Operative Management of Full-Thickness Rotator Cuff Tears
Key Takeaway
Full-thickness rotator cuff tears require meticulous surgical planning and biomechanical restoration of the tendon footprint. This guide outlines evidence-based algorithms for arthroscopic repair, emphasizing tear pattern recognition—such as acute and chronic L-shaped configurations—and the critical principle of margin convergence. By tailoring anchor constructs and suture passes to tear size, surgeons can optimize footprint coverage, minimize tension at the muscle-tendon interface, and significantly improve postoperative healing rates.
Comprehensive Introduction and Patho-Epidemiology
The operative management of full-thickness rotator cuff tears represents a cornerstone of modern orthopedic shoulder surgery, reflecting decades of evolution in biomechanical understanding, surgical instrumentation, and biological augmentation. The primary objective of surgical intervention is to achieve a biomechanically stable, tension-free repair that restores the anatomical footprint of the rotator cuff, thereby optimizing the biological environment for tendon-to-bone healing. Historically, the biologic healing of rotator cuff repairs has been a subject of intense academic scrutiny. Early arthroscopic techniques yielded variable results, often inferior to their open counterparts regarding structural integrity. As noted in foundational literature, early arthroscopic procedures performed in the late 1990s and early 2000s demonstrated less evidence of robust healing, largely due to the biomechanical limitations of early anchor designs and single-row constructs that failed to adequately compress the tendon against the tuberosity.
The patho-epidemiology of rotator cuff disease is fundamentally age-dependent, representing a continuum from tendinosis to partial tearing, and ultimately, to full-thickness and massive rotator cuff tears. Epidemiological studies utilizing cadaveric and ultrasonographic data indicate that the prevalence of full-thickness tears increases exponentially with age, affecting approximately 25% of individuals in their sixties and exceeding 50% in octogenarians. The etiology is multifactorial, encompassing both intrinsic and extrinsic mechanisms. Intrinsic theories emphasize age-related microvascular compromise—specifically within the "critical zone" of the supraspinatus tendon, located 10 to 15 millimeters proximal to its insertion—leading to degenerative microtearing, apoptosis, and impaired healing capacity. Extrinsic theories, initially championed by Neer, focus on mechanical impingement of the rotator cuff against the coracoacromial arch, particularly in the presence of a Type III (hooked) acromion or acromioclavicular joint osteophytosis.
Modern academic consensus acknowledges that rotator cuff pathogenesis is a synergistic combination of these intrinsic and extrinsic factors, further complicated by genetic predispositions and metabolic comorbidities such as diabetes mellitus and hypercholesterolemia. When a full-thickness tear occurs, the normal biomechanical force couples of the glenohumeral joint are disrupted. The uncoupling of the anterior (subscapularis) and posterior (infraspinatus and teres minor) forces leads to superior migration of the humeral head under the unopposed pull of the deltoid. Over time, this mechanical dysfunction results in progressive tendon retraction, capsular contracture, and irreversible myotendinous architectural changes, including muscle atrophy and fatty infiltration.
The transition from older, high-failure-rate techniques to modern surgical success is rooted in the recognition of these complex tear patterns and the application of advanced biomechanical principles, such as margin convergence and footprint maximization. Restoring the biomechanical linkage of the rotator cable is paramount to preventing tension overload at the repair site. Today, with the evolution of transosseous-equivalent (TOE) suture-bridge techniques and a deeper understanding of tear morphology, arthroscopic repairs of full-thickness cuff tears heal reliably when meticulous attention is paid to footprint restoration, mechanical stability, and biological optimization.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the shoulder girdle is the sine qua non for successful rotator cuff repair. The rotator cuff comprises four musculotendinous units—the supraspinatus, infraspinatus, teres minor, and subscapularis—that dynamically stabilize the glenohumeral joint while facilitating a massive range of motion. The supraspinatus and infraspinatus tendons fuse near their insertion, forming a continuous, interwoven fibrous structure rather than distinct, isolated tendinous bands. This complex inserts onto the greater tuberosity in a highly specific footprint. Cadaveric studies have meticulously mapped this footprint, revealing that the supraspinatus insertion is primarily located on the superior facet of the greater tuberosity, measuring approximately 16 mm in medial-to-lateral width and 25 mm in anterior-to-posterior length. The infraspinatus inserts onto the middle facet, while the teres minor inserts onto the inferior facet.
