Ulnohumeral (Outerbridge-Kashiwagi) Arthroplasty: An Intraoperative Masterclass

Key Takeaway
This masterclass provides a comprehensive, intraoperative guide to Ulnohumeral (Outerbridge-Kashiwagi) Arthroplasty for primary elbow osteoarthritis. We'll meticulously cover surgical anatomy, patient positioning, step-by-step execution including osteophyte removal and foraminectomy, critical pearls, potential pitfalls, and essential postoperative management. Fellows will gain a granular understanding of this technique to restore elbow function and alleviate pain.
Comprehensive Introduction and Patho-Epidemiology
The ulnohumeral arthroplasty, classically recognized in the orthopedic literature as the Outerbridge-Kashiwagi (O-K) procedure, represents a pivotal surgical intervention for the management of advanced primary osteoarthritis of the elbow. Originally conceptualized to address the debilitating mechanical impingement seen in degenerative elbow disease, this procedure has evolved into a highly refined, joint-preserving technique. It is specifically designed to restore functional range of motion and alleviate the severe, impingement-related pain that manifests at the extreme arcs of flexion and extension. Unlike total elbow arthroplasty, which carries significant lifelong lifting restrictions and a higher complication profile, the O-K arthroplasty preserves the native joint architecture and allows patients to return to heavy manual labor and high-demand physical activities.
Primary osteoarthritis of the elbow is a relatively uncommon clinical entity when compared to weight-bearing joints like the hip or knee, affecting approximately 2% of the general population. However, its demographic distribution is highly specific; it predominantly afflicts middle-aged males, typically presenting in the fifth or sixth decade of life. The exact pathophysiological etiology remains somewhat elusive, but biomechanical studies and clinical histories strongly correlate the condition with repetitive, high-impact mechanical stress and overuse. Patients frequently present with a history of employment in heavy manual labor (such as construction, carpentry, or pneumatic drill operation) or participation in rigorous upper-extremity athletics (such as weightlifting, throwing sports, or gymnastics). In younger cohorts, predisposing factors such as a history of osteochondritis dissecans of the capitellum or subtle, undiagnosed ligamentous instability may serve as the catalyst for early-onset degenerative changes.
The hallmark pathologic cascade of primary elbow osteoarthritis is characterized by the robust formation of periarticular osteophytes, with relative preservation of the central articular cartilage until the very late stages of the disease. This is a stark contrast to rheumatoid arthritis or post-traumatic osteoarthritis, where global cartilage destruction and joint space narrowing are early and prominent features. In primary osteoarthritis, hypertrophic bone formation occurs most aggressively at the margins of the olecranon, the coronoid process, and within their respective fossae on the distal humerus. As these osteophytes enlarge, they create a mechanical block, leading to the classic clinical presentation of pain at the extremes of motion and a progressive loss of terminal extension and flexion. Furthermore, the fragmentation of these osteophytes frequently leads to the formation of intra-articular loose bodies, which lodge in the dependent recesses of the joint, exacerbating mechanical symptoms, causing sudden locking, and accelerating capsular contracture.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of elbow anatomy and kinematics is an absolute prerequisite for executing the Outerbridge-Kashiwagi arthroplasty safely and effectively. The elbow is a highly constrained, complex modified hinge joint comprising three distinct articulations encased within a single synovial cavity: the ulnohumeral joint, the radiocapitellar joint, and the proximal radioulnar joint. For the O-K procedure, our primary focus is the ulnohumeral articulation, which governs the primary arc of flexion and extension. The distal humerus flares into the medial and lateral columns, which form a strong triangular construct supporting the articular segment—the trochlea medially and the capitellum laterally. The trochlea, a spool-shaped structure, articulates with the highly congruent greater sigmoid notch of the proximal ulna. Notably, the articular surface of the distal humerus is tilted approximately 30 degrees anterior to the longitudinal axis of the humeral shaft, a critical anatomical feature that allows for terminal flexion without the coronoid process impinging prematurely on the anterior humeral shaft.
The olecranon and coronoid fossae are critical anatomical landmarks for this procedure. These thin, diaphanous bony depressions are located immediately proximal to the trochlea on the posterior and anterior aspects of the distal humerus, respectively. They are separated by a thin wafer of bone known as the supratrochlear septum. During terminal extension, the tip of the olecranon process seats perfectly within the olecranon fossa; conversely, during terminal flexion, the coronoid process seats within the coronoid fossa. In the osteoarthritic elbow, these fossae become obliterated by osteophytic encroachment, and the corresponding processes become hypertrophied. The O-K procedure fundamentally relies on the precise, surgical fenestration of this supratrochlear septum, creating a transmural window that effectively deepens both fossae simultaneously and provides a portal for anterior joint debridement from a purely posterior surgical approach.
