Subscapularis Tears: Mastering the Optimal Angle of Approach

Key Takeaway
This article provides essential research regarding Subscapularis Tears: Mastering the Optimal Angle of Approach. A subscapularis tendon tear typically occurs at its insertion into the lesser tuberosity of the proximal humerus. Often overlooked, these tears are caused by intrinsic factors or extrinsic mechanical factors like subcoracoid impingement. Proper evaluation, considering the optimal angle of approach, is paramount for diagnosis and treatment to restore functional shoulder stability.
Comprehensive Introduction and Patho-Epidemiology
The subscapularis muscle is the largest and most powerful of the rotator cuff muscles, providing more than fifty percent of the total cuff strength. Historically, it has been referred to as the "forgotten tendon" because tears of the subscapularis were frequently overlooked, underdiagnosed, and consequently undertreated. A subscapularis tendon tear typically occurs at its insertion into the lesser tuberosity of the proximal humerus. With the advent of advanced arthroscopic techniques and improved magnetic resonance imaging (MRI), the true prevalence of subscapularis pathology has been increasingly recognized. It is now understood that subscapularis tendon tears are a critical source of anterior shoulder pain and profound functional disability, necessitating a high index of suspicion during clinical evaluation. Proper evaluation of the shoulder is of paramount importance, as timely and anatomically accurate treatment of subscapularis tendon tears can predictably restore the functional stability of the glenohumeral joint.
The pathogenesis of subscapularis tears is multifactorial, involving both intrinsic degenerative processes and extrinsic mechanical factors. Intrinsic factors include age-related microvascular compromise, localized tendon hypoxia, and progressive collagen degeneration, which collectively weaken the tendon insertion. Extrinsic mechanical factors, however, play a highly specific and critical role in anterior cuff failure. The normal subcoracoid space—also known as the coracohumeral interval—represents the distance from the coracoid tip to the lesser tuberosity of the proximal humerus. Anatomic and imaging studies have defined the normal coracohumeral interval to be between 8.4 and 11 mm. When this space becomes stenotic, the coracoid process acts as a mechanical abutment against the subscapularis tendon during internal rotation and forward elevation.
Subcoracoid stenosis is strictly defined as less than 6 mm of space between the coracoid and the proximal humerus, measurable via MRI or dynamic arthroscopy. Patients with documented subscapularis tears often exhibit a significantly reduced coracohumeral interval, averaging 5 mm compared to 10 mm in matched cohorts without subscapularis pathology. This mechanical impingement creates the "roller-wringer effect." In subcoracoid impingement, the prominent coracoid tip indents the superficial surface of the subscapularis tendon. This indentation generates immense tensile forces on the convex, articular (under) surface of the tendon, leading to progressive fiber failure. Cadaveric studies corroborate that subscapularis tendon tears frequently initiate as partial-thickness articular-sided tears at the most superior aspect of the insertion, particularly in the elderly population.
The natural history of untreated subscapularis tendon tears is characterized by progressive medial retraction, extensive fatty infiltration, and inexorable functional decline. Complete tears of the subscapularis tendon often result in severe medial retraction of the tendon edge to the level of the anterior glenoid rim. This retraction disrupts the intricate balance of the glenohumeral force couples, leading to obligate anterosuperior humeral head translation. In patients with massive rotator cuff tears involving the subscapularis, the loss of this anterior restraint can be profoundly disabling. Many of these patients suffer from pseudoparalysis and never regain functional overhead use of their upper extremities without meticulous surgical intervention. Even in cases of chronic tears with significant muscle atrophy, repair is often advocated because the subscapularis may still provide a vital tenodesis effect, acting as an anterior buttress to stabilize the humeral fulcrum.
Detailed Surgical Anatomy and Biomechanics
The subscapularis muscle originates from the medial two-thirds of the anterior scapular fossa, forming a robust, multipennate muscle belly. The muscle courses laterally beneath the coracoid process and transitions into a dense, tendinous structure at the level of the anterior glenoid rim. The subscapularis tendon becomes intimately confluent with the anterior glenohumeral joint capsule deep to it before inserting into the lesser tuberosity of the proximal humerus. The normal subscapularis tendon not only intermingles with the capsular fibers but also blends seamlessly at its superior insertion with the fibers of the medial sling of the long head of the biceps tendon. This medial sling is a complex retinacular structure composed of fibers from the superior glenohumeral ligament (SGHL) and the coracohumeral ligament (CHL) complex.
