Arthroscopic Olecranon Osteophyte Resection Guide
Key Takeaway
Valgus extension overload syndrome frequently results in the formation of posterior olecranon osteophytes, causing posterior impingement and pain in overhead athletes. Arthroscopic resection involves meticulous visualization of the posterior compartment, identification of the impinging osteophyte, and precise burring of 2 to 3 mm of the olecranon tip. This restores terminal extension while preserving the critical stabilizing anatomy of the ulnohumeral articulation.
Comprehensive Introduction and Patho-Epidemiology
Posterior elbow impingement, frequently manifesting as Valgus Extension Overload (VEO) syndrome, is a well-documented and biomechanically complex clinical entity primarily affecting overhead athletes. This demographic includes baseball pitchers, javelin throwers, tennis players, and collegiate volleyball attackers. The repetitive, high-velocity valgus stress applied to the elbow during the late cocking and early acceleration phases of throwing generates profound compressive forces across the radiocapitellar joint and the posteromedial ulnohumeral articulation. Simultaneously, massive tensile forces are imparted upon the medial ligamentous structures. This dichotomous force distribution creates a unique microenvironment for pathological bone formation and capsular derangement, fundamentally altering the functional anatomy of the throwing elbow.
Over time, this repetitive microtrauma leads to the formation of reactive osteophytes at the posteromedial tip of the olecranon. According to Wolff’s Law, the bone remodels in response to the cyclical compressive loads and sheer stresses encountered as the olecranon is forcefully wedged into the olecranon fossa during terminal extension. As the elbow is forced into this terminal extension during the deceleration and follow-through phases of the throwing motion, these hypertrophic osteophytes impinge within the olecranon fossa. This repetitive abutment results in localized chondromalacia, fragmentation of the osteophytes leading to intra-articular loose body formation, and debilitating posterior elbow pain that sharply limits athletic performance.
Furthermore, the chronic inflammatory response elicited by this mechanical impingement frequently leads to profound capsular hypertrophy. A thickened posterolateral capsule—specifically a radiocapitellar plica—can become fibrotic and interpose within the joint. This fibrotic band acts as a space-occupying lesion within the tight confines of the radiocapitellar articulation, causing mechanical symptoms such as snapping, catching, or popping during active extension. Epidemiologically, VEO and associated posteromedial impingement are ubiquitous in professional and elite amateur baseball pitchers, with studies indicating that nearly all collegiate and professional pitchers exhibit some degree of asymptomatic olecranon remodeling.
The transition from asymptomatic adaptation to symptomatic pathology usually occurs in the late teens to early twenties, correlating with increases in throwing velocity and cumulative pitch counts. The incidence of surgical intervention for VEO has risen concurrently with the overall increase in elbow injuries in overhead athletes. Understanding the patho-epidemiology of this condition requires an appreciation of the entire kinetic chain; deficits in core stability, scapular dyskinesia, or premature trunk rotation frequently exacerbate the valgus torque at the elbow, accelerating the onset of VEO. Consequently, the orthopedic surgeon must view the osteophyte not merely as an isolated bony anomaly, but as the terminal manifestation of a profound biomechanical overload syndrome.
Detailed Surgical Anatomy and Biomechanics
A rigorous understanding of ulnohumeral and radiocapitellar biomechanics is the cornerstone of safe and effective arthroscopic intervention in the elbow. The osseous anatomy of the elbow joint provides substantial inherent stability, particularly in extension. The ulnohumeral joint acts as a highly constrained hinge, where the greater sigmoid notch of the ulna articulates with the trochlea of the distal humerus. In terminal extension, the tip of the olecranon process seats intimately within the olecranon fossa of the posterior humerus. This bony congruency is not merely for articulation; it serves as a critical secondary restraint to valgus stress. When the elbow is fully extended, the olecranon engaged in its fossa provides up to 30% of the resistance to valgus torque.
