Open Repair of Rotator Cuff Tears: A Masterclass in Surgical Techniques
Key Takeaway
Open repair of rotator cuff tears remains a foundational technique for managing massive, retracted, or complex tear patterns. This procedure demands meticulous tendon mobilization, precise biomechanical restoration using double-row or transosseous equivalent techniques, and careful preservation of the deltoid origin. Successful outcomes rely on achieving a tension-free, biologically robust tendon-to-bone footprint while adhering to strictly staged postoperative rehabilitation protocols to optimize tissue healing and functional recovery.
Comprehensive Introduction and Patho-Epidemiology
While the advent and refinement of arthroscopic techniques have established a new gold standard for the management of many rotator cuff pathologies, the open repair of rotator cuff tears remains an indispensable and highly relevant procedure in the armamentarium of the modern orthopaedic surgeon. The open approach is particularly indicated for massive, chronically retracted tears, complex revision surgeries, and cases requiring intricate tendon transfers or biologic augmentation where arthroscopic visualization and manipulation may be biomechanically or technically prohibitive. The mastery of open rotator cuff surgery requires a profound understanding of three-dimensional shoulder anatomy, the biological limitations of degenerated tendon tissue, and the biomechanical principles governing the restoration of the glenohumeral force couples.
Understanding the pathoanatomy of the torn rotator cuff is paramount to executing a successful repair. Most rotator cuff tears are not simply transverse avulsions from the greater tuberosity; they possess a significant longitudinal component, rendering their geometry oval, U-shaped, L-shaped, or triangular. Consequently, all but the smallest and most acute of tears require extensive, multidirectional mobilization. The tendon must be advanced both anteriorly and laterally—not merely laterally—to restore the anatomical footprint and correct the resting length of the muscle-tendon unit. In tears exceeding 2 to 3 cm in diameter, the infraspinatus tendon is almost invariably involved, necessitating a comprehensive approach to both the superior and posterior aspects of the rotator cuff to achieve a watertight and biomechanically sound reconstruction.
The epidemiology of rotator cuff disease demonstrates a clear age-dependent progression, highlighting the degenerative nature of the condition. While acute traumatic tears do occur, particularly in younger patients following high-energy trauma or shoulder dislocations, the vast majority of rotator cuff tears are the culmination of chronic, progressive intrinsic tendon degeneration coupled with extrinsic mechanical impingement. As the tear propagates, the involved muscle bellies undergo predictable pathophysiological changes, most notably muscle atrophy and fatty infiltration. These changes, initially described and classified by Goutallier, are often irreversible and directly dictate the biological healing potential of the repaired tendon. A thorough appreciation of this patho-epidemiology is essential for setting realistic surgical goals and managing patient expectations.
Furthermore, the chronicity of the tear dictates the degree of tendon retraction and the formation of dense, intra-articular and extra-articular adhesions. The longer a tear remains untreated, the more the muscle-tendon unit retracts medially, leading to a contracted state that severely complicates anatomical reduction. The surrounding bursa becomes hypertrophic and fibrotic, obscuring normal anatomical landmarks and creating a hostile environment for tendon excursion. The surgeon must therefore approach an open rotator cuff repair not merely as a localized suturing exercise, but as a comprehensive structural and biological rehabilitation of the entire shoulder girdle, addressing capsular contractures, bursal pathology, and bony impingement simultaneously.