The microanatomy of the tendon-to-bone insertion site, or enthesis, is critical to understanding repair biology. The native enthesis is a specialized transitional tissue divided into four distinct histological zones: tendon, uncalcified fibrocartilage, calcified fibrocartilage, and bone. This gradual transition mitigates stress concentrations at the interface between the compliant tendon and the rigid bone. Surgical repair, however, does not regenerate this complex four-zone enthesis; rather, it heals via a fibrovascular scar tissue interface mediated by Sharpey’s fibers. Because this scar tissue is biomechanically inferior to the native enthesis, the surgical construct must provide absolute mechanical stability to protect the healing interface during the critical early phases of biological remodeling.
From a biomechanical perspective, the rotator cuff functions through the establishment of force couples in both the coronal and transverse planes. In the coronal plane, the inferiorly directed force of the rotator cuff counterbalances the superiorly directed force of the deltoid, centering the humeral head within the glenoid concavity during arm elevation. In the transverse plane, the anterior force of the subscapularis is balanced by the posterior forces of the infraspinatus and teres minor. Disruption of these force couples, particularly in massive tears, results in altered kinematics, superior humeral head escape, and accelerated glenohumeral arthropathy.
Furthermore, the architectural concept of the "rotator cable" and "rotator crescent," as popularized by Burkhart, is essential for intraoperative decision-making. The rotator cable is a thick, fibrous band of tissue extending from the coracohumeral ligament anteriorly to the inferior margin of the infraspinatus posteriorly. It acts much like the suspension cable of a bridge, stress-shielding the thinner, more avascular rotator crescent tissue that inserts laterally onto the greater tuberosity. In older patients with degenerative tears, the crescent tissue often fails, but if the cable remains intact and functionally attached to the tuberosity, the shoulder may remain biomechanically compensated. Surgical repair must aim to restore the integrity of the rotator cable and its linkage to the bony footprint to re-establish the suspension bridge biomechanics, thereby reducing strain on the repaired crescent tissue.
Exhaustive Indications and Contraindications
The decision to proceed with operative management of a full-thickness rotator cuff tear requires a nuanced synthesis of patient-specific variables, including chronological and physiological age, functional demands, symptom duration, tear morphology, and the presence of irreversible degenerative changes. Surgery is not universally indicated for all full-thickness tears, as a significant proportion of degenerative tears in the elderly population can be managed successfully with structured physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), and judicious corticosteroid injections. However, strict parameters exist where surgical intervention is highly recommended to prevent irreversible structural damage and functional decline.
Acute, traumatic full-thickness tears in young or highly active patients represent an absolute indication for early surgical repair. Delayed intervention in these cases leads to rapid tendon retraction, muscle atrophy, and a significant decrease in the probability of achieving a structurally sound, tension-free repair. In the setting of chronic, degenerative tears, surgery is indicated when patients experience persistent pain and functional limitation that are refractory to a minimum of three to six months of comprehensive non-operative management. Additionally, the progression of tear size is a critical factor; asymptomatic tears that demonstrate enlargement on serial imaging, or those that transition from asymptomatic to symptomatic, warrant operative consideration to halt the degenerative cascade.
Conversely, absolute and relative contraindications must be respected to avoid catastrophic surgical failures and patient morbidity. The presence of advanced glenohumeral osteoarthritis, specifically cuff tear arthropathy (Hamada Grade 3 or higher), precludes isolated rotator cuff repair, as the altered joint mechanics and cartilage loss will not be addressed by tendon repair alone; such patients are better served by reverse total shoulder arthroplasty (RTSA). Furthermore, irreversible muscle degeneration, characterized by severe fatty infiltration (Goutallier Grade 3 or 4) and profound muscle atrophy (Thomazeau Grade 3), serves as a strong relative contraindication. In these scenarios, the muscle has lost its contractile capability, and repairing the tendon will not restore function but will merely subject the patient to a high risk of structural failure and persistent pseudoparalysis.