The primary restraint to valgus stress is the Medial Ulnar Collateral Ligament (MUCL) complex, specifically the anterior bundle. The anterior bundle originates from the anteroinferior surface of the medial epicondyle and inserts onto the sublime tubercle of the proximal ulna. During the throwing motion, particularly during the late cocking and acceleration phases where the elbow is flexed between 90 and 120 degrees, the anterior bundle of the MUCL is subjected to forces approaching its ultimate tensile failure strength. If the MUCL becomes attenuated through repetitive microtrauma, the resultant microinstability shifts the burden of valgus restraint heavily onto the radiocapitellar joint (causing compressive chondral damage) and the posteromedial olecranon (causing reactive osteophytosis).
The neurovascular anatomy surrounding the elbow dictates the safe zones for arthroscopic portal placement. The ulnar nerve courses posterior to the medial epicondyle within the cubital tunnel and is at extreme risk during the establishment of posteromedial portals or during aggressive osseous resection in the posteromedial gutter. The radial nerve, traversing anterior to the lateral epicondyle and dividing into the posterior interosseous nerve and superficial radial nerve, is the primary structure at risk during anterolateral portal placement. The median nerve and brachial artery lie centrally in the anterior compartment, protected by the brachialis muscle, but remain vulnerable to aberrant trocar insertion or excessive fluid extravasation leading to compartment syndrome.
Biomechanically, the throwing motion is a kinetic chain that transfers energy from the lower extremities, through the core, and into the upper extremity. The elbow acts as a funnel for this kinetic energy. Any breakdown in the proximal kinetic chain forces the shoulder and elbow to generate compensatory torque. In the context of VEO, the posteromedial olecranon osteophyte is a direct biomechanical consequence of valgus torque combined with rapid extension. Therefore, the surgeon must recognize that resecting the osteophyte alters the biomechanical equilibrium of the joint. The olecranon tip must be preserved to maintain its function as a secondary valgus restraint; over-resection dramatically increases the strain on the anterior bundle of the MUCL, potentially precipitating catastrophic ligamentous failure.
Exhaustive Indications and Contraindications
The decision to proceed with arthroscopic resection of an olecranon osteophyte must be predicated on a meticulous clinical evaluation and a documented failure of comprehensive conservative management. Initial management of posterior elbow impingement and plica syndrome should universally be non-operative, spanning a minimum of three to six months. This regimen includes scheduled pharmacotherapy (NSAIDs), strict cessation of the offending athletic activity, and a highly structured physical therapy program focusing on the kinetic chain, flexor-pronator mass strengthening, and periscapular stabilization. Intra-articular corticosteroid injections may be utilized for both diagnostic confirmation and therapeutic relief, though their use in young athletes should be judicious to avoid chondral toxicity.
Surgical intervention is explicitly indicated when a patient experiences persistent, activity-limiting posteromedial or posterolateral elbow pain, accompanied by mechanical symptoms such as catching or locking, that entirely precludes their return to sport despite exhaustive non-operative measures. Clinically, these patients will demonstrate a positive valgus extension overload test (pain elicited by forced terminal extension while a valgus stress is applied). Radiographic indications include definitive evidence of impinging posteromedial osteophytes on axial and lateral plain films, the presence of intra-articular loose bodies, or MRI evidence of a pathological radiocapitellar plica (capsular thickening >3 mm) with associated focal chondromalacia in the posterolateral compartment.
Contraindications to arthroscopic olecranon osteophyte resection are equally critical to define. Absolute contraindications include active local or systemic infection, severe advanced osteoarthritis of the ulnohumeral joint (where isolated osteophyte resection will not reliably relieve generalized arthritic pain and may destabilize the joint), and an inability to comply with strict postoperative rehabilitation protocols. A critical relative contraindication—and a frequent pitfall in sports medicine—is the presence of concurrent, symptomatic MUCL insufficiency. Performing an isolated olecranon osteophyte resection in a patient with an incompetent MUCL will exacerbate valgus instability, rapidly accelerating joint degeneration and leading to a swift return of symptoms. In such cases, concurrent MUCL reconstruction (Tommy John surgery) must be performed.