Neurovascular considerations in the posterior approach to the elbow are paramount, with the ulnar nerve demanding the highest degree of vigilance. The ulnar nerve courses distally through the posterior compartment of the arm, piercing the medial intermuscular septum to enter the cubital tunnel posterior to the medial epicondyle. It is tethered by the arcuate ligament (Osborne's fascia) and rests intimately against the posterior band of the medial ulnar collateral ligament. In up to 20% of patients with advanced elbow osteoarthritis, posterior and medial osteophytes can mechanically impinge upon the cubital tunnel, leading to compressive ulnar neuropathy. Consequently, meticulous identification, neurolysis, and protection of the ulnar nerve are obligatory steps in the surgical sequence. While the radial nerve and the median nerve are generally protected by the anterior musculature, aggressive anterior capsular release or uncontrolled advancement of instruments through the newly created supratrochlear fenestration can theoretically place these anterior neurovascular structures at catastrophic risk.
Exhaustive Indications and Contraindications
Patient selection is the cornerstone of achieving excellent clinical outcomes with the ulnohumeral arthroplasty. The ideal candidate is a highly motivated, high-demand patient—often a middle-aged male laborer or athlete—who presents with a chief complaint of impingement pain localized specifically to the extremes of flexion and extension. These patients typically demonstrate a well-preserved arc of mid-range motion and maintain functional, pain-free forearm rotation (pronation and supination), indicating relative sparing of the radiocapitellar and proximal radioulnar joints. Radiographic evaluation must definitively confirm the presence of hypertrophic osteophytes on the olecranon, coronoid, and within their respective fossae, correlating with the clinical mechanical blocks. Furthermore, the presence of symptomatic intra-articular loose bodies or concomitant, mechanically induced ulnar neuropathy strongly supports the indication for this comprehensive joint-preserving debridement.
Conversely, strict adherence to contraindications is vital to prevent surgical failures and patient dissatisfaction. The O-K procedure is fundamentally a debridement and decompression operation; it does not resurface the joint. Therefore, patients presenting with diffuse, severe pain throughout the entire arc of motion, indicative of global articular cartilage denudation, are poor candidates. Inflammatory arthropathies, such as rheumatoid arthritis, are absolute contraindications, as the primary pathology is synovial-driven cartilage destruction rather than mechanical impingement. Severe joint space narrowing on standard radiographs, significant architectural distortion from prior trauma, or profound multi-ligamentous instability also preclude this procedure. In such scenarios, total elbow arthroplasty or interpositional arthroplasty may represent more appropriate surgical algorithms, depending on the patient's age and functional demands.
Below is a comprehensive table delineating the strict indications and contraindications for the Outerbridge-Kashiwagi ulnohumeral arthroplasty:
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Primary Indications | Pain isolated to terminal flexion/extension | Indicates mechanical impingement rather than global articular wear. |
| Radiographic anterior/posterior osteophytes | Confirms the structural source of the mechanical block. | |
| Preserved radiocapitellar joint space | Ensures mid-arc motion and rotation will remain pain-free postoperatively. | |
| Presence of symptomatic loose bodies | Mechanical locking requires surgical extraction for symptom resolution. | |
| Relative Indications | Concomitant ulnar neuropathy | Can be addressed simultaneously via decompression/transposition during the posterior approach. |
| Mild capsular contracture | Can be addressed via limited capsular release through the fenestration. | |
| Absolute Contraindications | Inflammatory arthritis (e.g., Rheumatoid) | Global cartilage destruction will not be relieved by osteophyte resection. |
| Diffuse pain throughout the entire arc of motion | Indicates severe, end-stage joint degeneration requiring arthroplasty. | |
| Severe radiocapitellar osteoarthritis | Will result in persistent pain during pronation/supination postoperatively. | |
| Active joint infection | Requires eradication prior to any elective reconstructive or debridement procedure. | |
| Relative Contraindications | Gross elbow instability | Debridement and collateral ligament stripping may exacerbate instability. |
| Arc of motion less than 40 degrees | Suggests severe soft tissue contracture that bony debridement alone cannot correct. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with a rigorous radiographic evaluation. High-quality, orthogonal plain radiographs are the foundation of our assessment. A true anteroposterior (AP) view is essential for evaluating the medial and lateral joint spaces, the carrying angle, and the presence of medial or lateral osteophytes. The true lateral radiograph, taken with the elbow flexed at exactly 90 degrees, is arguably the most critical view. It allows for precise visualization of the hypertrophic osteophytes extending from the olecranon tip and the coronoid process, as well as the degree of encroachment within the olecranon and coronoid fossae. Oblique views can further delineate the radiocapitellar articulation and the medial epicondyle, ensuring no subtle pathology is missed.