Indications and Contraindications Matrix
| Category | Specific Criteria | Clinical Rationale / Impact |
|---|---|---|
| Absolute Indications | Acute traumatic tear in an active patient (<60 years). | Prevents rapid retraction and irreversible muscle atrophy; maximizes healing potential. |
| Relative Indications | Chronic symptomatic tear failing >3-6 months of conservative care. | Alleviates intractable pain and restores function in patients with preserved muscle quality. |
| Relative Indications | Asymptomatic tear demonstrating significant enlargement on serial MRI. | Halts the progression to a massive, irreparable tear and preserves the glenohumeral force couples. |
| Relative Contraindications | Goutallier Grade 3 or 4 fatty infiltration / Severe atrophy. | High rate of structural failure; muscle contractility is permanently lost. Consider salvage options. |
| Relative Contraindications | Concomitant severe adhesive capsulitis (stiff shoulder). | Repairing a stiff shoulder exacerbates postoperative stiffness. Capsule must be released or rehabilitated first. |
| Absolute Contraindications | Advanced Cuff Tear Arthropathy (CTA) / Hamada Grade $/ge$ 3. | Glenohumeral joint is destroyed. Isolated repair will fail. RTSA is the definitive treatment. |
| Absolute Contraindications | Active glenohumeral joint infection. | Implantation of foreign bodies (anchors/sutures) in an infected field guarantees chronic osteomyelitis. |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical Assessment and Advanced Imaging
Pre-operative planning begins with a meticulous clinical examination to define the impingement profile and isolate specific musculotendinous deficits. Patients typically present with night pain, weakness in elevation and external rotation, and compensatory scapulothoracic dyskinesia. The integrity of the supraspinatus is assessed via Jobe’s test (empty can) and the full can test. The infraspinatus and teres minor are evaluated through resisted external rotation with the arm at the side, the external rotation lag sign, and the hornblower's sign. The subscapularis, often the "forgotten tendon," must be rigorously tested using the lift-off test, belly-press test, and bear-hug test. A positive lag sign in any plane is a poor prognostic indicator, strongly suggesting a massive, retracted tear with significant muscle dysfunction.
Magnetic Resonance Imaging (MRI) without contrast remains the gold standard for evaluating full-thickness tears, providing exquisite soft-tissue detail. The surgeon must systematically evaluate tear size and retraction in both the coronal and sagittal planes, utilizing the Patte classification to quantify medial retraction relative to the glenoid face. Crucially, muscle atrophy and fatty infiltration must be graded using the Goutallier classification on T1-weighted sagittal oblique images (Y-view). Grade 0 represents normal muscle; Grade 1 shows fatty streaks; Grade 2 has more muscle than fat; Grade 3 has equal fat and muscle; and Grade 4 has more fat than muscle. Grades 3 and 4 are generally considered irreversible and portend a significantly higher rate of structural failure post-repair. Additionally, the acromial morphology, presence of an os acromiale, and the status of the long head of the biceps tendon (LHBT) must be templated to plan for concomitant procedures such as acromioplasty or biceps tenodesis.
Patient Positioning and Operating Room Setup
The procedure can be performed in either the beach-chair or lateral decubitus position, a decision largely dictated by surgeon preference, training background, and specific tear morphology.
The Beach Chair Position offers excellent anatomical orientation, facilitating an intuitive understanding of the shoulder's three-dimensional geometry. It allows for unrestricted access to the anterior, superior, and posterior aspects of the shoulder, and permits intraoperative assessment of arm range of motion without the hindrance of traction. Furthermore, it allows for a seamless conversion to an open or mini-open procedure if arthroscopic techniques prove insufficient. However, the beach chair position carries a known risk of cerebral hypoperfusion events due to the hydrostatic gradient between the heart and the brain. Meticulous anesthetic management, maintaining mean arterial pressure (MAP) parameters, is mandatory.