Detailed Surgical Anatomy and Biomechanics
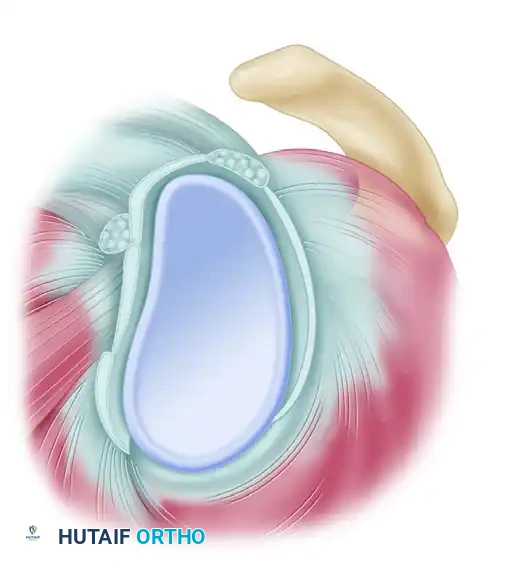
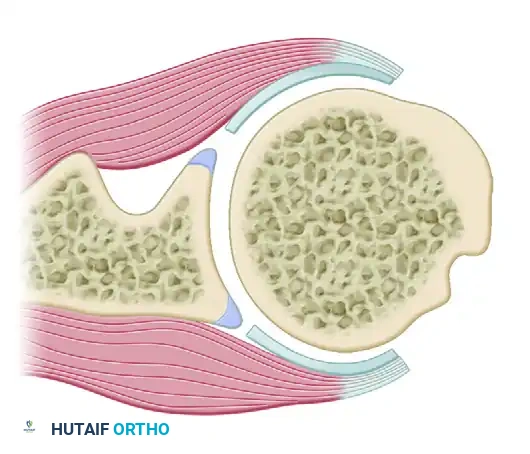
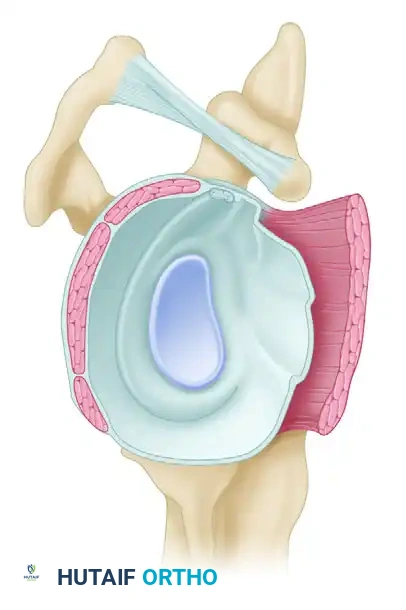
A profound mastery of the surgical anatomy of the rotator cuff and its associated neurovascular structures is the foundation upon which successful open repairs are built. The rotator cuff comprises four distinct muscle-tendon units—the supraspinatus, infraspinatus, teres minor, and subscapularis—that coalesce to form a continuous tendinous hood around the humeral head. Recent anatomical studies have redefined our understanding of the rotator cuff footprint. Contrary to historical teachings that assigned a large, rectangular insertion to the supraspinatus, modern cadaveric analyses reveal that the supraspinatus footprint is relatively small and triangular, inserting primarily on the anteromedial aspect of the greater tuberosity. The infraspinatus, conversely, possesses a much larger, trapezoidal insertion that extends far anteriorly, occupying a significant portion of the greater tuberosity previously attributed to the supraspinatus.
The biomechanical concept of the "rotator cable" and "rotator crescent," popularized by Burkhart, is critical for understanding tear propagation and repair strategies. The rotator cable is a thick, fibrous band of tissue extending from the coracohumeral ligament anteriorly to the inferior margin of the infraspinatus posteriorly, functioning much like the suspension cable of a bridge. It spans the relatively thinner, avascular tissue of the rotator crescent, which inserts directly onto the greater tuberosity. Tears that remain confined within the crescent may be biomechanically stable and minimally symptomatic, whereas tears that disrupt the rotator cable lead to catastrophic failure of the suspension system, resulting in rapid tear propagation, massive retraction, and significant functional impairment. Repairing or reconstituting this cable is a primary objective of the surgical intervention.
Restoration of the glenohumeral force couples is the ultimate biomechanical goal of rotator cuff surgery. The shoulder joint relies on dynamic stabilization, orchestrated by two primary force couples. In the coronal plane, the inferiorly directed pull of the intact rotator cuff balances the superiorly directed shear force of the deltoid muscle. When the supraspinatus and infraspinatus fail, the deltoid's unopposed upward pull leads to superior migration of the humeral head, clinically manifesting as a decreased acromiohumeral interval and eventual cuff tear arthropathy. In the transverse plane, the anterior force of the subscapularis must be perfectly balanced by the posterior force of the infraspinatus and teres minor. A successful open repair must meticulously restore both force couples to recenter the humeral head within the glenoid fossa, thereby optimizing the mechanical advantage of the deltoid and restoring active elevation.