FIG 1 • B. AP radiograph of the elbow. This view shows ossification and osteophytes of the olecranon and coronoid fossa.

FIG 1 • A. Lateral radiograph of a 50-year-old heavy laborer’s elbow. Note the characteristic osteophytes of the olecranon and of the coronoid process.
In the contemporary era of orthopedic surgery, advanced cross-sectional imaging has become an invaluable adjunct. A non-contrast Computed Tomography (CT) scan with three-dimensional (3D) reconstructions is highly recommended for preoperative templating. The CT scan provides unparalleled spatial resolution, allowing the surgeon to map the exact location, size, and morphology of all osteophytes and, crucially, to identify occult loose bodies hidden within the capsular recesses that might be obscured on plain radiographs. Furthermore, the CT scan helps assess the thickness of the medial and lateral columns of the distal humerus, ensuring that the planned supratrochlear fenestration will not inadvertently compromise the structural integrity of the distal humerus and precipitate a catastrophic supracondylar fracture.
Patient positioning is a critical logistical step that dictates the ease of surgical exposure and intraoperative fluoroscopic assessment. While the supine position with the arm draped across the chest is an option, the lateral decubitus position is widely considered the gold standard for the posterior approach to the elbow. The patient is placed in the lateral decubitus position on a well-padded beanbag, with all bony prominences meticulously protected. The operative arm is draped free and allowed to rest over a padded L-bar or a sterile stack of blankets, allowing the elbow to rest comfortably at 90 degrees of flexion. This setup allows gravity to assist in retracting the triceps and provides the surgeon with an unobstructed, ergonomic view of the posterior elbow compartment.

FIG 2 • With the patient in the lateral decubitus position, the elbow is flexed at 90 degrees and is resting on pillows. A posterior approach is used via a straight skin incision.
A sterile pneumatic tourniquet is applied high on the brachium. The arm is exsanguinated with an Esmarch bandage, and the tourniquet is inflated to standard upper extremity pressures (typically 250 mmHg). A bloodless field is absolutely essential for identifying subtle articular pathology, visualizing the ulnar nerve, and safely executing the transmural fenestration without inadvertently injuring anterior neurovascular structures. Intraoperative fluoroscopy must be positioned on the opposite side of the table, capable of swinging in to provide true AP and lateral views without requiring the surgical team to break sterility or reposition the patient's torso.
Step-by-Step Surgical Approach and Fixation Technique
Superficial Dissection and Triceps Management
The surgical approach begins with a generous, straight posterior longitudinal incision, centered over the olecranon. The incision typically originates 6 to 8 centimeters proximal to the tip of the olecranon and extends 4 to 6 centimeters distally along the subcutaneous border of the ulna. This straight incision avoids the medial and lateral epicondyles, minimizing the risk to cutaneous nerve branches, and provides an extensile window that can be expanded if necessary. Subcutaneous flaps are elevated full-thickness, taking care to preserve the superficial fascia, until the triceps tendon and the olecranon bursa are fully exposed. The olecranon bursa is routinely excised to prevent postoperative bursitis and to clarify the anatomical planes.