The Lateral Decubitus Position utilizes longitudinal and lateral traction (typically 10 to 15 pounds) to distract the glenohumeral joint and expand the subacromial space. This provides unparalleled visualization of the articular surface of the rotator cuff and the inferior capsule. It is particularly advantageous for managing massive, retracted tears that require extensive capsular releases and mobilization. The primary disadvantages include a steeper learning curve for anatomical orientation (as the anatomy is rotated 90 degrees) and the risk of traction-related neurapraxia to the brachial plexus if traction weight or duration is excessive. Regardless of the chosen position, meticulous padding of all bony prominences and strict adherence to positioning protocols are essential to prevent perioperative complications.
Step-by-Step Surgical Approach and Fixation Technique
Recognizing the geometric configuration of the tear is the most critical step in arthroscopic rotator cuff repair. Failure to recognize the tear pattern leads to non-anatomic, high-tension repairs that are doomed to mechanical failure. Tears are rarely simple, two-dimensional avulsions; they are complex, three-dimensional structural failures that must be reduced along their specific axes of mobility. Following diagnostic arthroscopy and meticulous footprint preparation—which involves light decortication to a bleeding cortical bed (the "crimson crescent") without violating the structural integrity of the subcortical bone—the surgeon must classify and address the specific tear pattern.
Acute L-Shaped Tears
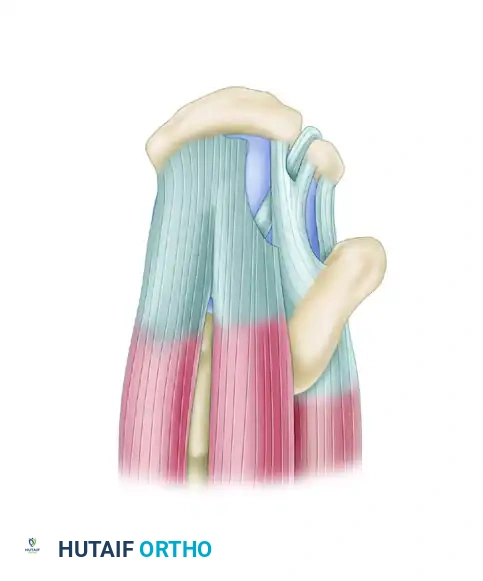
Acute L-shaped tears typically involve the supraspinatus and the rotator interval. These tears possess a longitudinal component (parallel to the tendon fibers) and a transverse component (avulsed from the greater tuberosity).
Superior view of an acute L-shaped rotator cuff tear involving the supraspinatus and rotator interval.
The biomechanical principle of repairing an L-shaped tear dictates that the longitudinal split must be addressed first. Attempting to pull the apex of the tear directly lateral to the tuberosity will result in excessive tension, dog-ear deformity, and inevitable failure.
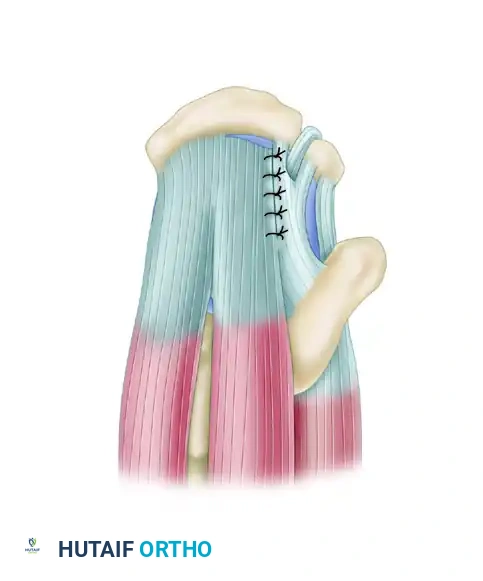
Tears should be initially repaired along the longitudinal split using side-to-side sutures.
