Medial Approach to the Distal Humerus: Master Techniques & Avoid Osteotomy

Key Takeaway
Learn more about Medial Approach to the Distal Humerus: Master Techniques & Avoid Osteotomy and how to manage it. The medial approach to the distal humerus is a surgical technique used to access the medial supracondylar ridge, common flexor/pronator origin, and medial elbow joint compartment. It is applied for extra-articular fractures of the medial column of the distal humerus, medial epicondylitis, ulnar collateral ligament repair, and loose body removal, without an epicondyle osteotomy.
Introduction and Epidemiology
The medial approach to the distal humerus represents a highly versatile, anatomic corridor utilized by orthopedic surgeons to address a spectrum of osseous, ligamentous, and intra-articular pathologies of the medial elbow. Historically, extensive exposure of the distal humerus relied heavily on trans-olecranon osteotomies or medial epicondyle osteotomies. However, advancements in anatomic understanding and internal fixation have popularized osteotomy-sparing approaches. The medial approach provides direct access to the medial supracondylar ridge, the medial epicondyle, the common flexor-pronator mass origin, and the medial compartment of the ulnohumeral joint without the requisite morbidity of an osteotomy.

Epidemiologically, isolated medial column fractures of the distal humerus (such as Milch Type I or AO/OTA 13-B1) are relatively rare compared to bicolumnar fractures, but they demand precise anatomic reduction to restore the trochlear groove and medial buttress, preventing late valgus instability or post-traumatic arthrosis. Furthermore, the medial approach is the workhorse for sports medicine surgeons addressing ulnar collateral ligament (UCL) insufficiency, a pathology increasingly prevalent among overhead throwing athletes. By avoiding a medial epicondyle osteotomy, surgeons mitigate the risks of nonunion, malunion, hardware prominence, and iatrogenic ulnar neuropathy, thereby facilitating accelerated postoperative rehabilitation protocols.
Surgical Anatomy and Biomechanics
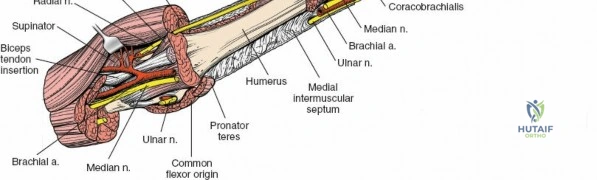
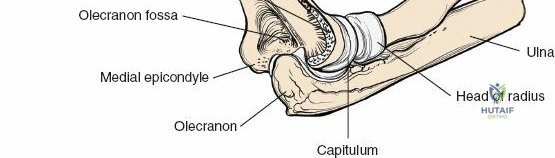
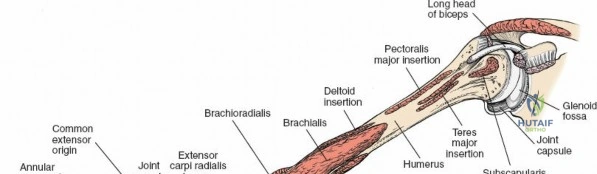
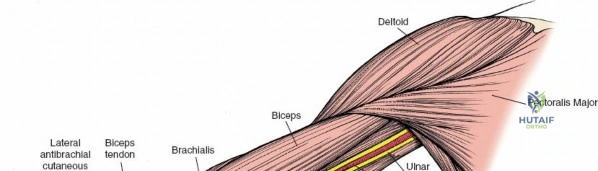
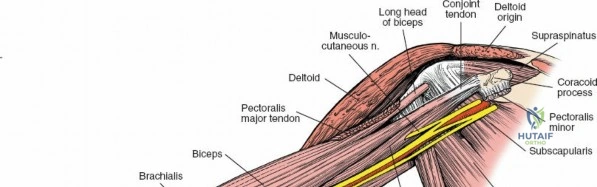
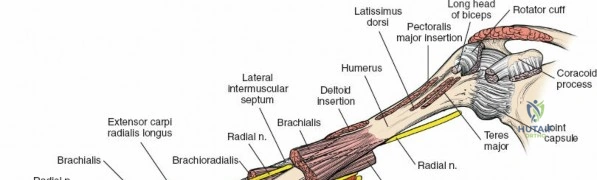
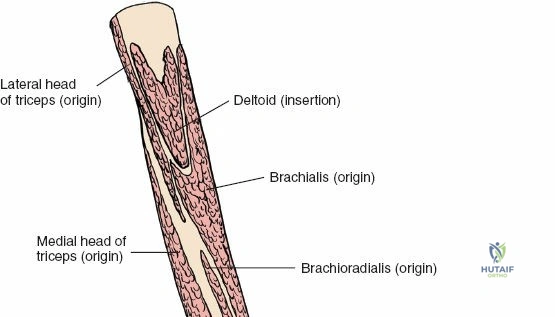
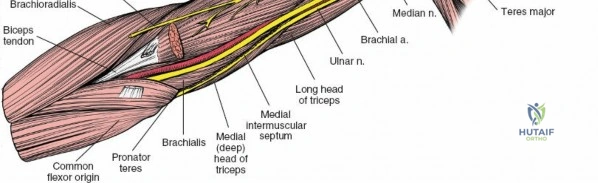
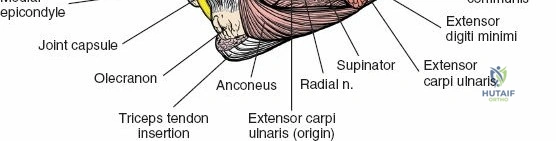
A profound comprehension of the medial elbow anatomy is paramount for executing this approach safely and effectively. The distal humerus is conceptualized as a two-column structure (medial and lateral) linked by the articular tie-arch (the trochlea and capitellum). The medial column diverges from the humeral shaft at approximately 45 degrees and terminates at the medial epicondyle, which serves as the primary origin for the ulnar collateral ligament complex and the flexor-pronator muscle mass.


