Mastering Lateral Collateral Ligament Reconstruction of the Elbow: An Intraoperative Guide to the Figure-8 Yoke and Split Anconeus Fascia Transfer Techniques
Key Takeaway
Step into the operating room for a comprehensive masterclass on lateral collateral ligament (LCL) reconstruction of the elbow. This guide covers detailed anatomy, patient positioning, and meticulous intraoperative execution of both the Figure-8 Yoke and Split Anconeus Fascia Transfer techniques. Learn crucial pearls for preventing complications and ensuring successful outcomes for posterolateral rotatory instability (PLRI).
Comprehensive Introduction and Patho-Epidemiology
Welcome, esteemed colleagues, to the operating theater. Today, we are tackling a challenging but immensely rewarding procedure: Lateral Collateral Ligament (LCL) Reconstruction of the elbow. This is not merely an exercise in soft tissue repair; it is a complex biomechanical restoration aimed at re-establishing the fundamental stability of a highly constrained articulation. Our primary objective is to prevent the debilitating cascade of posterolateral rotatory instability (PLRI) and, ultimately, to return our patients to their highest possible level of function. This chapter serves as an exhaustive, intraoperative masterclass on the subject, focusing specifically on the Figure-8 Yoke and Split Anconeus Fascia Transfer techniques.
Posterolateral rotatory instability represents a complex, three-dimensional spectrum of elbow instability, almost universally initiated by insufficiency of the lateral collateral ligament complex. The pathomechanics involve a predictable sequence of tissue failure, famously described by O'Driscoll as the "Horii circle." This cascade begins on the lateral side with the disruption of the lateral ulnar collateral ligament (LUCL) and progresses anteriorly and posteriorly to involve the capsule, eventually reaching the medial collateral ligament in cases of frank dislocation. While academic debate persists regarding whether isolated injury to the LUCL alone is sufficient to cause symptomatic PLRI, or if broader capsuloligamentous involvement is requisite, the clinical consensus remains clear: significant lateral-sided trauma is the primary culprit.
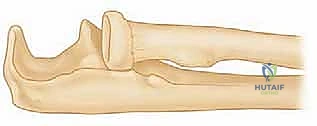
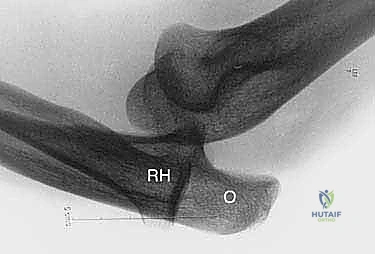
To truly understand the pathology, one must visualize the kinematics of the injury. Imagine the patient's forearm is supinated and slightly flexed. When an axial load coupled with a valgus stress is applied, the attenuated or absent LCL allows the ulnohumeral joint to rotate externally. This abnormal rotation compresses the radiocapitellar joint, acting as a fulcrum, and ultimately forces the radial head to subluxate or frankly dislocate posteriorly relative to the capitellum. This pathognomonic movement is the hallmark of PLRI and forms the basis for our diagnostic provocative testing. If left untreated, this chronic abnormal tracking leads to rapid radiocapitellar arthrosis and profound functional disability.
Beyond acute, high-energy trauma such as elbow dislocations, orthopedic surgeons frequently encounter LCL attenuation in more insidious clinical scenarios. Patients with a history of multiple lateral elbow surgeries, particularly aggressive lateral epicondyle debridements or repeated corticosteroid injections, are at high risk for iatrogenic PLRI. Furthermore, patients presenting with residual cubitus varus following malunion of pediatric supracondylar humerus fractures experience chronic, altered biomechanical vectors that progressively stretch the lateral ligamentous restraints. These chronic, non-traumatic cases often present with subtle mechanical symptoms—clicking, snapping, or a feeling of apprehension—rather than the dramatic frank dislocations seen in the emergency department.