By utilizing side-to-side sutures (such as a figure-of-eight or simple interrupted configuration) using ultra-high-molecular-weight polyethylene (UHMWPE) suture, the longitudinal split is closed. Once this split is closed, the tear is effectively converted into a smaller, manageable crescent-shaped tear. This converged margin can then be repaired directly to the bone footprint with minimal tension.

The converged margin is finally repaired to the bone footprint.
Chronic L-Shaped and U-Shaped Tears
When an L-shaped tear is left untreated, chronic retraction, capsular contracture, and biological remodeling cause it to assume a retracted U-shaped configuration.
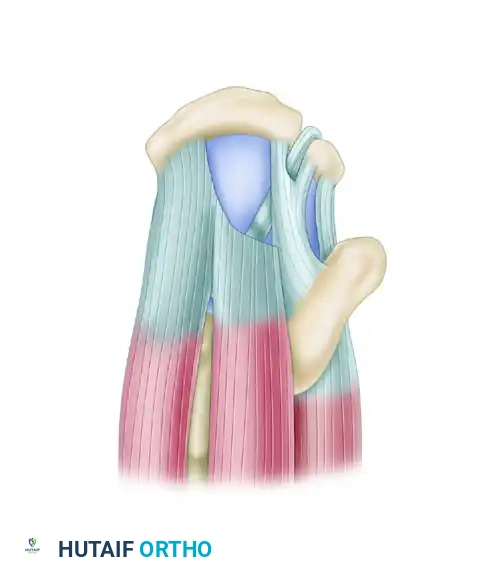
Superior view of a chronic L-shaped tear, which has retracted and assumed a U-shaped configuration.
Despite their retracted appearance, these tears often exhibit excellent mobility from an anterior-to-posterior direction. Typically, one tear margin (usually the posterior leaf involving the infraspinatus) is more mobile than the anterior leaf. The principle of margin convergence, pioneered by Burkhart, is absolutely essential in this scenario.

Tears should be initially repaired using side-to-side sutures, applying the principle of margin convergence to reduce strain on the final bone repair.
By placing side-to-side sutures starting at the medial apex of the tear and working laterally, the surgeon essentially "zips" the tear closed. This technique significantly reduces the strain on the free edge of the tendon, converting a massive U-shaped defect into a functional crescent.

The converged margin is then repaired to the bone in a tension-free manner.
Never attempt to pull a chronic U-shaped tear directly lateral to the tuberosity without first performing margin convergence. Doing so will exceed the ultimate tensile strength of the tendon, leading to immediate intraoperative suture pull-through or early postoperative failure.
Evidence-Based Fixation Strategies and the Suture Bridge
The decision to perform a single-row versus a double-row repair depends heavily on the size of the tear, the quality of the tendon, and the surgeon's technical proficiency. Footprint coverage must be obtained under physiological tension. Biomechanical studies have definitively demonstrated that transosseous-equivalent (TOE) or suture-bridge double-row constructs provide superior load-to-failure strength, minimize gap formation, and optimize contact pressure and area at the tendon-bone interface compared to traditional single-row repairs.
For small tears (< 1.0 cm), a single-row repair using one or two anchors with triple-loaded sutures provides adequate compression without overcrowding the footprint. For medium-to-large tears (1.5 cm to 3.0 cm), a double-row TOE construct is favored. In this technique, a medial row of anchors is placed at the articular margin. The sutures are passed through the tendon, and medial knots are tied (or knotless medial anchors are used). The remaining suture tails are then crisscrossed over the bursal surface of the tendon and secured laterally with knotless anchors placed on the lateral cortex of the greater tuberosity. This creates a pressurized seal against synovial fluid intrusion, which is known to contain lytic enzymes that inhibit tendon healing. For massive, chronically retracted tears where lateral excursion is limited despite extensive releases (including coracohumeral ligament release), medializing the footprint and utilizing a robust single-row repair is preferred to avoid over-tensioning the construct.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and adherence to biological principles, complications following rotator cuff repair remain a significant clinical challenge. The most common complication is structural failure, or retear, which correlates directly with initial tear size, patient age, and the degree of preoperative fatty infiltration. Retear rates vary widely in the literature, ranging from 10% for small tears to as high as 40-90% for massive, multi-tendon tears. However, it is critical to distinguish between structural failure and clinical failure; many patients with imaging-confirmed retears maintain excellent pain relief and functional improvement, provided the force couples and rotator cable biomechanics were partially restored.