Osseous and Ligamentous Anatomy
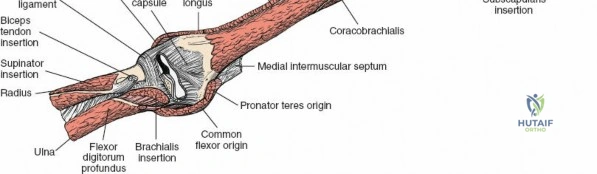
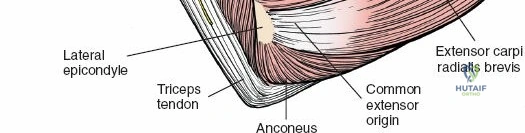
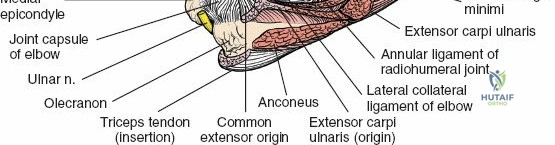
The medial epicondyle is a distinct, non-articular bony prominence. Just proximal to it lies the medial supracondylar ridge, which provides the attachment site for the medial intermuscular septum. The UCL complex is the primary restraint to valgus stress at the elbow. It consists of the anterior bundle (originating from the anteroinferior surface of the medial epicondyle and inserting on the sublime tubercle of the ulna), the posterior bundle, and the transverse ligament (Cooper's ligament). The anterior bundle is the most critical biomechanical stabilizer and is the primary focus during UCL reconstruction.