Navigating the neurovascular anatomy during open repair is fraught with potential hazards. The axillary nerve, which innervates the deltoid and teres minor, courses intimately close to the surgical field. It exits the axilla through the quadrangular space and winds around the surgical neck of the humerus, lying approximately 5 cm distal to the lateral border of the acromion. This anatomical constant dictates the "safe zone" for the deltoid-splitting approach. Similarly, the suprascapular nerve, responsible for innervating the supraspinatus and infraspinatus, is at risk during aggressive medial, posterior, or inferior mobilization. It courses through the suprascapular notch, supplies the supraspinatus, and then sharply descends through the spinoglenoid notch to supply the infraspinatus. Excessive medial traction on a retracted tendon or blind dissection near the glenoid neck can result in catastrophic iatrogenic denervation of the very muscles the surgeon is attempting to salvage.
Exhaustive Indications and Contraindications
The decision to proceed with an open rotator cuff repair, as opposed to an arthroscopic or non-operative approach, requires a nuanced evaluation of the patient's pathology, physiological age, functional demands, and the surgeon's technical expertise. Open repair is classically indicated for massive, chronically retracted tears (typically involving two or more tendons or exceeding 5 cm in diameter) where the sheer mechanical force required to mobilize and reduce the tendon to the footprint exceeds the capabilities of arthroscopic instruments. Furthermore, in the setting of revision surgery, where normal tissue planes have been obliterated by scar tissue and previous hardware may need to be localized and removed, the superior tactile feedback and direct visualization afforded by an open approach are invaluable.
Concomitant procedures often tip the scales in favor of an open approach. When a massive, irreparable posterosuperior rotator cuff tear necessitates a tendon transfer—such as a latissimus dorsi or lower trapezius transfer—an open or mini-open approach is inherently required to route the transferred tendon and secure it to the greater tuberosity. Similarly, cases requiring robust biologic augmentation with thick extracellular matrix scaffolds or allografts may be more efficiently and securely managed through an open incision, ensuring precise tensioning and incorporation of the graft into the host tissue without the spatial constraints of arthroscopic cannulas.
Conversely, strict contraindications exist that must prevent the surgeon from attempting an anatomical repair. The most absolute contraindication is the presence of advanced rotator cuff tear arthropathy, characterized by severe superior migration of the humeral head, femoralization of the greater tuberosity, and acetabularization of the coracoacromial arch (Hamada Grade 3 or higher). In such scenarios, attempting to repair the tendon is an exercise in futility; the altered joint mechanics and severely degenerated tissue guarantee failure, and a reverse total shoulder arthroplasty is the appropriate surgical intervention. Additionally, an active glenohumeral or subacromial infection absolutely precludes any reconstructive effort until the infection is definitively eradicated.
Relative contraindications revolve around the biological quality of the muscle and the patient's physiological status. Severe fatty infiltration (Goutallier Stage 3 or 4), where intramuscular fat exceeds functional muscle tissue, indicates irreversible muscle degeneration. Even if a technically perfect structural repair is achieved, the muscle will not generate sufficient contractile force to restore function, and the repair is highly likely to fail biologically. Furthermore, profound deltoid dysfunction—whether due to previous iatrogenic axillary nerve injury or primary neurological disease—is a strong contraindication, as the deltoid is the primary motor unit of the shoulder; without it, repairing the rotator cuff will not restore active elevation.