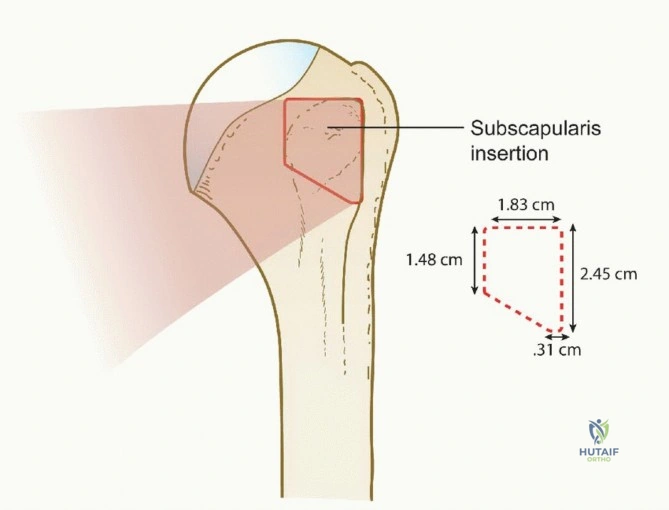
The footprint of the subscapularis tendon insertion on the lesser tuberosity is approximately 2.5 cm long (ranging from 1.5 to 3.0 cm) and is distinctly trapezoidal. The widest and thickest portion of the insertion is located at its most superior (cephalad) aspect, tapering inferiorly. This unique geometric configuration closely resembles the shape of the state of Nevada. Biomechanically, the superior aspect is the strongest and most critical part of the subscapularis insertion, bearing the brunt of the tensile loads during active internal rotation. The subscapularis muscle is dually innervated by the upper and lower subscapular nerves, which branch from the posterior cord of the brachial plexus. Its primary blood supply is derived from the subscapular artery, with rich anastomotic networks supplying the muscle belly, though the tendinous insertion remains relatively hypovascular, predisposing it to degenerative failure.
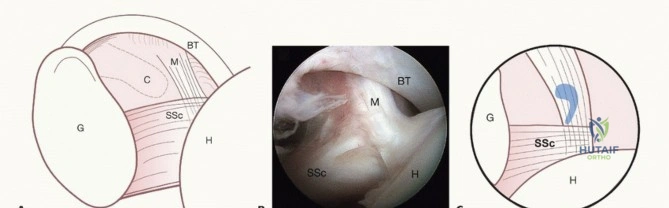
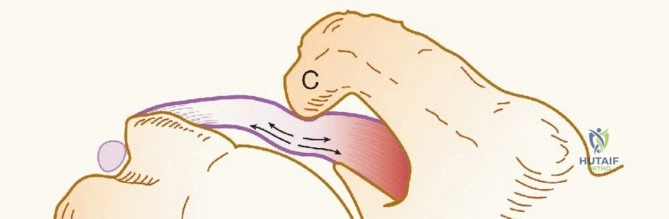
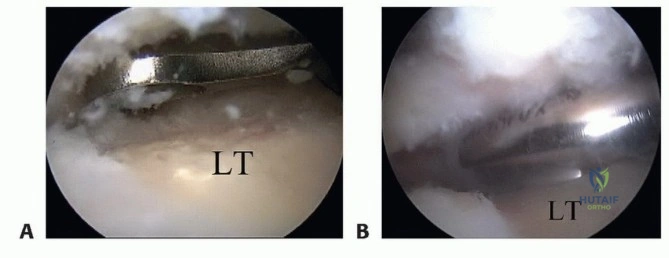
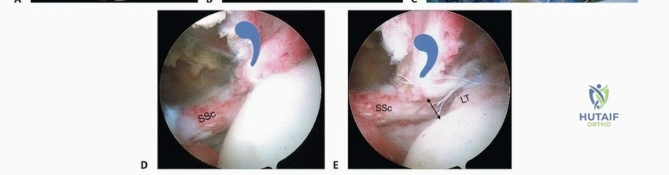
A hallmark of subscapularis anatomy, crucial for the arthroscopic surgeon, is the "comma sign." When a complete tear of the subscapularis tendon occurs, the tendon edge retracts medially. In doing so, it pulls the adjacent medial sling of the biceps tendon (composed of the SGHL and CHL) along with it. The fibers of this medial sling are oriented approximately perpendicular to the horizontal fibers of the subscapularis tendon. Arthroscopically, this retracted tissue complex forms a distinct, comma-shaped soft tissue structure. Recognizing the comma sign is an invaluable navigational tool; tracing the comma laterally and inferiorly reliably leads the surgeon directly to the superolateral edge of the retracted subscapularis tendon, even when it is obscured by dense bursal scarring or capsular adhesions.