Intraoperative view of the initial triceps exposure.
Management of the extensor mechanism is the next critical juncture. For the standard O-K procedure, a triceps-splitting approach is highly effective and minimizes disruption to the extensor mechanism's continuity. A longitudinal incision is made sharply through the midline of the triceps fascia, muscle belly, and distal tendon, extending down to the tip of the olecranon. Using a periosteal elevator, the medial and lateral halves of the triceps are elevated subperiosteally off the posterior aspect of the distal humerus. This dissection must remain strictly on the bone to avoid intramuscular bleeding and to ensure a robust fascial layer remains for a secure closure.

Longitudinal splitting of the triceps tendon and muscle belly.
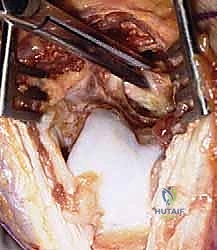
Once the triceps is elevated and retracted with self-retaining retractors (such as a Gelpi or Weitlaner), the posterior capsule of the elbow joint is exposed. In the setting of advanced osteoarthritis, the capsule is invariably thickened, fibrotic, and contracted. A transverse or crucial capsulotomy is performed to enter the joint space. Immediately upon entering the joint, the surgeon is typically confronted with hypertrophic osteophytes filling the olecranon fossa and prominent bony excrescences on the tip of the olecranon. Free loose bodies are frequently encountered at this stage and should be meticulously extracted and cataloged.
Ulnar Nerve Decompression and Protection
Before proceeding with any aggressive bony resection, the ulnar nerve must be definitively addressed. Even in the absence of preoperative cubital tunnel syndrome symptoms, the anatomical distortion caused by medial osteophytes mandates, at a minimum, in situ decompression and meticulous protection. The dissection is carried medially, identifying the medial epicondyle. The fascia of the flexor carpi ulnaris (Osborne's ligament) is incised, and the ulnar nerve is identified within the cubital tunnel.
Identification and neurolysis of the ulnar nerve.
The nerve is carefully neurolysed using vessel loops for gentle retraction. If the patient had preoperative ulnar neuropathy, or if the medial osteophytes are so massive that their removal would jeopardize the nerve, a formal anterior transposition (subcutaneous or submuscular, based on surgeon preference and patient anatomy) is performed. If the nerve is to remain in situ, it must be continuously protected with a malleable retractor throughout the remainder of the procedure, particularly during the use of high-speed burrs or osteotomes near the medial column.
Failure to adequately protect the ulnar nerve is the most common source of catastrophic iatrogenic complication in this procedure. The surgeon must maintain constant situational awareness of the nerve's location. The medial column of the distal humerus must be cleared of osteophytes carefully, often using rongeurs or hand curettes rather than power instruments, to prevent thermal or direct mechanical injury to the adjacent neural structures.
Posterior Osteophyte Resection and The Ulnohumeral Fenestration
With the posterior compartment exposed and the ulnar nerve protected, attention is turned to the bony debridement. The first step is the resection of the olecranon tip osteophytes. Using a sharp, curved osteotome or a high-speed burr, the hypertrophic bone on the proximal aspect of the olecranon is excised, restoring the normal contour of the greater sigmoid notch. Next, the osteophytes surrounding the margins of the olecranon fossa are cleared, delineating the true anatomical boundaries of the fossa and the medial/lateral columns.

Resection of posterior osteophytes from the olecranon fossa.
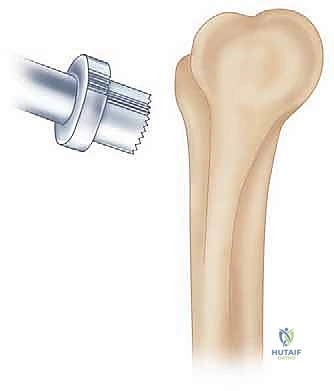
The defining step of the Outerbridge-Kashiwagi procedure is the creation of the supratrochlear fenestration. This is achieved by trephining the thin cortical bone separating the olecranon and coronoid fossae. A specialized trephine (typically 15mm to 20mm in diameter, depending on the patient's size) or a high-speed burr is utilized. The instrument is centered perfectly within the olecranon fossa, aiming slightly distally and anteriorly, perpendicular to the anterior humeral cortex.

