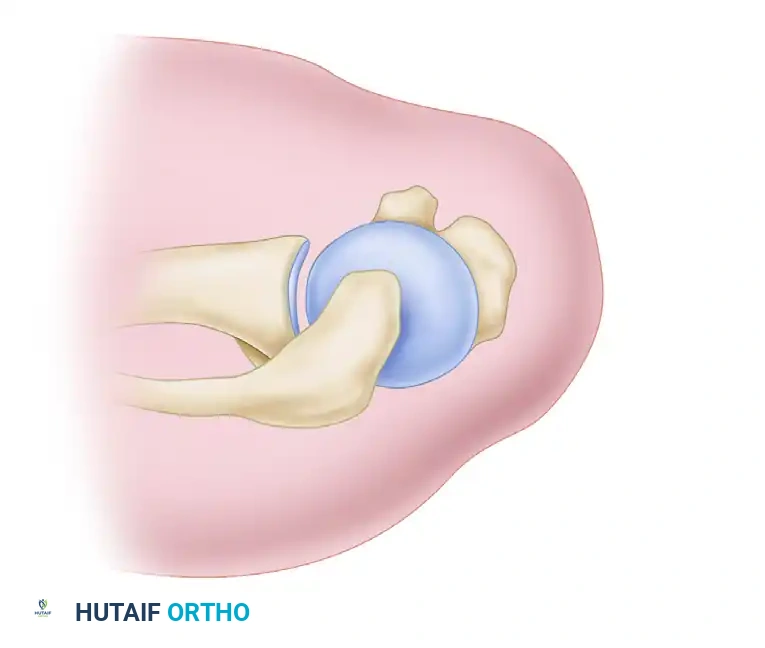
Figure 1: Burkhart and Tehrany portals for arthroscopic subscapularis repair. (A) Anterior portal for anchor placement. (B) Anterolateral portal for mobilization. (C) Accessory anterolateral portal for traction sutures. (D) Posterior portal for viewing.
Two additional working portals are critical for complex repairs. The anterolateral portal is placed just anterior to the biceps tendon and serves as the primary working portal for subscapularis mobilization, capsular release, and preparation of the bone bed. Finally, an accessory anterolateral portal is placed just posterior to the biceps tendon. This portal is dedicated to managing traction sutures, which are essential for controlling the tendon during mobilization and repair. With the arthroscope in the posterior portal, a thorough diagnostic sweep is performed. The surgeon must dynamically manipulate the arm, utilizing internal rotation to relax the intact portion of the subscapularis, thereby exposing hidden articular-sided partial tears or the "bare footprint" of the lesser tuberosity.
Tear Recognition and Management of the Biceps
Subscapularis tears, particularly those that are chronic and retracted, can be notoriously difficult to visualize. The tendon edge often retracts medially, blending seamlessly with the anterior capsule and the base of the coracoid. When facing a retracted tear, the surgeon must actively search for the "comma sign." The medial sling of the biceps—composed of the SGHL and CHL—remains attached to the superolateral portion of the torn subscapularis tendon. As the tendon retracts medially, this capsuloligamentous complex forms a distinct, comma-shaped arc just above the superolateral corner of the subscapularis. Identifying this comma tissue is the master key to locating the superolateral edge of the retracted tendon.
Once the tear is identified, the long head of the biceps tendon must be addressed. Pathology of the subscapularis almost universally compromises the biceps pulley, leading to instability. If the biceps is subluxated medially into the joint, dislocated, or exhibits significant structural tearing, an arthroscopic tenotomy or tenodesis must be performed. Leaving an unstable or pathologic biceps tendon in situ will not only result in persistent anterior shoulder pain but will also mechanically interfere with the subscapularis repair, potentially leading to early failure. The biceps is typically tenotomized at its labral origin and subsequently tenodesed in the bicipital groove or subpectorally, depending on surgeon preference.
Interval Slide and Tendon Mobilization
For massive, contracted rotator cuff tears involving the subscapularis, achieving a tension-free repair requires aggressive, systematic mobilization. An interval slide technique, as described by Tauro et al., is often necessary to allow lateral excursion of the tendon without undue tension. This involves releasing the scarred rotator interval tissue between the superior border of the subscapularis and the anterior border of the supraspinatus.
Figure 2: Basket punch inserted through the lateral subacromial portal to begin the interval release.