Below is a comprehensive table detailing the clinical decision-making matrix for this procedure:
| Category | Specific Criteria | Clinical Rationale / Impact |
|---|---|---|
| Primary Indications | Failure of 3-6 months conservative therapy | Ensures natural healing potential is exhausted before altering joint biomechanics. |
| Primary Indications | Positive Valgus Extension Overload test | Confirms mechanical abutment of the olecranon within the fossa during functional arcs. |
| Radiographic Indications | Symptomatic loose bodies / Osteophytes >3mm | Direct mechanical blocks to extension requiring physical extraction and decompression. |
| Absolute Contraindications | Active joint infection / Cellulitis | Risk of systemic sepsis and catastrophic joint destruction. |
| Absolute Contraindications | Advanced global ulnohumeral osteoarthritis | Resection fails to address global chondral loss; alters joint kinematics negatively. |
| Relative Contraindications | Concomitant MUCL Insufficiency | Isolated resection removes secondary valgus restraint, worsening instability unless MUCL is reconstructed. |
| Relative Contraindications | Ulnar nerve subluxation with severe neuritis | May require concurrent ulnar nerve transposition to address neurological symptoms safely. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for arthroscopic olecranon resection requires a rigorous, multi-modal imaging review to precisely define the pathological anatomy and template the surgical resection. Standard anteroposterior (AP), lateral, and axial (flexed to 110 degrees) radiographs are mandatory. The axial view is paramount for visualizing the posteromedial olecranon osteophyte and identifying loose bodies sequestered within the depths of the olecranon fossa. The surgeon must meticulously measure the dimensions of the osteophyte on the lateral radiograph. This templating is critical: the goal is to define the exact millimeter depth of the pathological bone to ensure that resection is strictly limited to the osteophyte (typically 2 to 3 mm) while preserving the native olecranon contour.
Magnetic Resonance Imaging (MRI) or MR arthrography is indispensable for evaluating the integrity of the MUCL, assessing the extent of chondral damage (particularly capitellar osteochondritis dissecans, which frequently co-occurs with VEO), and identifying a pathological posterolateral plica. The surgeon must scrutinize the T2-weighted axial and coronal sequences to rule out partial-thickness tears of the anterior bundle of the MUCL. If the MUCL is compromised, the pre-operative plan must be drastically altered to include ligamentous reconstruction, and the patient must be counseled accordingly. Furthermore, the pre-operative physical examination under anesthesia (EUA) is a critical step to dynamically assess valgus laxity before the skin is incised.
Patient positioning and anesthesia are foundational to the success of the procedure. The operation is typically performed under general anesthesia, supplemented by a regional block (supraclavicular or axillary) to minimize volatile anesthetic requirements and provide robust postoperative analgesia. While the supine suspended position and lateral decubitus position are viable, the prone position is widely considered optimal for procedures focusing heavily on the posterior compartment, such as VEO decompression. In the prone position, the arm is draped over a well-padded arm board, allowing the elbow to rest at 90 degrees of flexion with gravity assisting in joint distraction. This position provides unparalleled, unobstructed access to the posterior compartment, the olecranon fossa, and the posteromedial gutter.