Biomechanically, the main functions of the subscapularis muscle are to internally rotate and adduct the humerus, while providing a dynamic anterior restraint to humeral head translation. More importantly, the subscapularis acts in concert with the posterior rotator cuff muscles (infraspinatus and teres minor) to balance the transverse-plane force couple. Simultaneously, it works with the deltoid to balance the coronal-plane force couple. This dynamic stabilization is essential to centralize the humeral head on the glenoid—often conceptualized as "maintaining the golf ball on the golf tee." This centralized compression provides a stable, fixed fulcrum for normal glenohumeral arthrokinematics. Loss of the subscapularis tendon disrupts this fulcrum, leading to abnormal kinematics, anterior subluxation, and accelerated degenerative joint disease.
Exhaustive Indications and Contraindications
The clinical presentation of a subscapularis tear demands a meticulous history and an exhaustive physical examination. While most subscapularis tears in the community are degenerative, the classic scenario for a traumatic tear involves a violent, forced external rotation mechanism. This eccentric tensile load is particularly devastating to a tendon already "at risk" due to subcoracoid stenosis. Unlike patients with isolated posterosuperior rotator cuff tears who primarily struggle with overhead elevation, patients with subscapularis tears report profound weakness and pain during activities of daily living performed in front of the body and below the shoulder level (e.g., tucking in a shirt, opening a heavy door, or washing the contralateral axilla).
Physical examination must include specific provocative maneuvers to isolate subscapularis function. The Lift-off test is positive when the patient cannot actively hold the dorsum of their hand away from the lumbar spine; crucially, this test typically only becomes positive when at least 75% of the inferior subscapularis tendon is torn. Because many patients lack the internal rotation necessary to reach the lumbar spine, the Napoleon test (modified belly press) is essential. A positive Napoleon test—where the patient must flex the wrist to 90 degrees and drop the elbow posteriorly to press on the belly—indicates a complete tendon tear. An intermediate test (wrist flexed 30 to 60 degrees) suggests that more than 50% of the tendon is torn. A negative test occurs when the patient can "strike the pose" with a straight wrist, indicating less than 50% tearing. The Bear hug test is the most sensitive maneuver for detecting upper subscapularis injuries (partial superior tears); a positive test occurs when the examiner can easily pull the patient's hand off the contralateral shoulder.
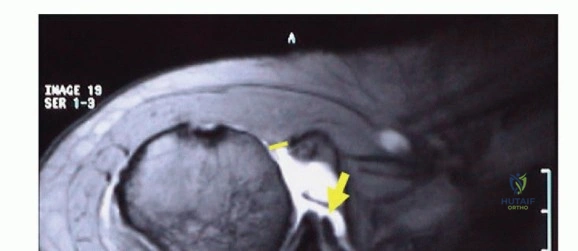
Diagnostic imaging is a cornerstone of preoperative planning. A standard radiographic series must include five views: anteroposterior (AP) internal rotation, AP external rotation, AP with 30-degree caudal tilt, a supraspinatus outlet view, and a true axillary view. The axillary view is particularly critical for assessing static anterior humeral translation, which is pathognomonic for massive subscapularis failure. MRI is the gold standard for evaluating the extent of the tear, the degree of medial retraction, and the presence of muscle atrophy and fatty infiltration (Goutallier classification). Tears are best appreciated on axial and sagittal oblique sequences. Furthermore, MRI allows for precise measurement of the coracohumeral interval to confirm subcoracoid stenosis.