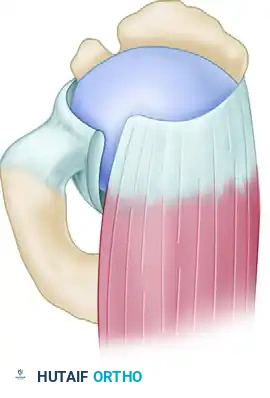
Figure 3: Completed interval slide release for a crescentic tear.
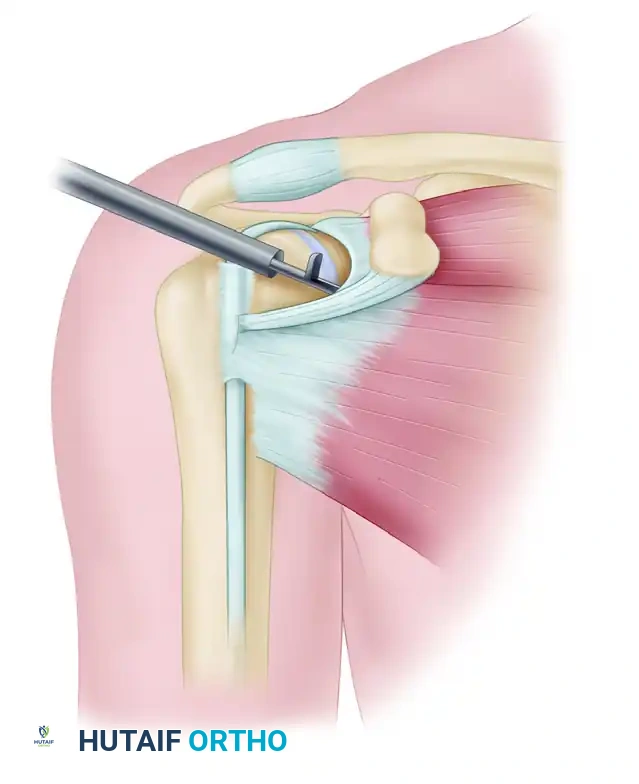
Figure 4: Completed interval slide release for a longitudinal tear.
If the tendon still cannot be easily reduced over the bone bed, a rigorous three-sided release is performed. A traction suture is passed through the superolateral edge of the subscapularis tendon and retrieved through the accessory anterolateral portal. While exerting lateral traction on the tendon, an arthroscopic elevator or electrocautery device is introduced through the anterolateral portal to systematically mobilize the anterior, posterior, and superior aspects of the subscapularis. The surgeon must meticulously free the deep articular surface of the tendon from the anterior glenoid neck and capsule, and the anterior surface from the base of the coracoid process.
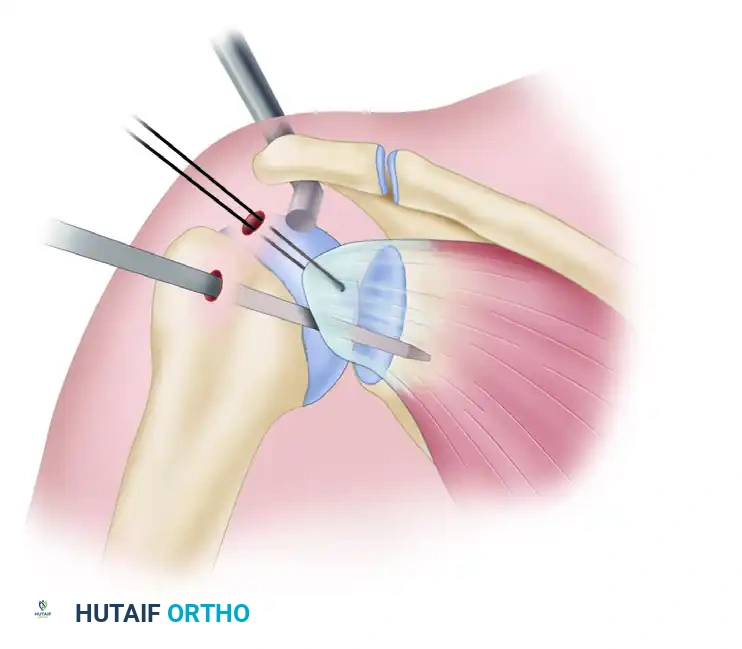
Figure 5: Superior view of subscapularis mobilization using an arthroscopic elevator while applying tension via a traction suture.