Detailed Surgical Anatomy and Biomechanics
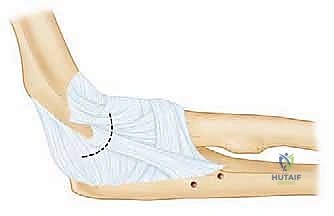
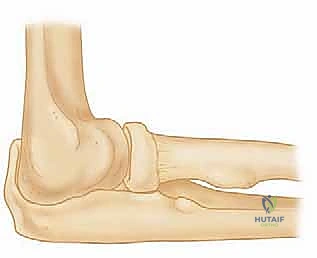
Before a scalpel ever touches the skin, a profound understanding of the lateral elbow's surgical anatomy is non-negotiable. The lateral collateral ligament complex is not a single band, but rather a sophisticated, multi-layered fascial and ligamentous network crucial for posterolateral stability. It comprises four primary components that function synergistically. The most critical of these is the Lateral Ulnar Collateral Ligament (LUCL), sometimes referred to in older literature as the Radial Ulnohumeral Ligament (RUHL). This structure is our primary target for reconstruction. It originates from a broad, flat footprint on the lateral epicondyle, specifically at the isometric center of rotation of the capitellum, and courses distally and posteriorly to insert on the supinator crest of the proximal ulna.
The other components of the complex play vital secondary roles. The Radial Collateral Ligament (RCL) proper is located more anteriorly and primarily resists varus stress, inserting into the annular ligament rather than directly onto bone. The Annular Ligament itself is a robust, funnel-shaped fibrous band that sweeps around the radial head, stabilizing the proximal radioulnar joint and serving as an anchoring point for the RCL. Finally, the Accessory Collateral Ligament, when present, provides supplementary stabilization to the annular ligament during varus stress. All these ligaments originate deep to the common extensor muscle mass, creating a complex three-dimensional envelope around the radiocapitellar joint.

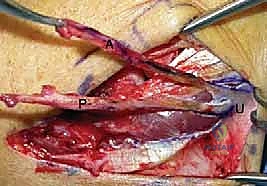
Navigating this anatomy surgically requires an intimate knowledge of the surrounding muscular intervals and neurovascular structures. Our primary workhorse approach utilizes the Köcher interval, a fascial plane located between the anconeus (innervated by the radial nerve) and the extensor carpi ulnaris (ECU, innervated by the posterior interosseous nerve). While this is an internervous plane and relatively safe, meticulous blunt dissection is paramount. The dynamic stabilizers of the elbow, specifically the anconeus and the extensor muscle groups (ECU, ECRB, ECRL), provide crucial active stability against varus and posterolateral rotatory forces. Preserving their fascial origins and muscular integrity during the approach is just as important as the ligament reconstruction itself for optimal post-operative function.
The most critical neurovascular consideration during any lateral elbow approach is the Posterior Interosseous Nerve (PIN). As a major motor branch of the radial nerve, the PIN passes between the two heads of the supinator muscle, traversing the arcade of Frohse. To protect this vital structure, the surgeon must maintain the forearm in strict pronation throughout the deep dissection. Pronation dynamically rotates the supinator muscle belly and the encased PIN anteriorly and medially, safely distancing it from the surgical field near the supinator crest. Additionally, the Lateral Antebrachial Cutaneous Nerve (LABCN) must be identified and protected during the superficial subcutaneous dissection to prevent painful post-operative neuromas or dysesthesia.
Exhaustive Indications and Contraindications
The diagnostic journey for PLRI requires a high index of suspicion, as the clinical presentation can be remarkably subtle. Patients typically report a history of trauma, though an increasing number present with iatrogenic instability following recurrent lateral epicondylitis surgery. While younger patients (under 20 years of age) frequently report a history of frank elbow dislocations, elderly patients or those with chronic attenuation often do not. The classic, unifying complaint is the presence of mechanical-type symptoms—recurrent clicking, popping, catching, or a sensation of the joint "slipping" out of place—specifically exacerbated during activities that combine elbow supination, extension, and axial loading, such as pushing up from a chair.
Physical examination in the awake patient is notoriously difficult due to intense muscle guarding and apprehension. However, several provocative tests are essential. The Supine Lateral Pivot-Shift Test is the gold standard. With the patient supine and the arm overhead, the elbow is slightly flexed, and a valgus stress, axial load, and supination force are applied. A positive test reveals the radial head subluxating posteriorly, followed by a palpable and often visible "clunk" as the elbow flexes past 40 degrees and the joint relocates. Because this is painful and terrifying for the patient, the Push-up Test and the Chair Push-up Test are highly useful clinical surrogates; reproduction of apprehension or lateral elbow pain during these maneuvers strongly suggests PLRI.