| Clinical Scenario | Operative Indications | Absolute Contraindications |
|---|---|---|
| Acute Traumatic Tears | Any full-thickness tear in an active patient; partial tears >50% depth failing conservative care. | Medically unstable patient; active local or systemic infection. |
| Chronic Degenerative Tears | Persistent pain/weakness >3-6 months; progressive fatty infiltration (Goutallier 1-2). | Advanced cuff tear arthropathy (Hamada Grade 4-5); fixed superior migration. |
| Concomitant Pathology | Biceps subluxation/dislocation; massive multi-tendon cuff tears requiring anterior force couple restoration. | Severe fatty infiltration (Goutallier 3-4) of the subscapularis muscle belly. |
| Subcoracoid Impingement | Coracohumeral interval <6mm with symptomatic partial/full articular-sided tears. | Deltoid paralysis or severe axillary neuropathy. |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for arthroscopic subscapularis repair requires a comprehensive synthesis of the patient's history, physical examination, and advanced imaging. The surgeon must template the anticipated anchor trajectory, evaluate the bone stock of the lesser tuberosity, and determine the necessity of a concomitant coracoplasty. If the MRI demonstrates a coracohumeral interval of less than 6 mm accompanied by a "kissing lesion" on the lesser tuberosity, an arthroscopic coracoplasty must be incorporated into the surgical plan to prevent postoperative mechanical failure of the repair. Furthermore, the status of the long head of the biceps tendon must be scrutinized; a disrupted medial sling almost invariably leads to biceps instability, necessitating a biceps tenodesis or tenotomy.
On the day of surgery, the anesthesiologist typically administers general anesthesia with endotracheal intubation, often supplemented by an interscalene regional block to optimize postoperative pain control. Protective eyewear is applied to the patient to prevent inadvertent ocular injury during positioning and instrument passing. While some surgeons prefer the beach-chair position, the lateral decubitus position offers distinct advantages for subscapularis repair, including superior visualization of the anterior compartment and the ability to apply controlled traction to open the subcoracoid space. The patient is carefully rotated into the lateral decubitus position, and a well-padded axillary roll is placed to protect the dependent brachial plexus.

The patient's torso is secured in place using a rigid vacuum beanbag, and the table is tilted backward approximately 20 to 30 degrees to orient the glenoid parallel to the floor. All bony prominences, particularly the fibular head and greater trochanter, are meticulously padded with pillows beneath and between the legs. A forced-air warming blanket is applied to the lower body to prevent intraoperative hypothermia. The sterile field must be expansive, extending posteriorly to a position medial to the scapula and anteriorly just lateral to the nipple line, allowing unrestricted access for accessory anterior portals.

After the patient is properly protected, positioned, padded, and draped, the surgeon performs a thorough examination under anesthesia (EUA) to assess passive range of motion and glenohumeral translation. The surgical assistant then prepares the operative extremity with a standard sterile scrub. The arm is placed into a sterile traction sleeve and suspended with 5 to 10 pounds of balanced traction (e.g., STaR Sleeve Traction System). The spatial orientation of the arm is critical: the shoulder is positioned in 20 to 30 degrees of abduction and 20 degrees of forward flexion. This specific vector maximizes the working space within the anterior glenohumeral joint and relaxes the anterior capsule, facilitating mobilization of the retracted subscapularis tendon.
Step-by-Step Surgical Approach and Fixation Technique
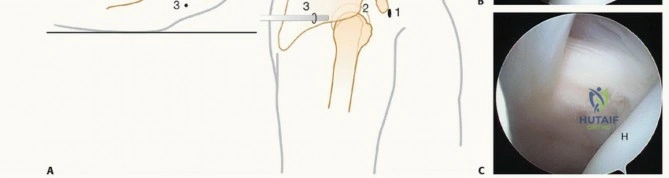
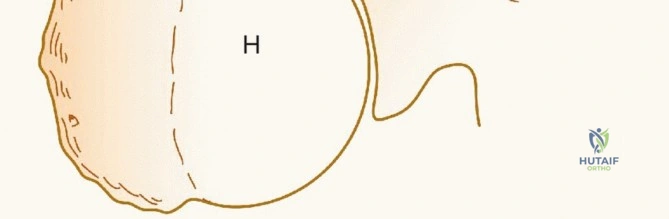
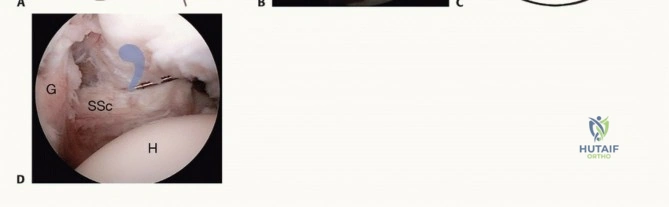
Successful arthroscopic treatment of subscapularis tears hinges on meticulous portal placement. The surgeon must adhere to the "6 Ps" for arthroscopic portals: "Proper portal placement prevents poor performance." The standard posterior viewing portal is established first, typically 2 cm inferior and 1 cm medial to the posterolateral acromial edge. Upon entering the joint, a comprehensive diagnostic arthroscopy is performed. The surgeon evaluates the articular cartilage, the labrum, and the posterosuperior rotator cuff. Attention is then directed anteriorly. In the setting of a complete subscapularis tear, the footprint on the lesser tuberosity will be bare, and the tendon will be retracted medially.