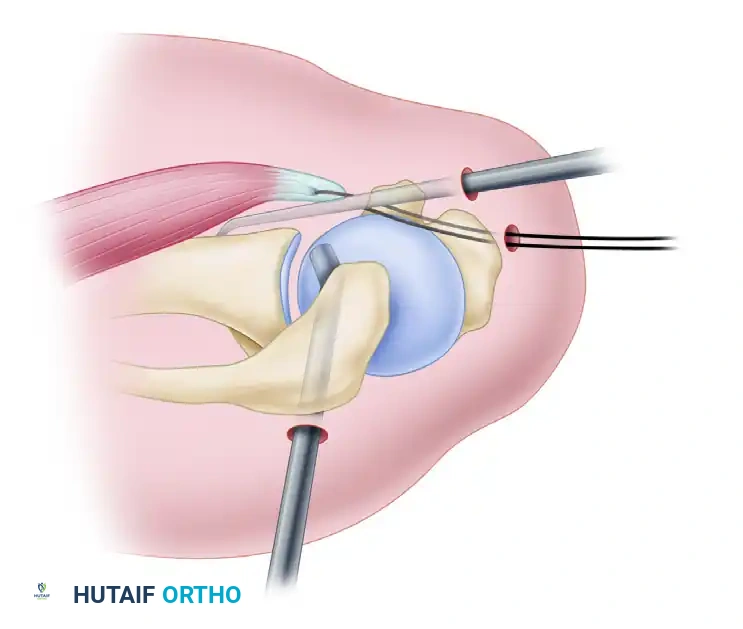
Figure 6: Anterior view demonstrating the elevator freeing the capsular adhesions from the subscapularis.
Crucially, the surgeon must strictly avoid dissecting or cutting near the inferior border of the subscapularis tendon. The axillary nerve and posterior humeral circumflex vessels run dangerously close to this inferior margin. By comprehensively freeing the anterior, posterior, and superior borders, the application of lateral traction on the tendon will effectively and safely disrupt any remaining inferior adhesions through blunt tension, completely minimizing the risk of catastrophic neurovascular injury.
Bone Bed Preparation and Fixation Techniques
A robust biological healing response requires a meticulously prepared, bleeding bone bed. A high-speed arthroscopic burr is introduced through the anterolateral portal to decorticate the lesser tuberosity footprint. To maximize tendon-to-bone contact and reduce tension on the repair, the bone bed is often medialized by approximately 5 mm. This is achieved by removing the articular cartilage at the medial margin of the footprint down to a bleeding cancellous base, creating an optimal environment for osteotendinous integration.
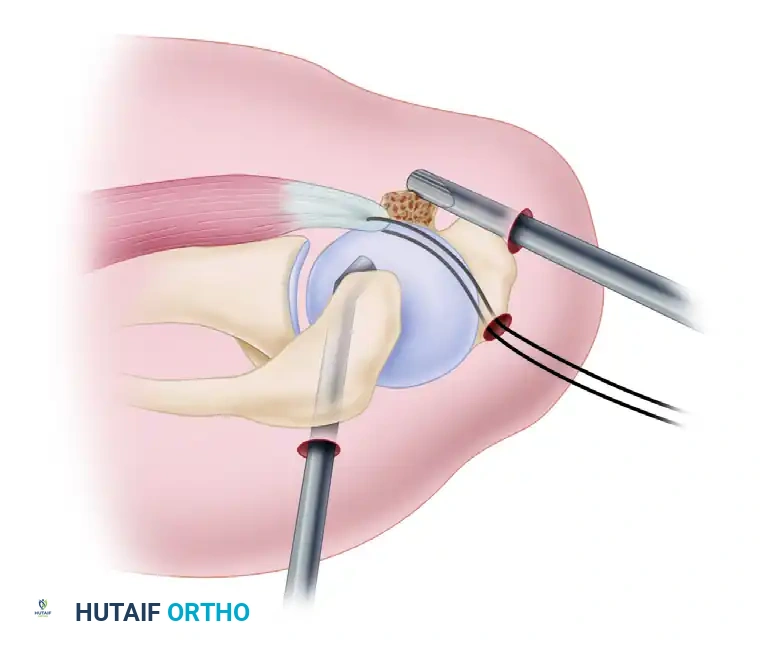
Figure 7: Preparation of the bone bed on the lesser tuberosity using a high-speed burr (superior view).