Postoperative stiffness, often secondary to adhesive capsulitis or over-tensioning of the repair, is another frequent complication, occurring in up to 15% of patients. It is more common in partial-thickness repairs, concomitant labral repairs, and patients with metabolic conditions such as diabetes. Most cases resolve with aggressive, phased physical therapy and time, though refractory cases may require arthroscopic capsular release after biological healing of the cuff is assured (typically after 6 to 9 months). Infection, particularly indolent infections caused by Cutibacterium acnes (formerly Propionibacterium acnes), presents a unique diagnostic challenge. C. acnes is a slow-growing anaerobe native to the sebaceous glands of the shoulder. Infections may present months postoperatively with subtle stiffness and vague pain rather than overt erythema or systemic signs.
When a primary repair fails clinically, salvage management must be tailored to the patient's specific pathoanatomy. In younger patients with intact cartilage and an irreparable posterosuperior tear, Superior Capsular Reconstruction (SCR) utilizing a thick dermal allograft or fascia lata autograft can restore the superior restraint to the humeral head. Alternatively, lower trapezius or latissimus dorsi tendon transfers can actively restore external rotation and elevation. In older patients, or those with concomitant glenohumeral arthritis (Cuff Tear Arthropathy), Reverse Total Shoulder Arthroplasty (RTSA) is the definitive salvage procedure, providing reliable pain relief and functional restoration by medializing and distalizing the center of rotation, thereby recruiting the deltoid to compensate for the deficient rotator cuff.
Complications and Salvage Strategies Matrix
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Management / Salvage Strategy |
|---|---|---|---|
| Structural Retear | 10% (Small) to >50% (Massive) | High tension, poor biology, advanced age, non-compliance with rehab. | If asymptomatic: Observe. If symptomatic: Revision repair, SCR, Tendon Transfer, or RTSA. |
| Postoperative Stiffness | 5% - 15% | Adhesive capsulitis, over-tensioning, prolonged immobilization, diabetes. | Aggressive PT, oral corticosteroids. Arthroscopic capsular release if refractory >6-9 months. |
| Infection (C. acnes) | 0.5% - 1.5% | Anaerobic colonization of dermal sebaceous glands. Male gender. | Arthroscopic irrigation and debridement, anchor retention/removal based on fixation, IV antibiotics. |
| Nerve Injury | < 1% | Traction neurapraxia (lateral decubitus) or direct injury to axillary/suprascapular nerve. | Observation and EMG at 3 months. Most traction injuries resolve spontaneously. |
| Anchor Pullout / Osteolysis | 1% - 3% | Poor bone stock (osteopenia), aggressive decortication, improper anchor angle. | Revision fixation with larger anchors or medialization. Bone grafting if severe cysts present. |
Phased Post-Operative Rehabilitation Protocols
Successful biological healing of a rotator cuff repair is heavily dependent on strict adherence to a phased, biologically sound postoperative rehabilitation protocol. The surgeon's technical perfection in the operating room can be easily unraveled by premature or aggressive physical therapy. The enthesis requires a minimum of 12 to 16 weeks for Sharpey's fibers to bridge the tendon-bone interface and mature sufficiently to withstand physiological loads. Therefore, rehabilitation must balance the competing interests of protecting the fragile repair and preventing debilitating postoperative stiffness.