Operating room setup must be meticulously orchestrated. A non-sterile tourniquet is applied high on the brachium, though its inflation is often reserved for cases where visualization is severely compromised by bleeding, as routine inflation can tether the capsule and increase the risk of neuropraxia. Fluid management is critical; an automated pump system is utilized, but pressures must be strictly maintained between 30 and 40 mmHg to prevent massive fluid extravasation into the fascial compartments of the forearm, which can rapidly lead to compartment syndrome. The surgical team must ensure that all specialized arthroscopic equipment, including 4.0-mm hooded burrs, small joint osteotomes, and radiofrequency ablation wands, are readily available before the diagnostic arthroscopy commences.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of an arthroscopic olecranon osteophyte resection demands meticulous technique, precise portal placement, and a profound respect for the surrounding neurovascular structures. While the primary goal is resection, the "fixation technique" in this context refers to the stabilization of the joint environment, including the management and potential fixation of concomitant osteochondral lesions (e.g., capitellar OCD) that frequently present in the overhead athlete. The procedure begins with a systematic evaluation of the anterior compartment. The joint is insufflated with 20 to 30 mL of normal saline via the soft spot to distend the capsule and displace the anterior neurovascular bundle safely away from the joint line.
The proximal anterolateral portal is established first, utilizing a superficial skin incision followed by blunt dissection with a mosquito hemostat down to the capsule to protect the radial nerve. The arthroscope is introduced, and an anteromedial portal is established under direct intra-articular visualization using an outside-in spinal needle localization technique, ensuring a safe distance from the medial antebrachial cutaneous nerve. A thorough diagnostic sweep of the anterior radiocapitellar and ulnohumeral joints is performed. Any anterior loose bodies are extracted, and anterior capsular adhesions are released if a pre-operative flexion contracture was identified. Once the anterior compartment is cleared, the arthroscope is removed, and attention is directed to the posterior compartment.
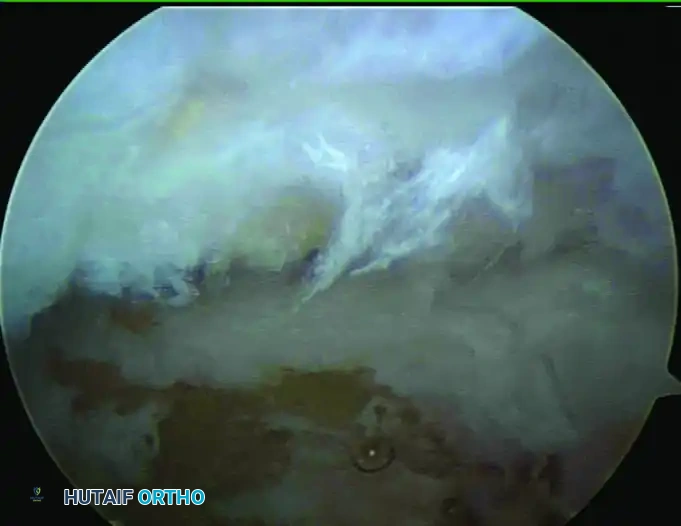
Establishing the posterior portals requires precision. The posterolateral portal is placed 2 to 3 cm proximal to the olecranon tip, just lateral to the triceps border, serving as the primary viewing portal. The direct posterior (trans-triceps) portal is established 3 cm proximal to the olecranon tip in the midline, serving as the primary working portal. A 4.0-mm motorized shaver is introduced to clear the olecranon fossa of fibrotic tissue, hypertrophic synovium, and any hidden loose bodies. The elbow is then dynamically brought into varying degrees of extension to directly observe the impingement of the olecranon tip against the fossa. The pathological osteophyte will manifest as a prominent osseous ridge at the superior and posteromedial aspect of the olecranon.