Neurovascular Structures
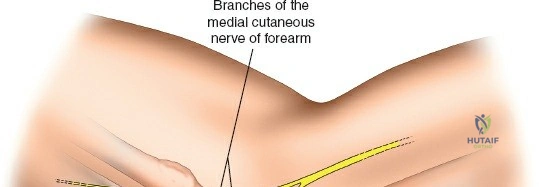
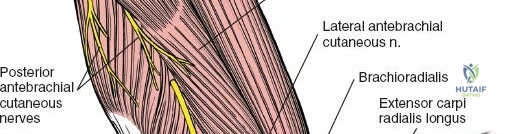
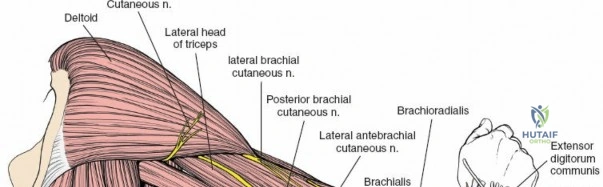
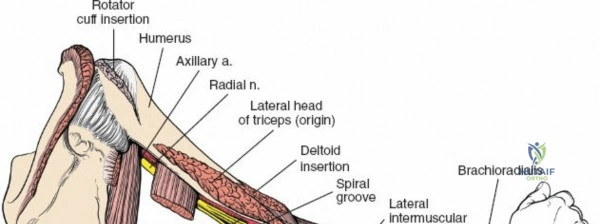
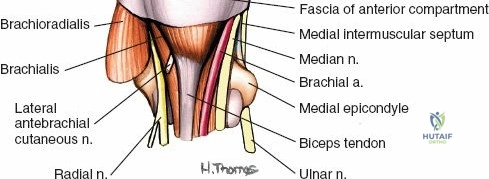
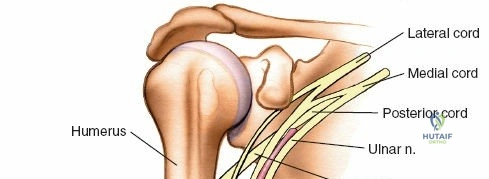
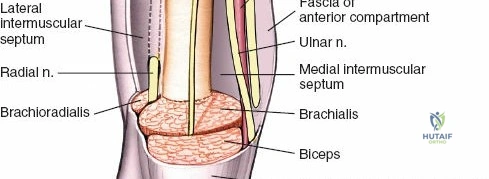
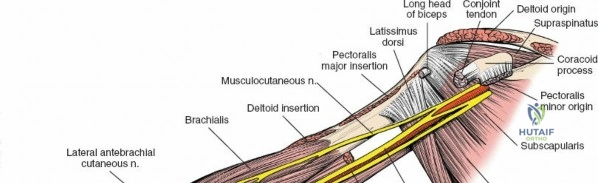
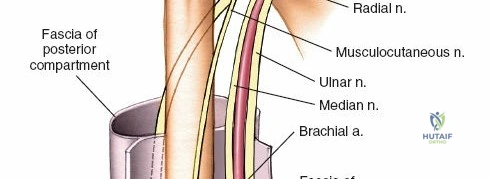
The ulnar nerve is the most critical structure at risk during the medial approach. It transitions from the anterior compartment of the arm to the posterior compartment by piercing the medial intermuscular septum at the arcade of Struthers (approximately 8 cm proximal to the medial epicondyle). It then travels distally along the posterior aspect of the medial epicondyle within the cubital tunnel, roofed by Osborne's fascia and the arcuate ligament of the flexor carpi ulnaris (FCU). The medial antebrachial cutaneous (MABC) nerve courses superficially in the subcutaneous tissue of the medial arm and forearm. Its anterior and posterior branches must be meticulously identified and protected during the initial superficial dissection to prevent painful neuroma formation.
Internervous Planes
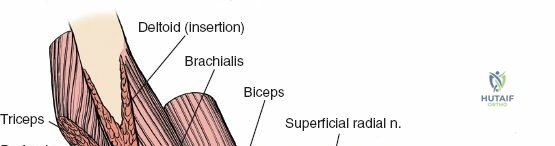
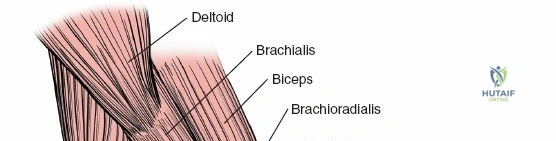
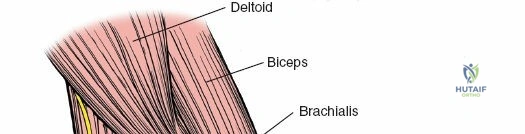
The approach exploits a reliable internervous plane. Proximally and posteriorly, the plane lies between the flexor-pronator group (arising from the medial epicondyle, innervated primarily by the median nerve, with the FCU innervated by the ulnar nerve) and the triceps brachii muscle (innervated by the radial nerve). Developing this plane allows for broad exposure of the medial column while preserving the motor innervation to the dynamic stabilizers of the elbow and wrist.
Indications and Contraindications
The medial approach is selectively utilized for pathologies isolated to the medial column or medial joint space. It is not designed for comprehensive bicolumnar exposure, which typically requires a posterior approach with or without an olecranon osteotomy.