The choice of fixation depends on the size of the tear and the degree of tendon excursion achieved. For complete tears, two or more anchors are generally required to recreate the broad footprint of the subscapularis. Standard screw-type or all-suture anchors are placed via the anterior portal, ensuring a deadman's angle of 45 degrees to the bone surface to maximize pullout strength. For large, retracted tears, passing sutures can be technically demanding. The "traction shuttle" technique is highly effective: braided sutures from the seated anchor are threaded through a loop created on the pre-existing traction suture. As the traction suture is pulled out of the tendon, it shuttles the anchor's sutures through the tissue. The sutures are then retrieved through the anterolateral portal, and arthroscopic knot tying or knotless fixation is performed, securing the tendon firmly to the prepared footprint.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced instrumentation, arthroscopic subscapularis repair carries a distinct profile of potential complications. The most common complication is postoperative stiffness, particularly a persistent deficit in external rotation. This is often the result of overtensioning the repair, inadequate capsular release during the initial mobilization, or a failure of the patient to strictly adhere to the phased rehabilitation protocol. While mild stiffness is often tolerated and may even protect the repair during the early healing phases, severe adhesive capsulitis requires aggressive physical therapy and, occasionally, arthroscopic capsular release once the tendon has definitively healed (typically beyond 6 months postoperatively).
Structural failure, or retear, is the most dreaded complication, with incidence rates ranging from 5% in small, isolated tears to upwards of 20% in massive, multi-tendon repairs with advanced chronicity. Retears are heavily correlated with preoperative fatty infiltration (Goutallier stage 3 or higher), patient age over 65, and the use of single-row fixation in massive tears. A retear often presents with recurrent anterior shoulder pain, a positive lift-off or belly-press sign, and a return of profound weakness. If a retear is identified, revision arthroscopic repair may be attempted if the tendon quality permits and the muscle has not undergone irreversible atrophy.
Neurologic injury, specifically to the axillary nerve, is a rare but catastrophic complication, occurring in less than 1% of cases. It is almost exclusively associated with overzealous sharp dissection or electrocautery at the inferior border of the subscapularis muscle belly. Symptoms include profound deltoid weakness, inability to abduct the arm, and numbness over the lateral shoulder badge area. Iatrogenic axillary nerve injuries require immediate neurological workup, EMG studies, and potentially nerve exploration and grafting if recovery is not observed within 3 to 6 months.
| Complication | Estimated Incidence | Primary Etiology | Salvage / Management Strategy |
|---|---|---|---|
| Postoperative Stiffness | 10% - 15% | Overtensioning, prolonged immobilization | Aggressive physical therapy, eventual arthroscopic capsulotomy |
| Structural Retear | 5% - 20% | Poor tissue quality, advanced fatty infiltration | Revision repair, Pectoralis Major transfer, RTSA |
| Axillary Nerve Injury | < 1% | Sharp dissection at the inferior tendon border | Observation, EMG/Nerve conduction, Nerve grafting |
| Hardware Failure / Anchor Pullout | 1% - 3% | Osteoporotic bone, improper anchor trajectory | Revision fixation with larger or alternative anchors |
| Coracoid Impingement | 2% - 5% | Failure to address narrowed coracohumeral distance | Arthroscopic coracoplasty (subcoracoid decompression) |
When revision arthroscopic repair is deemed impossible due to complete tendon retraction, severe tissue degradation, or advanced Goutallier stage 4 fatty infiltration, salvage procedures must be considered. In younger, active patients with an irreparable subscapularis tear but an intact posterosuperior rotator cuff, a pectoralis major tendon transfer is the procedure of choice. This transfer routes the sternal head of the pectoralis major either deep or superficial to the conjoint tendon to insert on the lesser tuberosity, effectively restoring the anterior force couple. In older patients, or those with concomitant irreparable superior cuff tears and advancing glenohumeral arthritis, a Reverse Total Shoulder Arthroplasty (RTSA) is the definitive salvage procedure, relying on deltoid tension rather than a functional rotator cuff to achieve overhead elevation and joint stability.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following arthroscopic subscapularis repair is arguably as critical to the final clinical outcome as the surgical procedure itself. The protocol must delicately balance the biological requirement for undisturbed tissue healing with the biomechanical necessity of preventing profound postoperative stiffness. Because the subscapularis functions as an internal rotator, the act of external rotation places direct, linear tension on the repaired tendon footprint. Therefore, the rehabilitation phases are heavily dictated by the need to protect the repair from premature external rotation stress.