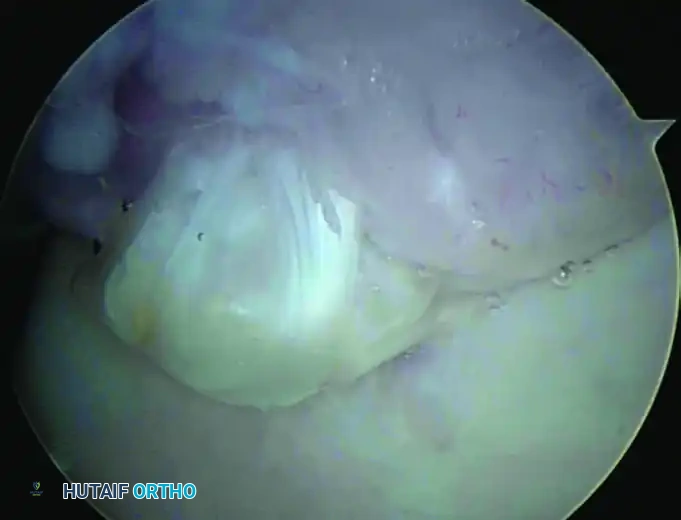
Resection is initiated using a 4.0-mm hooded arthroscopic burr. The hood of the burr must always be oriented towards the soft tissues (triceps and posterior capsule) to prevent iatrogenic soft tissue damage. The surgeon meticulously burrs away the osteophyte, strictly adhering to the pre-operative template. Crucial Technical Pearl: No more than 2 to 3 mm of bone should be removed. The resection must restore the normal anatomical contour of the olecranon without violating the native articular congruency. If concomitant capitellar OCD lesions are identified during the diagnostic sweep, the fixation technique involves either debridement and microfracture for small lesions, or the use of bioabsorbable pins/osteochondral autograft transfer (OATS) for larger, unstable fragments.
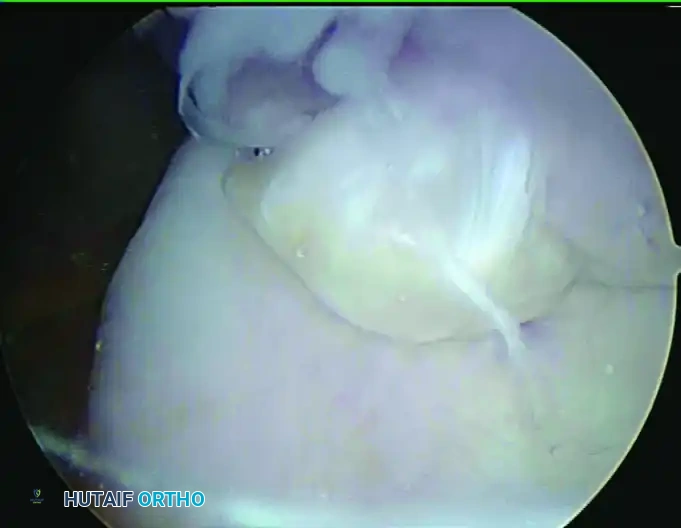
Following the osseous resection, the elbow is again dynamically tested in terminal extension to confirm that impingement has been completely eradicated and that the newly contoured olecranon seats smoothly within the fossa. If full-thickness chondral defects are present in the olecranon fossa due to chronic abutment, an arthroscopic awl is used to perform microfracture, penetrating the subchondral bone to a depth of 2 to 3 mm to stimulate a fibrocartilage healing response. The joint is then copiously irrigated with several liters of saline to evacuate all bone debris, minimizing the risk of heterotopic ossification. The portals are closed with non-absorbable sutures, and a bulky, sterile compressive dressing is applied to control postoperative hemarthrosis.
Complications, Incidence Rates, and Salvage Management
While arthroscopic resection of olecranon osteophytes is a highly successful intervention when executed correctly, the procedure carries specific, potentially career-ending risks for the overhead athlete. The most devastating complication specific to this procedure is iatrogenic valgus instability. The olecranon tip provides critical resistance to valgus stress when the elbow is extended. Resecting more than 3 to 4 mm of the olecranon tip exponentially increases the tension on the anterior band of the MUCL. In a high-velocity throwing athlete, this loss of secondary bony restraint can rapidly lead to MUCL attenuation and catastrophic failure. The incidence of iatrogenic instability is directly correlated with the depth of resection and the surgeon's failure to recognize pre-existing, subtle MUCL laxity.