Advanced imaging is critical for confirming the diagnosis and ruling out concomitant pathology. Standard anteroposterior and lateral radiographs are often normal but may reveal subtle signs such as small avulsion fractures of the lateral epicondyle (the "fleck sign") or early radiocapitellar arthrosis. Stress radiographs, however, are paramount. When performed correctly, they objectively demonstrate widening of the ulnohumeral joint space and posterior subluxation of the radial head. Magnetic Resonance Imaging (MRI), particularly MR arthrography with intra-articular contrast, is the imaging modality of choice to clearly delineate tears or attenuation of the LUCL complex and to assess the integrity of the common extensor origin.
| Category | Specific Criteria |
|---|---|
| Absolute Indications | Recurrent, symptomatic PLRI confirmed by exam/imaging; Failure of a 3-6 month trial of non-operative management (bracing, therapy); Acute, massive LCL avulsions with gross instability preventing early ROM. |
| Relative Indications | Symptomatic PLRI in high-demand athletes or manual laborers; Concomitant radial head fractures requiring excision/replacement where the LCL must be repaired to restore stability; Iatrogenic instability following lateral epicondylectomy. |
| Absolute Contraindications | Active joint infection (septic arthritis); Severe, uncorrectable osseous deformity of the distal humerus or proximal ulna precluding stable fixation; Medically unstable patient unfit for anesthesia. |
| Relative Contraindications | Advanced, bone-on-bone radiocapitellar or ulnohumeral osteoarthritis (reconstruction may increase pain by increasing joint contact pressures); Poor soft tissue envelope or active skin infection over the surgical site; Patient non-compliance with complex post-operative rehabilitation protocols. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful LCL reconstruction. The surgical goal is not merely to tether the joint, but to meticulously recreate the isometric biomechanics of the native LUCL. This begins with a comprehensive review of all imaging modalities. The surgeon must evaluate the osseous stock of the lateral epicondyle and the supinator crest, as cystic changes or previous drill holes (from prior epicondylitis surgery) may dictate the use of alternative fixation methods or modified tunnel trajectories. Furthermore, the choice of graft must be finalized preoperatively. Autografts, such as the palmaris longus or a strip of triceps fascia, are preferred for their biological incorporation and lack of disease transmission risk. However, in revision scenarios or when autograft is unavailable, robust allografts (e.g., gracilis or semitendinosus) are excellent alternatives.
An Examination Under Anesthesia (EUA) is a mandatory, non-negotiable step in the pre-operative workflow. Once the patient is fully anesthetized and paralyzed, the protective muscle guarding is eliminated, allowing for an unhindered assessment of joint laxity. The surgeon must perform a definitive pivot-shift test and varus stress testing, often under live fluoroscopy, to document the exact degree and direction of instability. This real-time dynamic assessment confirms the preoperative diagnosis, rules out subtle concomitant medial-sided laxity, and provides a baseline against which the final reconstructed stability will be judged before the patient leaves the operating room.

Patient positioning must facilitate unhindered access to the lateral elbow while allowing full, dynamic range of motion throughout the procedure. The patient is placed supine on the operating table. The affected arm is typically positioned on a radiolucent hand table or arm board. Alternatively, placing the arm across the patient's chest can offer excellent visualization of the lateral aspect and allows the surgeon to easily range the elbow to assess isometricity during graft tensioning. A sterile, well-padded tourniquet is applied high on the brachium. The entire arm, from the fingertips to the axilla, is prepped and draped free to ensure the surgeon has complete control over forearm rotation and elbow flexion at all times.