Phase I: Protection and Immobilization (Weeks 0-6)
During the initial six weeks, the primary goal is absolute protection of the surgical repair. The patient is strictly immobilized in a padded shoulder sling, ideally positioned in approximately 30 degrees of internal rotation. This position minimizes tension on the lesser tuberosity footprint. Strict restrictions are enforced: external rotation beyond neutral (0 degrees) is absolutely prohibited. Active internal rotation is completely restricted to prevent active muscle contraction from avulsing the repair. Active or passive overhead elevation is also severely restricted to protect the repair and any concomitant superior cuff repairs. To prevent distal stiffness and vascular stasis, elbow, wrist, and hand active range of motion exercises are encouraged immediately on postoperative day one.
Phase II: Passive Range of Motion (Weeks 6-10)
At the six-week mark, biologic healing has progressed sufficiently to allow the discontinuation of the sling and the initiation of controlled passive range of motion (PROM). The focus shifts to restoring forward elevation in the scapular plane and gentle, progressive external rotation. The physical therapist must be acutely aware of the intraoperative tension assessments documented by the surgeon. External rotation is gradually increased, typically aiming for 30 degrees by week 8, and progressing toward symmetrical external rotation by week 10. All movements must remain strictly passive; active internal rotation is still avoided to protect the maturing osteotendinous junction.
Phase III: Active Range of Motion and Early Strengthening (Weeks 10-14)
As the patient enters the third month postoperatively, the protocol transitions to active-assisted and eventually full active range of motion (AROM). The patient begins utilizing pulleys, wands, and gravity-eliminated positions to restore active kinematics. Gentle, sub-maximal isometric internal rotation exercises are introduced to begin re-educating the subscapularis muscle belly without subjecting the tendon to dynamic sheer forces. The physical therapist must continue to avoid aggressive end-range stretching or sudden, forceful external rotation movements, as the tendon is still undergoing critical remodeling and maturation.
Phase IV: Advanced Strengthening and Return to Activity (Weeks 14+)
In the final phase of rehabilitation, progressive resistive exercises are implemented to rebuild the strength and endurance of the rotator cuff and periscapular stabilizers. Isotonic strengthening using resistance bands and light free weights is initiated, focusing on restoring the transverse force couple. Closed kinetic chain exercises are utilized to enhance proprioception and dynamic glenohumeral stability. Return to heavy labor, heavy lifting, or contact sports is generally delayed until at least 6 months postoperatively, and is strictly contingent upon the patient demonstrating symmetrical, pain-free range of motion, normal scapulothoracic rhythm, and at least 90% strength recovery compared to the contralateral shoulder.
Summary of Landmark Literature and Clinical Guidelines
The evolution of arthroscopic subscapularis repair is deeply rooted in several landmark biomechanical and clinical studies that have fundamentally shifted orthopedic paradigms. Historically, Christian Gerber’s seminal work in the early 1990s established the functional importance of the subscapularis and introduced the Lift-Off test, proving that isolated subscapularis tears were a distinct clinical entity that caused profound disability. Gerber’s initial open repair outcomes demonstrated significant improvements in pain and function, but the morbidity of the open approach highlighted the need for minimally invasive alternatives.
The arthroscopic revolution for subscapularis repair was spearheaded by Stephen Burkhart and his description of the "comma sign" in 2003. Burkhart meticulously detailed how the medial sling of the biceps—comprising the SGHL and CHL—remains attached to the superolateral corner of the torn subscapularis, forming a comma-shaped arc as the tendon retracts. This single anatomic observation provided arthroscopic surgeons with a reliable, reproducible roadmap for identifying and mobilizing retracted, previously "hidden" subscapularis tears. Burkhart and Tehrany subsequently published their comprehensive four-portal technique, establishing the standard of care for portal placement and trajectory that remains in widespread use today.
The classification of subscapularis tears was significantly refined by Laurent Lafosse in 2