Phase I: Maximum Protection (Weeks 0-6)
The primary goal of Phase I is to protect the surgical construct while allowing for early biological healing. The patient is placed in an abduction sling (typically 15 to 30 degrees of abduction) to remove tension from the superior cuff, particularly the supraspinatus. Range of motion (ROM) is strictly passive. Depending on the tear size and repair tension, patients begin pendulum exercises and passive forward elevation and external rotation within safe limits determined intraoperatively by the surgeon. Active motion of the elbow, wrist, and hand is encouraged to prevent distal edema and stiffness. There is an absolute restriction on active shoulder motion, lifting, and sudden reactive movements.
Phase II: Active-Assisted to Active Motion (Weeks 6-12)
As the initial fibrovascular scar tissue forms, the protocol transitions to Phase II. The abduction sling is gradually weaned and discontinued, typically around the 6-week mark. Range of motion exercises transition from passive to active-assisted, utilizing pulleys, wand exercises, and wall-crawls, eventually progressing to full active ROM in all planes. Submaximal, pain-free isometric exercises for the deltoid and the intact rotator cuff muscles are initiated to reverse disuse atrophy. Scapulothoracic mobilization is critical during this phase to correct compensatory dyskinesia and ensure a stable base for glenohumeral kinematics.
Phase III: Strengthening and Early Function (Weeks 12-24)
At 12 weeks, the tendon-to-bone interface has achieved sufficient mechanical strength to tolerate isotonic loading. Phase III focuses on progressive isotonic strengthening using resistance bands and light free weights. The emphasis is placed on high-repetition, low-weight exercises to build endurance in the rotator cuff and scapular stabilizers. Restoring the anterior-posterior and superior-inferior force couples is the primary biomechanical objective. Patients may begin to perform light activities of daily living below shoulder level, but heavy lifting and overhead loading remain restricted.
Phase IV: Return to Advanced Function and Sport (Months 6+)
The final phase of rehabilitation is tailored to the patient's specific functional goals, whether that involves returning to manual labor, overhead sports, or normal daily activities. Advanced plyometric exercises, sport-specific drills, and heavy resistance training are integrated. A clinical evaluation of strength, functional mechanics, and dynamic stability is required before clearing the patient for full, unrestricted activity. It is imperative to educate the patient that maximal biological remodeling and functional recovery can take up to 12 to 18 months postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The evidence-based practice of rotator cuff repair is built upon a foundation of landmark clinical and biomechanical studies. Galatz et al. provided a sobering assessment of early arthroscopic repairs, demonstrating high retear rates in large tears and highlighting the biomechanical inadequacies of single-row, non-compressive constructs. This catalyzed a paradigm shift in anchor design and suture configuration. Subsequently, Boileau et al. and Sugaya et al. published seminal works demonstrating that modern arthroscopic techniques, particularly those emphasizing footprint restoration and biological augmentation, yield reliable healing and excellent functional outcomes that rival or exceed open techniques.
The biomechanical superiority of the transosseous-equivalent (TOE) suture-bridge technique was definitively established by researchers such as Meier and Mazzocca, who demonstrated that maximizing the pressurized contact area at the tendon-bone interface significantly enhances load-to-failure strength and minimizes gap formation under cyclic loading. Clinically, Burkhart's conceptualization of the "rotator cable" and the principle of "margin convergence" revolutionized the approach to massive, retracted tears, providing surgeons with a reproducible algorithm to reduce tension and restore force couples without over-stressing the degenerative tendon edge.
From a clinical guideline perspective, the American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines for the Management of Rotator Cuff Injuries advocate for surgical repair in active patients with acute, traumatic tears, and recommend a trial of conservative management for chronic, degenerative tears. The guidelines also strongly support the use of MRI for accurate preoperative templating and emphasize the necessity of structured, phased postoperative rehabilitation. Mastery of this literature is essential for the academic orthopedic surgeon, ensuring that operative decision-making remains grounded in rigorous, peer-reviewed science rather than anecdotal experience.