Primary indications include the open reduction and internal fixation (ORIF) of extra-articular or simple intra-articular fractures of the medial column. It is also the standard approach for the surgical management of recalcitrant medial epicondylitis (golfer's elbow), repair or reconstruction of the UCL in throwing athletes, and the removal of loose bodies localized to the medial ulnohumeral joint space.
| Indication Category | Specific Clinical Scenarios | Operative Rationale |
|---|---|---|
| Trauma | Medial condyle fractures (Milch I/II), Medial epicondyle avulsions | Direct access for anatomic reduction and stable internal fixation of the medial column. |
| Sports Medicine | UCL tears, Valgus extension overload | Facilitates autograft/allograft routing and fixation (docking or interference screw techniques). |
| Degenerative | Recalcitrant medial epicondylitis | Allows excision of angiofibroblastic dysplasia within the flexor-pronator origin. |
| Intra-articular | Medial compartment loose bodies, Osteophytes | Capsulotomy allows direct visualization and extraction of joint debris. |
| Nerve Pathology | Cubital tunnel syndrome | Allows for in situ decompression or anterior transposition of the ulnar nerve. |
Contraindications include complex, comminuted bicolumnar distal humerus fractures (AO/OTA 13-C2 and 13-C3) where orthogonal or parallel plating of both columns is required, as the medial approach alone cannot provide adequate visualization of the capitellum or lateral column. Additionally, severe medial soft tissue compromise (e.g., traumatic degloving or active infection) precludes the use of this incision.


Pre Operative Planning and Patient Positioning
Thorough preoperative planning relies on high-quality orthogonal radiographs of the elbow. For intra-articular fractures, a non-contrast Computed Tomography (CT) scan with 3D reconstructions is highly recommended to delineate articular comminution and dictate plate positioning. For ligamentous injuries, Magnetic Resonance Imaging (MRI) or MR arthrography is utilized to assess the integrity of the UCL anterior bundle and evaluate for concomitant flexor-pronator tears or osteochondral defects.



Patient positioning is dictated by surgeon preference, concurrent injuries, and the specific pathology being addressed. Two primary positions are utilized: prone and supine.
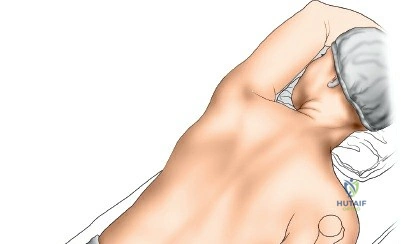
Prone Positioning
Placing the patient prone on the operating table is highly advantageous for posterior and medial access. The arm is positioned such that the elbow is flexed to 90 degrees, and the forearm is allowed to hang in neutral rotation over a padded bolster or arm board. This position allows gravity to assist with elbow flexion and naturally retracts the triceps posteriorly, facilitating exposure of the posterior aspect of the medial column. It is particularly useful for fracture fixation where posterior plate application is planned.




Supine Positioning
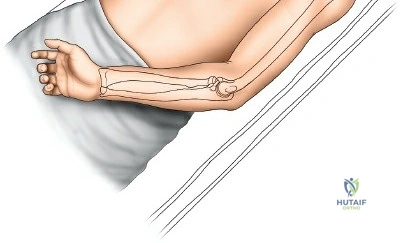
Alternatively, the patient may be placed supine. The operative arm is supported on a radiolucent hand table. The shoulder is abducted and maximally externally rotated so that the medial epicondyle faces anteriorly toward the surgeon. The elbow is flexed to 90 degrees. This position is generally preferred for UCL reconstructions, medial epicondylitis surgery, and in polytrauma patients where prone positioning is contraindicated due to airway, spine, or thoracic concerns.
Regardless of the position chosen, the limb is exsanguinated by elevating it for 3 to 5 minutes or by applying an Esmarch bandage. A sterile pneumatic tourniquet is then inflated to an appropriate pressure (typically 250 mmHg) to ensure a bloodless surgical field.