The anterior working portals are established under direct intra-articular visualization using a spinal needle. An anterosuperior portal is created high in the rotator interval, just anterior to the leading edge of the supraspinatus, serving as the primary viewing portal for the subscapularis footprint. An anteroinferior (or mid-anterior) portal is established just superior to the upper border of the subscapularis tendon, serving as the primary working portal. The first critical step in the repair is identifying the "comma sign." By tracing the comma-shaped tissue complex of the displaced medial sling, the surgeon locates the superolateral edge of the retracted subscapularis tendon.

Once identified, the tendon must be mobilized. Extensive releases are often required for chronic, retracted tears. The surgeon must perform a complete anterior, superior, and posterior capsular release. The coracohumeral ligament is transected, and adhesions between the subscapularis and the base of the coracoid are meticulously lysed using an electrocautery device or a radiofrequency wand. During the inferior mobilization, the surgeon must remain acutely aware of the axillary nerve, which runs intimately close to the inferior border of the subscapularis muscle belly. A successful release is achieved when the tendon edge can be effortlessly reduced to the lateral margin of the lesser tuberosity footprint.

If subcoracoid stenosis is present, a coracoplasty is performed prior to tendon fixation. Using a motorized burr through the anteroinferior portal, the posterolateral aspect of the coracoid tip is resected until at least 7 mm of clearance is achieved between the coracoid and the subscapularis tendon during dynamic internal rotation. Following coracoplasty, the lesser tuberosity footprint is prepared. The cortical surface is lightly decorticated with a burr or shaver to create a bleeding bone bed, optimizing the biologic environment for tendon-to-bone healing, while preserving the underlying cancellous architecture for robust anchor purchase.
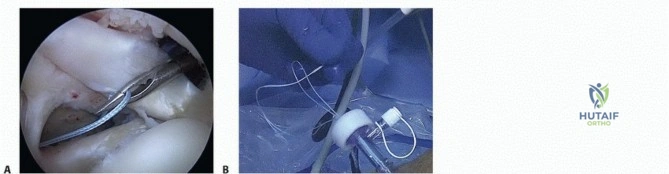
Both knotless and knotted anchor technologies have demonstrated excellent biomechanical and clinical outcomes. In general, a knotless technique is preferred for partial articular-sided tears and nonretracted full-thickness tears, as it minimizes subcoracoid impingement from bulky suture knots. For chronically retracted, high-tension tears, a knotted technique utilizing double-loaded suture anchors may be required to ensure secure tissue approximation. Anchors are placed at the medial margin of the footprint. Suture passing is accomplished using penetrating graspers or a spectrum lasso device, ensuring that large, full-thickness bites of the tendon are captured. The sutures are then tied or secured with knotless lateral row anchors, compressing the tendon firmly against the decorticated footprint. Finally, given the high incidence of medial sling disruption, a concomitant biceps tenodesis is routinely performed to eliminate the LHB as a source of persistent anterior pain.



Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, arthroscopic subscapularis repair carries a distinct profile of intraoperative and postoperative complications. The most devastating intraoperative complication is iatrogenic nerve injury. The axillary nerve, located mere millimeters from the inferior border of the subscapularis, is at extreme risk during aggressive inferior capsular releases and thermal ablation. Similarly
Clinical & Radiographic Imaging Archive