Fluoroscopy setup is equally critical. A C-arm must be positioned to easily obtain true, orthogonal anteroposterior and lateral views of the elbow without compromising the sterile field. The monitor should be in the surgeon's direct line of sight. Intraoperative imaging is utilized not only during the EUA but extensively during the procedure to verify the precise placement of guide pins for bone tunnels. Ensuring that the humeral tunnel is perfectly centered on the capitellar axis of rotation, and that the ulnar tunnels have an adequate cortical bridge, prevents catastrophic intraoperative fractures and guarantees the biomechanical success of the reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped and the tourniquet inflated, we initiate the surgical approach. A 10-centimeter longitudinal incision is centered directly over the lateral epicondyle. The incision extends proximally along the lateral supracondylar ridge of the humerus and distally towards the supinator crest of the ulna. Careful subcutaneous dissection is performed to elevate full-thickness fasciocutaneous flaps. During this superficial phase, meticulous hemostasis is maintained, and a concerted effort is made to identify and gently retract any branches of the lateral antebrachial cutaneous nerve to prevent post-operative neuromas.
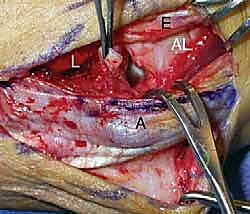
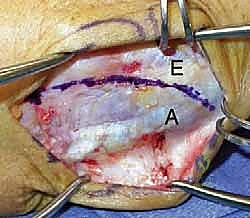
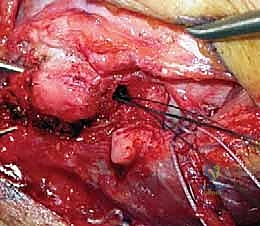
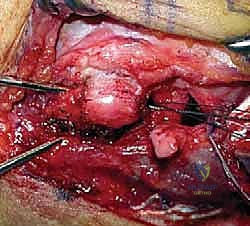
The deep dissection targets the Köcher interval, the primary surgical corridor for lateral elbow pathology. This interval is identified by locating the fascial raphe between the anconeus muscle posteriorly and the extensor carpi ulnaris (ECU) anteriorly. Distally, this interval can sometimes be difficult to discern; starting proximally at the lateral epicondyle and dissecting distally often facilitates identification. The fascia is incised sharply along this line. The ECU and the common extensor origin are elevated anteriorly, while the anconeus is retracted posteriorly. It is at this exact moment that the surgical assistant must ensure the forearm is fully pronated. This critical maneuver physically shifts the posterior interosseous nerve (PIN) anteriorly, burying it within the supinator muscle belly and pulling it safely away from our retractor blades and drill paths.
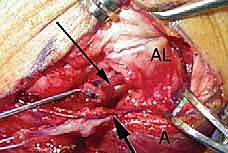
Once the joint capsule is exposed, a longitudinal arthrotomy is performed slightly anterior to the equator of the radial head. This provides excellent visualization of the radiocapitellar joint and allows for inspection of the articular cartilage. We now identify the anatomic footprints for our reconstruction. On the ulnar side, the supinator crest is exposed by subperiosteal elevation of the supinator muscle, taking great care not to dissect too far anteriorly. On the humeral side, the isometric point is identified on the lateral epicondyle. This point corresponds to the central axis of rotation of the capitellum. Identifying this true isometric point is the most critical technical step of the procedure; a non-isometric graft will either stretch out over time or cause severe post-operative stiffness.

The Figure-8 Yoke Reconstruction Technique
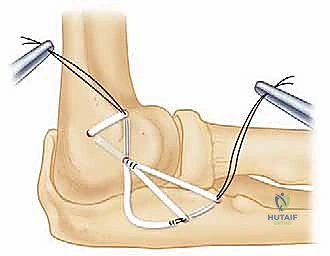
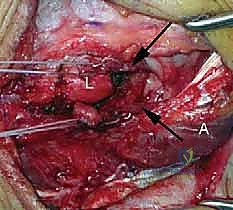
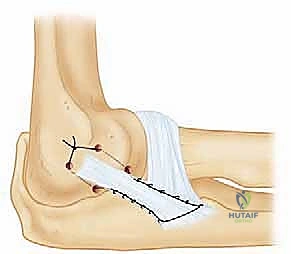
The Figure-8 Yoke technique is a highly robust, biomechanically superior method for reconstructing the LCL complex, utilizing a free tendon graft (typically palmaris longus or allograft). The process begins with the creation of the ulnar tunnels. Two drill holes, typically 3.2mm or 4.0mm depending on graft diameter, are created along the supinator crest. These holes are separated by a robust 1.5 to 2.0-centimeter cortical bone bridge to prevent pull-out. The drill bits are angled to converge within the medullary canal of the ulna, creating a continuous, intraosseous tunnel. A suture loop is passed through this tunnel to act as a shuttle for the graft.