Creation of the supratrochlear fenestration using a burr.
It is absolutely critical to maintain the structural integrity of the medial and lateral columns during this step. The fenestration must not exceed the width of the native fossa, as excessive bone removal can precipitate a postoperative supracondylar fracture. Once the anterior cortex is breached, the window is widened and smoothed using a Kerrison rongeur or a spherical burr. This newly created portal provides direct, albeit restricted, visual and instrumental access to the anterior compartment of the elbow joint.
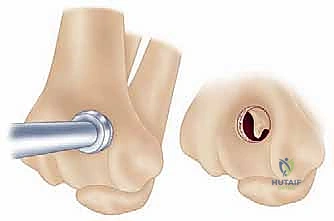
The completed ulnohumeral fenestration, providing access to the anterior compartment.
Anterior Debridement and Dynamic Assessment
Through the supratrochlear fenestration, the surgeon can now address the anterior pathology. By flexing the elbow, the coronoid process is brought into view within the window. Using pituitary rongeurs, angled curettes, and specialized arthroscopic burrs passed through the open posterior incision, the osteophytes on the tip of the coronoid process and within the coronoid fossa are meticulously resected.
Resection of anterior osteophytes on the coronoid process through the fenestration.

Using rongeurs to extract loose bodies and debris from the anterior capsule.
The anterior capsule, which is often severely contracted and contributes to the loss of extension, can also be addressed through this window. Using a blunt elevator or a carefully manipulated scalpel, the capsule can be elevated off the anterior aspect of the distal humerus, effectively releasing the contracture. This step requires extreme caution, as the brachial artery and median nerve lie immediately anterior to the capsule. Aggressive or blind plunging with sharp instruments must be strictly avoided.

Careful anterior capsular release through the fenestration.
Once all accessible osteophytes and loose bodies have been removed from both compartments, the joint is thoroughly irrigated to remove bone debris. A dynamic assessment of the range of motion is then performed. The elbow is taken through a full arc of flexion and extension. The surgeon should observe smooth tracking of the olecranon and coronoid into their respective, newly deepened fossae, without any residual bony impingement. If a mechanical block persists, further targeted debridement is required. Fluoroscopy is utilized at this stage to confirm the complete removal of osteophytes and to verify that no radiopaque loose bodies remain hidden in the recesses.
Dynamic assessment of terminal flexion.

Dynamic assessment of terminal extension, ensuring the olecranon seats freely in the fenestration.
Following satisfactory dynamic assessment and fluoroscopic confirmation, meticulous hemostasis is achieved. The tourniquet is deflated prior to closure to ensure no active bleeding points remain, particularly from the muscle bellies or periosteal vessels. A medium-sized intra-articular drain is routinely placed to prevent postoperative hematoma formation, which can lead to severe pain, restricted motion, and increased risk of heterotopic ossification. The triceps split is repaired with heavy, non-absorbable sutures in an interrupted fashion, ensuring a robust, watertight closure of the extensor mechanism. The subcutaneous tissues and skin are closed meticulously, and a well-padded, bulky compressive dressing is applied with the elbow in extension to minimize bleeding and dead space.
Complications, Incidence Rates, and Salvage Management
While the Outerbridge-Kashiwagi arthroplasty is highly effective, it is a major joint-altering procedure that carries a specific profile of potential complications. A thorough understanding of these risks is essential for informed patient consent and for implementing intraoperative strategies to mitigate them. The most common and concerning complication is postoperative ulnar neuropathy. Even with meticulous protection or formal transposition, the nerve can become irritated due to traction, postoperative hematoma, or perineural fibrosis. The incidence of transient ulnar nerve symptoms ranges from 5% to 10%, though permanent motor or sensory deficits are rare if the nerve was handled delicately.
Heterotopic ossification (HO) is another significant risk, given the extensive bony resection and capsular stripping involved. The inflammatory response generated by bone dust and soft tissue trauma can stimulate ectopic bone formation, which can severely compromise the hard-won range of motion and lead to recurrent impingement. The incidence of clinically significant HO varies but can be up to 10% in high-risk individuals. Prophylactic measures, discussed in the rehabilitation section, are critical to minimizing this risk.
A catastrophic, though thankfully rare, complication is the iatrogenic fracture of the distal humerus, specifically a supracondylar fracture through the level of the fenestration. This occurs if the surgeon over-widens the supratrochlear window, excessively thinning the medial and lateral columns. The incidence is less than 1%, but the consequences