| Category | Indications for Open Repair | Contraindications for Open Repair |
|---|---|---|
| Tear Characteristics | Massive, chronically retracted tears (>5cm); Multi-tendon involvement requiring extensive mobilization. | Advanced Cuff Tear Arthropathy (Hamada Grade 3+); Fixed superior humeral head migration. |
| Surgical History | Complex revision surgeries; Hardware removal from previous failed repairs; Obliterated tissue planes. | Active subacromial or glenohumeral joint infection; Active osteomyelitis of the proximal humerus. |
| Muscle Biology | Goutallier Stage 0-2 (viable muscle belly capable of contraction post-repair). | Goutallier Stage 3-4 (severe fatty infiltration); Muscle atrophy (Thomazeau Grade III). |
| Concomitant Procedures | Requirement for structural tendon transfers (Latissimus Dorsi, Lower Trapezius); Thick biologic scaffold augmentation. | Deltoid paralysis or severe dysfunction (axillary nerve palsy); Inability to comply with strict post-op rehab. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the crucible in which successful surgical outcomes are forged. The clinical evaluation must go beyond merely diagnosing a tear; it must assess the functional deficit and the integrity of the remaining shoulder structures. Specific clinical tests, such as the external rotation lag sign and the Hornblower's sign, are critical for assessing the viability of the infraspinatus and teres minor, respectively. A positive lag sign often indicates significant fatty infiltration or massive retraction, warning the surgeon of a potentially irreparable situation. Similarly, the belly-press and bear-hug tests evaluate the subscapularis, ensuring that anterior extension of the tear is identified and addressed during the surgical exposure.
Advanced imaging is non-negotiable in the preoperative assessment of open rotator cuff repairs. High-resolution Magnetic Resonance Imaging (MRI) without contrast is the modality of choice. The surgeon must systematically evaluate the sagittal oblique T1-weighted sequences to grade the degree of fatty infiltration using the Goutallier classification, as this directly informs the biological prognosis. The coronal oblique T2-weighted sequences are utilized to measure the amount of medial tendon retraction (Patte classification) and to assess the acromiohumeral interval. Additionally, a standard radiographic series, including a true anteroposterior (Grashey), scapular Y, and axillary lateral view, is essential to evaluate acromial morphology (Biggliani classification), identify os acromiale, and rule out subtle glenohumeral arthritis or superior humeral head migration.
Patient positioning is a critical step that dictates surgical exposure, ease of mobilization, and overall operative efficiency. For open rotator cuff repairs, the modified beach chair position is overwhelmingly preferred. The patient is positioned with the backrest elevated to approximately 45 to 60 degrees, with the hips and knees slightly flexed to prevent sciatic nerve stretch and venous pooling. The operative shoulder must be translated laterally off the edge of the table to allow unrestricted extension and internal rotation of the arm, which is vital for exposing the posterior aspect of the greater tuberosity. The head must be securely immobilized in a neutral position using a dedicated headrest to prevent catastrophic cervical spine hyperextension or lateral flexion injuries during the procedure.
Draping and intraoperative arm management require careful attention. A wide sterile field must be established, extending from the base of the neck to the sternal notch medially, and down to the costal margin inferiorly, allowing for potential extension of the incision if a tendon transfer becomes necessary. The use of a mechanical limb positioner (such as a Spider or TRIMANO arm) is highly recommended. These devices allow the surgeon to seamlessly transition the arm through various degrees of abduction, forward flexion, and rotation, dynamically altering the tension on the rotator cuff tendons during mobilization and footprint preparation. Precise control of the arm position is particularly crucial during the knot-tying phase of a double-row repair to ensure the tendon is secured under minimal tension.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approach and Deltoid Management
The standard approach for an open rotator cuff repair is the anterolateral deltoid-splitting approach. The skin incision is typically centered over the anterolateral corner of the acromion, extending distally for approximately 4 to 5 cm. Meticulous care must be taken to identify the raphe between the anterior and middle heads of the deltoid. The split is developed bluntly, strictly adhering to the 5 cm rule to preserve the deltoid origin and protect the axillary nerve, which courses transversely beneath the muscle belly.
Surgical Warning: Compromise of the deltoid origin or iatrogenic injury to the axillary nerve transforms a potentially successful rotator cuff repair into a catastrophic functional failure. Always maintain a strict "safe zone" during deltoid splitting. A heavy stay suture should be placed at the distal apex of the deltoid split to physically prevent inadvertent distal propagation of the dissection.