Detailed Surgical Approach and Technique
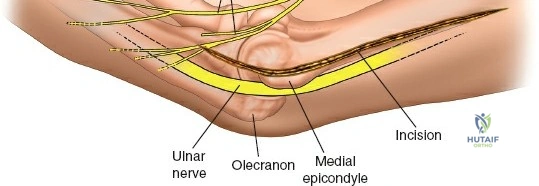
Landmarks and Incision
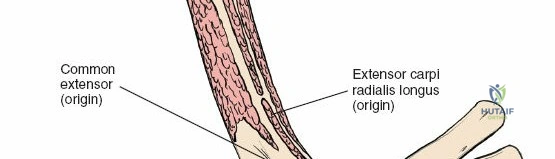
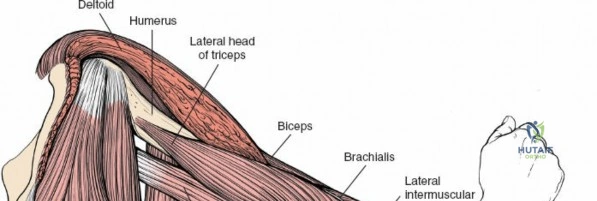
The primary osseous landmark is the medial epicondyle of the humerus, a large subcutaneous bony mass on the medial aspect of the distal humerus. Proximal to the epicondyle, the medial supracondylar ridge can be palpated, though it is often obscured by the overlying triceps and brachialis musculature.
The incision is typically 8 to 10 centimeters in length, centered directly over or slightly posterior to the medial epicondyle. For fracture work, the incision may be extended proximally along the medial supracondylar ridge. For UCL reconstruction, a slightly more anterior trajectory following the flexor-pronator mass may be utilized.



Superficial Dissection and Ulnar Nerve Management
The superficial dissection begins with careful incision of the subcutaneous tissues. Meticulous hemostasis is maintained. The surgeon must remain vigilant for branches of the MABC nerve, which cross the operative field transversely. These branches should be mobilized and protected with vessel loops; transection leads to painful neuromas that can severely compromise postoperative outcomes.
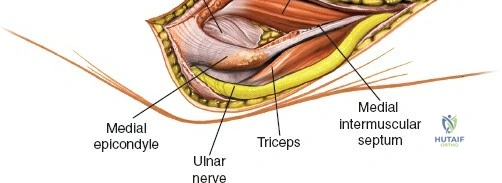
The most critical step in the superficial dissection is the identification and management of the ulnar nerve. The nerve is palpated as it resides in the cubital tunnel posterior to the medial epicondyle. The fascia overlying the nerve is incised, starting proximal to the medial epicondyle and extending distally into the forearm. The nerve is isolated along the entire length of the incision.
Depending on the pathology, the ulnar nerve may be managed via in situ decompression or formal anterior transposition. For extensive medial column plating, anterior subcutaneous or submuscular transposition is often required to prevent hardware impingement and tension on the nerve during fracture reduction. If transposed, the medial intermuscular septum must be excised proximally to prevent nerve kinking.



Deep Dissection and Articular Exposure
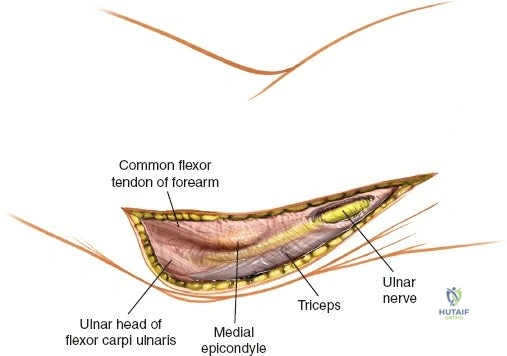
Once the ulnar nerve is protected, the deep dissection proceeds by exploiting the internervous plane between the flexor-pronator mass and the triceps. The medial intermuscular septum is identified. The triceps muscle is elevated bluntly from the posterior aspect of the medial supracondylar ridge and retracted posteriorly. Anteriorly, the brachialis and the flexor-pronator mass are elevated and retracted anteriorly.
To access the medial epicondyle and the supracondylar ridge without an osteotomy, the surgeon works on either side of the epicondyle. If necessary for fracture visualization, the origin of the flexor-pronator mass can be partially elevated subperiosteally, though a cuff of tissue should be preserved for later repair.
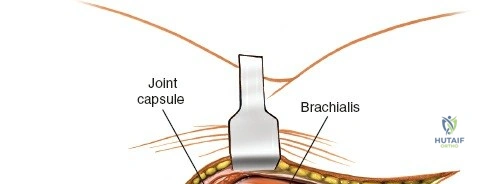
If access to the articular surface is required (e.g., for loose body removal or visualization of a trochlear fracture line), a longitudinal arthrotomy is performed through the medial capsule. The anterior bundle of the UCL must be strictly protected during this capsulotomy unless it is the target of the repair.