Neurological injury is a significant concern during elbow arthroscopy. The ulnar nerve is highly vulnerable during posterior and posteromedial portal placement, as well as during aggressive burring in the posteromedial gutter. Transient ulnar neuropraxia occurs in approximately 2% to 5% of cases and is typically secondary to massive fluid extravasation compressing the cubital tunnel, or direct thermal/mechanical trauma from instruments. Strict adherence to anatomical landmarks, the use of blunt dissection techniques for portal entry, and meticulous fluid pressure management (keeping pump pressures <40 mmHg) are mandatory to mitigate this risk.
Heterotopic Ossification (HO) and post-operative arthrofibrosis are complications arising from inadequate joint irrigation and prolonged immobilization, respectively. Bone debris generated by the motorized burr can act as a nidus for HO within the posterior capsule or triceps tendon. Copious, high-volume lavage at the conclusion of the procedure is essential. In patients with a history of hypertrophic bone formation, a short postoperative course of NSAIDs (e.g., Indomethacin) or a single dose of localized radiation therapy may be considered as prophylaxis. Incomplete resection of the osteophyte is another frequent pitfall, resulting in persistent mechanical symptoms and pain, ultimately requiring revision arthroscopy.
Salvage management for these complications is complex and requires advanced reconstructive skills. If iatrogenic MUCL failure occurs due to over-resection, the patient will require a formal MUCL reconstruction (Tommy John surgery) using an autograft (e.g., palmaris longus or gracilis). If severe HO develops and drastically limits range of motion, an open or arthroscopic capsular release with excision of the heterotopic bone is indicated, typically delayed until the bone is metabolically mature (at least 6 months post-operatively).
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Iatrogenic Valgus Instability | 1% - 3% (Higher in elite throwers) | Limit resection strictly to <3mm; pre-op MRI evaluation of MUCL. | MUCL Reconstruction (Tommy John Surgery) with structured 12-18 month rehab. |
| Ulnar Neuropraxia | 2% - 5% | Blunt dissection; limit fluid pressure <40 mmHg; avoid medial suction. | Observation (most resolve in 6-12 weeks); neurolysis/transposition if persistent. |
| Heterotopic Ossification (HO) | 3% - 7% | Copious joint lavage post-burring; meticulous hemostasis. | Indomethacin prophylaxis; delayed surgical excision and capsular release if symptomatic. |
| Incomplete Resection | 4% - 8% | Dynamic intraoperative testing in terminal extension under direct visualization. | Revision arthroscopic decompression and osteophyte resection. |
| Fluid Extravasation / Compartment Syndrome | < 1% | Monitor forearm tension; use outflow portals; limit surgical time. | Immediate cessation of procedure; emergent fasciotomy if pressures remain critically elevated. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following arthroscopic olecranon osteophyte resection is highly structured, phased, and must be individually tailored to the specific procedures performed, particularly if concomitant microfracture or OCD fixation was required. The overarching goal of rehabilitation is to restore full, symmetric range of motion (ROM) rapidly while protecting the healing articular surfaces and gradually rebuilding the kinetic chain required for overhead sports. Communication between the orthopedic surgeon, physical therapist, and athletic trainer is paramount to navigate the athlete safely through these phases.
Phase I: Immediate Postoperative Phase (Days 1-14)
The primary objectives of Phase I are to control inflammation, minimize hemarthrosis, and prevent arthrofibrosis, which the elbow is notoriously prone to developing. The arm is placed in a sling for comfort only; rigid immobilization is strictly avoided. Active and active-assisted ROM exercises for the elbow, wrist, and hand are initiated on postoperative day 1 or 2. The patient is instructed to perform multiple short sessions of ROM daily. Cryotherapy and elevation are utilized aggressively. If an isolated osteophyte resection was performed, weight-bearing as tolerated for daily activities is permitted. However, if microfracture of the olecranon fossa was performed, weight-bearing through the upper extremity is strictly restricted for 4 to 6 weeks to protect the maturing fibrocartilage clot, though early ROM remains critical to stimulate appropriate collagen alignment.