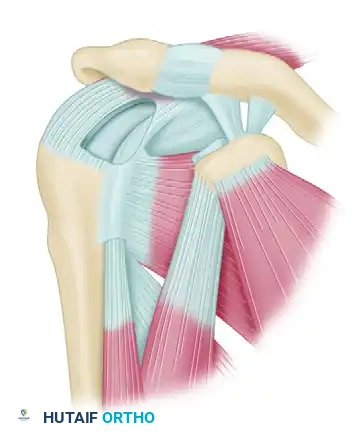
Once the subacromial space is accessed, a thorough and aggressive bursectomy is performed. The hypertrophic, inflamed subacromial bursa often completely obscures the underlying rotator cuff pathology. Using electrocautery and blunt dissection, the bursa is excised to clearly delineate the tear geometry, the coracoacromial ligament, and the borders of the remaining intact cuff. When the defect has been identified and its size approximated, attention is turned to the repair itself. In chronic tears, the tendon edges are often scarred, retracted, and adherent to surrounding structures, making mobilization the most critical phase of the operation.
Tendon Mobilization Techniques
Adequate mobilization is the absolute cornerstone of a tension-free repair. Excessive tension at the repair site is the most common mechanical mechanism of failure, typically resulting in the suture cutting through the degenerated tendon substance (cheese-wiring) in the early postoperative period.
Posterior Mobilization
Begin mobilization posteriorly with the infraspinatus. Using a blunt probe, a Cobb elevator, or a gloved finger, systematically release adhesions both inside and outside the joint capsule. The plane between the infraspinatus and the underlying capsule is often obliterated by scar tissue and must be meticulously recreated.

Clinical Pearl: Do not dissect below the level of the teres minor. Aggressive inferior dissection risks direct injury to the axillary nerve within the quadrangular space, or the suprascapular nerve as it courses through the spinoglenoid notch near the inferior border of the supraspinatus fossa. Traction on the infraspinatus must be applied carefully to avoid stretch neuropraxia of the suprascapular nerve.
Anterior Mobilization and Interval Slides
Continue mobilization anteriorly toward the supraspinatus. The supraspinatus and subscapularis muscles have strong, dense fascial attachments to the coracoid base via the coracohumeral ligament. Sharp release of the coracohumeral ligament in this area is absolutely essential and allows for significant lateral excursion of the supraspinatus. This is often referred to as an anterior interval slide.
If necessary, additional superior exposure and mobilization can be gained by performing a posterior interval slide, releasing the interval between the supraspinatus and infraspinatus. Furthermore, resecting the distal 1.0 to 1.5 cm of the clavicle at the acromioclavicular (AC) joint can provide superior access. However, this should be strictly reserved for patients with concomitant, symptomatic AC joint arthrosis to avoid unnecessary destabilization of the shoulder girdle.
Capsular Release
If the supraspinatus and infraspinatus tendons remain severely retracted and adequate length cannot be obtained despite the aforementioned bursal and interval releases, a formal capsular release is indicated. The superior capsule is often contracted and tethering the tendon medially.
Incise the capsule sharply at its insertion into the superior glenoid labrum. If necessary, carry this incision from the 8-o’clock position posterior to the 4-o’clock position anterior. This critical step completely separates the rotator cuff from the underlying glenohumeral joint, allowing the muscle belly to slide laterally independent of the contracted glenohumeral capsule.
Note: The use of a second posterior incision over the scapular spine to increase mobilization has been described historically (e.g., the Debeyre technique), but it results in a documented loss of muscle strength of at least one grade, causes significant morbidity, and is generally not recommended in modern orthopaedic practice.
Footprint Preparation and Repair Biomechanics
The goals of mobilization and footprint preparation are fourfold:
1. Obtain healthy tendon tissue of adequate biomechanical strength.
2. Position the tendon anatomically without tension, nerve damage, or deltoid compromise.
3. Decompress the subacromial space to prevent mechanical impingement.
4. Maximize the biological surface area for tendon-to-bone healing.
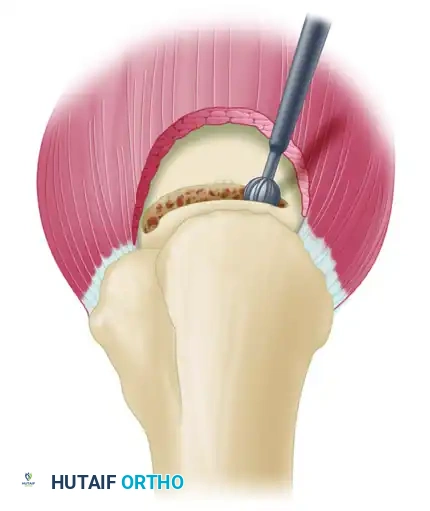
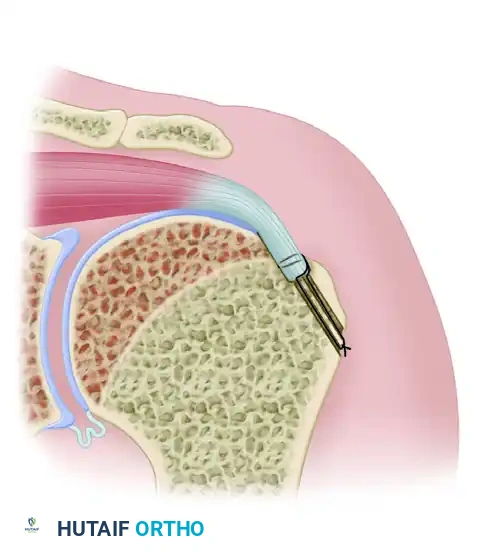
Creating the Bony Trough
Débride the end of the mobilized tendon to obtain a raw, bleeding edge, taking extreme care not to confuse the true tendon substance with the overlying hypertrophic bursa, which holds no biomechanical strength.
Use a rongeur, osteotome, or motorized high-speed burr to create a shallow, bleeding trough running the length of the exposed footprint on the greater tuberosity. This trough accommodates the thickness of the supraspinatus and infraspinatus tendons, promoting marrow-derived stem cell access to the repair site.
Surgical Pearl: Always bevel the proximal edge of the trough with a burr or rasp. A sharp cortical edge will act as a mechanical fulcrum, leading to premature suture abrasion and catastrophic failure at the tendon-bone interface during early postoperative rehabilitation.
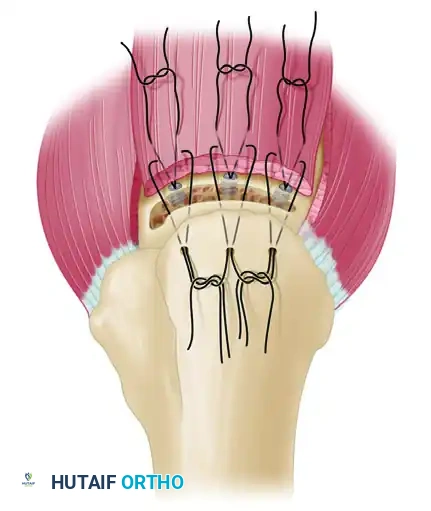
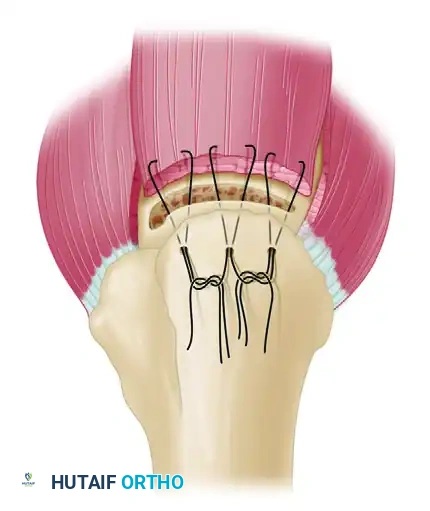
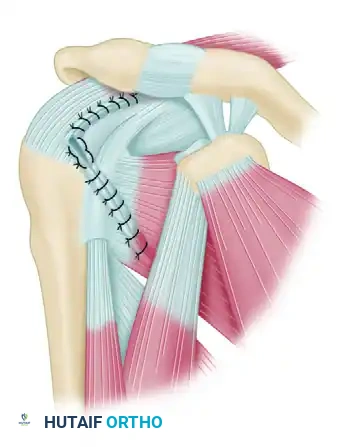
The Double-Row Repair Technique
We strongly advocate for a double-row or transosseous-equivalent technique, suturing the tendon to bone in a cancellous trough in combination with medial suture anchor fixation. This construct significantly reduces tension on the primary trough repair, dramatically increases the footprint contact area, and provides superior biomechanical yield strength and load-to-failure characteristics compared to traditional single-row repairs.