Fracture Reduction and Fixation Strategies
For medial column fractures, anatomic reduction is achieved using pointed reduction forceps. Temporary fixation is secured with Kirschner wires. Definitive fixation typically involves the application of a pre-contoured 3.5 mm or 2.7 mm anatomic locking plate. The plate is usually applied to the medial or posteromedial crest of the distal humerus.
Screws directed into the articular block must be carefully measured to avoid joint penetration, particularly in the region of the olecranon and coronoid fossae. The avoidance of an epicondylar osteotomy ensures that the flexor-pronator origin remains undisturbed, providing a robust, vascularized soft-tissue envelope over the hardware.
Closure and Layered Reconstruction
Following fixation or ligamentous reconstruction, the wound is copiously irrigated. The tourniquet is deflated, and meticulous hemostasis is achieved. If the ulnar nerve was transposed, a fascial sling may be created to prevent posterior subluxation. The flexor-pronator fascia is repaired if it was incised. The subcutaneous tissues and skin are closed in a layered fashion. A sterile compressive dressing and a posterior plaster splint are applied with the elbow in 90 degrees of flexion.
Complications and Management
The medial approach to the distal humerus is generally safe, but its proximity to critical neurovascular structures and the inherent tendency of the elbow to develop stiffness necessitate meticulous surgical technique.
| Complication | Incidence / Risk Factors | Prevention and Salvage Strategies |
|---|---|---|
| Ulnar Neuropathy | Up to 15% in trauma settings. Risk increased with excessive traction or hardware prominence. | Routine isolation and protection. Consider anterior transposition if hardware is prominent or tension is high. Salvage: Secondary neurolysis and transposition. |
| MABC Neuroma | 5-10%. Caused by transection of anterior/posterior branches. | Meticulous superficial dissection. Identify and protect branches with vessel loops. Salvage: Excision of neuroma and burying proximal stump into muscle. |
| Elbow Stiffness | Common after any elbow trauma/surgery. | Rigid internal fixation allowing early active ROM. Avoid prolonged immobilization (>2 weeks). Salvage: Arthroscopic or open arthrolysis. |
| Heterotopic Ossification (HO) | High risk in head trauma, burns, or delayed fixation. | Gentle soft tissue handling. Consider prophylactic Indomethacin or single-dose radiation in high-risk patients. Salvage: Surgical excision once bone scan is cold. |
| Hardware Prominence | Medial epicondyle has minimal soft tissue coverage. | Use low-profile, pre-contoured plates. Ensure screw heads are flush. Salvage: Hardware removal after clinical and radiographic union. |
Ulnar neuropathy remains the most significant concern. Transient neuropraxia often resolves with observation, but progressive motor or sensory deficits may warrant early re-exploration. Stiffness is combated primarily through rigid fixation that permits immediate postoperative rehabilitation.
Post Operative Rehabilitation Protocols
Rehabilitation protocols must be tailored to the specific procedure performed. For stable internal fixation of medial column fractures, the goal is early motion.
Phase I (0-2 weeks): The patient is placed in a posterior splint for 7-10 days to allow soft tissue rest. Active and active-assisted range of motion (ROM) of the wrist and shoulder are encouraged immediately.
Phase II (2-6 weeks): The splint is transitioned to a hinged elbow brace. Active and active-assisted ROM of the elbow is initiated. Extension block splinting may be utilized if there are concerns regarding ligamentous stability. Strengthening is strictly avoided to protect the fracture site or UCL graft.
Phase III (6-12 weeks): Once radiographic evidence of union is observed (or graft incorporation is progressing), progressive resistance exercises are initiated. Focus is placed on isotonic strengthening of the flexor-pronator mass and triceps.
Phase IV (3-6 months): For athletes undergoing UCL reconstruction