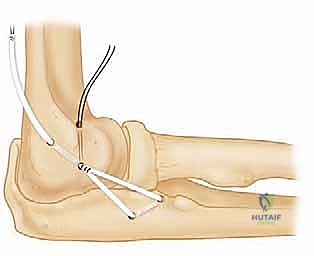
Attention is then turned to the humerus. A single, larger tunnel (or two converging smaller tunnels, depending on surgeon preference and fixation method) is drilled at the previously identified isometric point on the lateral epicondyle. The trajectory of this humeral tunnel is typically directed proximally and anteriorly to avoid penetrating the olecranon fossa. The free tendon graft is first passed through the ulnar tunnel. The two free ends of the graft are then crossed over the radiocapitellar joint in a "Figure-8" configuration. This crossing mimics the broad, fan-like stabilizing effect of the native ligamentous complex, providing superior resistance to posterolateral rotatory forces compared to a simple single-strand reconstruction.
The two free ends of the graft are subsequently shuttled into the humeral tunnel. Tensioning is the final, crucial step. The elbow is positioned in 30 to 40 degrees of flexion, and the forearm is placed in maximal pronation. This position reduces the posterolateral rotatory subluxation and approximates the native tension of the LUCL. While maintaining this position and applying a slight varus stress to ensure joint reduction, the graft limbs are pulled taut. Fixation within the humeral tunnel is achieved using a bio-tenodesis interference screw, cortical suspensory buttons, or heavy transosseous non-absorbable sutures tied over a bony bridge. The joint is then ranged to confirm stability and ensure the graft does not over-constrain the elbow in extension.
The Split Anconeus Fascia Transfer Technique
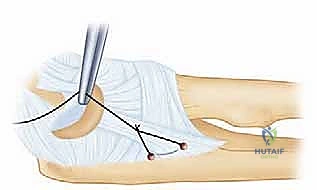
In specific clinical scenarios—such as low-demand elderly patients, cases of mild chronic attenuation, or as an augmentation to a primary repair—the Split Anconeus Fascia Transfer provides an elegant, local-tissue solution. This technique avoids the morbidity of autograft harvest and the costs associated with allografts. The procedure relies on utilizing the robust, contiguous fascia overlying the anconeus muscle, which naturally spans the lateral aspect of the elbow joint.
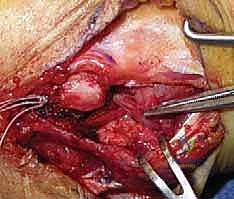
Following the standard lateral approach, the fascia of the anconeus is carefully delineated. A strip of this fascia, approximately 1.5 to 2.0 centimeters wide, is sharply incised. Crucially, the distal attachment of this fascial strip to the proximal ulna (near the supinator crest) is left entirely intact, serving as a living, vascularized ulnar footprint. The proximal portion of the fascial strip is then elevated off the underlying anconeus muscle belly, creating a mobilized flap of tissue that can be manipulated.
The mobilized proximal end of the anconeus fascia is then routed anteriorly and proximally towards the lateral epicondyle. A bony trough or a shallow tunnel is created at the isometric point on the lateral epicondyle, identical to the footprint used in the Figure-8 technique. The elbow is placed in 30 to 40 degrees of flexion and full pronation to reduce the joint. The fascial flap is drawn tightly into the humeral trough and secured using suture anchors or transosseous sutures. While biomechanically less rigid than a free tendon Figure-8 reconstruction, this transfer effectively acts as a dynamic check-rein against posterolateral rotatory subluxation.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, lateral collateral ligament reconstruction carries a distinct profile of potential complications. The orthopedic surgeon must be intimately familiar with these risks to counsel patients appropriately