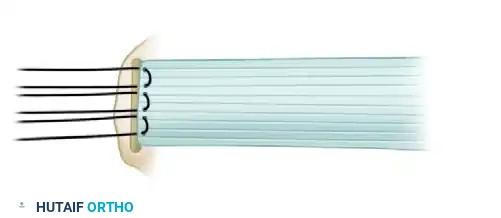
- Medial Row (Anchors): Place two or three fully threaded rotator cuff suture anchors immediately medial to the articular margin of the trough at a 45-degree angle (the "deadman's angle" to maximize pullout strength).
- Suture Passing: Pass the sutures through the rotator cuff tendon 3 to 5 mm medial to the freshly debrided free edge, utilizing a Mason-Allen or modified Mason-Allen configuration to maximize tissue grip.

- Lateral Row (Transosseous Tunnels): Drill holes for sutures 2 to 3 cm distal to the trough on the lateral humeral cortex. Connect these holes to the trough using a No. 5 Mayo needle, a towel clip, or a specialized suture-passing instrument.
Pitfall: Take extreme care not to fracture the thin cortical bone of the lateral humerus, which is frequently osteoporotic in this elderly patient demographic. Space the drill holes at least 5 mm (preferably 1 cm) apart to provide an adequate cortical bone bridge over which to tie the knots securely.
- Knot Tying: With No. 2 ultra-high-molecular-weight polyethylene (UHMWPE) nonabsorbable suture, use a double loop technique (superior to inferior, and inferior to superior) in a horizontal mattress manner. This configuration helps push the tendon down directly into the bleeding cancellous trough. Tie the anchor sutures down on top of the tendon with four or five alternating half-hitches to prevent impingement of the knot stack against the acromion.
Salvage Note: If the lateral humeral cortex fractures during the tying of the transosseous sutures, lateral row knotless suture anchors can be used as a rapid salvage procedure. Anchors have adequate holding power in cancellous bone and are excellent alternatives in problematic, highly osteoporotic situations.
Management of Massive and Irreparable Tears
Occasionally, despite the surgeon’s most diligent and aggressive efforts to mobilize the tendons via interval slides and capsular releases, tension remains unacceptably high. Cordasco and Bigliani identified five critical factors that improve the results of operative treatment for large and massive rotator cuff tears:
1. Adequate subacromial decompression.
2. Maintaining the integrity of the deltoid origin.
3. Mobilizing torn tendons and performing an interval slide when indicated.
4. Repairing tendons directly to bone.
5. Carefully supervising and staging postoperative rehabilitation.
In the ideal repair, the arm can be brought down to the patient’s side without tension. If tension remains, several salvage options exist, though none are biomechanically ideal and all represent a compromise.
Marginal Convergence (Partial Repair)
Partial repair of massive rotator cuff tears is an excellent alternative to simple débridement, aiming to restore the transverse force couple even if the supraspinatus cannot be fully lateralized. The initial step is a side-to-side tendon repair that results in "marginal convergence" toward the greater tuberosity.
By suturing the anterior (subscapularis/anterior supraspinatus) and posterior (infraspinatus) leaves of the tear together, the surgeon decreases the strain at the free margin of the rotator cuff, enhancing the mechanics of the construct and converting a massive U-shaped tear into a smaller, manageable crescentic tear that can then be repaired to bone with significantly less tension.
The McLaughlin Technique (Nonanatomical Repair)
If the tendon absolutely cannot reach the anatomical footprint despite maximal mobilization and marginal convergence, McLaughlin described suturing the tendon to a trough in bone at whatever point it can reach on the humeral head without undue tension.
This may require creating a bony trough more proximally (approximately 1 to 2 cm medial to the greater tuberosity) through the articular cartilage of the anterior neck area. While this achieves a watertight closure and partially restores the force couple, the mechanical advantage of the muscle-tendon unit is significantly diminished due to the proximal advancement and loss of the normal moment arm.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and careful patient selection, open rotator cuff repair is associated with a specific profile of complications. The most frequent complication remains the structural failure of the repair, or re-tear. The incidence of re-tearing is directly proportional to the initial tear size, the degree of fatty infiltration, and the patient's age