Phase II: Intermediate Strengthening Phase (Weeks 2-6)
Progression to Phase II is contingent upon the achievement of nearly full, painless ROM and the resolution of acute postoperative effusion. The focus shifts to progressive isotonic strengthening of the entire upper extremity musculature. Specific emphasis is placed on the flexor-pronator mass, which serves as an active dynamic restraint to valgus stress, thereby protecting the MUCL. Strengthening of the biceps, triceps, and wrist flexors/extensors is advanced using resistance bands and light free weights. Crucially, integration of periscapular and core strengthening is initiated early in this phase. Scapular dyskinesia is a primary contributor to altered elbow mechanics in throwers; ensuring proper scapular retraction and depression is vital to optimizing the kinetic chain before throwing resumes.
Phase III: Advanced Strengthening and Return to Sport (Weeks 6-12+)
Phase III involves the introduction of sport-specific biomechanics and high-level dynamic stabilization. Upper extremity plyometric exercises (e.g., medicine ball chest passes, plyometric push-ups) are introduced to train the stretch-shortening cycle of the musculature. For throwing athletes, a highly structured, progressive interval throwing program (ITP) is initiated typically around week 8 to 10. Entry into the ITP requires full, painless ROM, normal symmetric strength (5/5 on manual muscle testing), and absolutely no localized tenderness over the posteromedial olecranon or MUCL.
The ITP begins with short-distance, flat-ground throwing and progressively increases in distance, volume, and eventually velocity. Pitchers will transition to mound throwing only after successfully completing the flat-ground phases without symptom exacerbation. Unrestricted return to competitive overhead sports is typically achieved between 3 to 5 months postoperatively. This timeline is heavily dependent on the athlete passing rigorous, sport-specific functional testing, demonstrating flawless throwing mechanics, and exhibiting no signs of compensatory movement patterns that could predispose them to recurrent injury.
Summary of Landmark Literature and Clinical Guidelines
The evolution of arthroscopic management for Valgus Extension Overload and posteromedial impingement is deeply rooted in landmark biomechanical and clinical studies. The original descriptions of VEO by Andrews and colleagues in the 1980s fundamentally shifted the orthopedic community's understanding of posterior elbow pain in throwers. They elegantly described the triad of posteromedial olecranon osteophytes, radiocapitellar chondromalacia, and MUCL attenuation, establishing that the osteophyte was a symptom of a larger biomechanical derangement rather than an isolated pathology. This foundational work paved the way for joint-preserving arthroscopic techniques.
Biomechanical literature has heavily influenced the technical execution of this procedure. Landmark cadaveric studies by Fleisig, Kamineni, and Morrey meticulously quantified the role of the olecranon as a secondary valgus restraint. Their research demonstrated that resecting more than 3 mm of the posteromedial olecranon tip results in a non-linear, exponential increase in strain on the anterior bundle of the MUCL. These studies are the scientific basis for the universal surgical guideline emphasizing minimal, precise resection. Surgeons who ignore these biomechanical thresholds routinely face high rates of iatrogenic MUCL failure in their athletic patient populations.
Clinical outcomes literature consistently demonstrates high rates of success and return to play following isolated arthroscopic osteophyte resection in appropriately selected patients. Studies evaluating professional baseball pitchers have shown that over 85% of athletes return to their pre-injury level of competition, provided the MUCL is intact. However, literature also highlights the high revision rate in patients where subtle MUCL insufficiency was missed pre-operatively. Andrews and Cain's expansive retrospective reviews have shown that pitchers requiring concurrent MUCL reconstruction and olecranon resection have significantly longer recovery times but ultimately achieve stable, pain-free elbows.
Current consensus guidelines from organizations such as the American Shoulder and Elbow Surgeons (ASES) and the American Orthopaedic Society for Sports Medicine (AOSSM) heavily emphasize a comprehensive diagnostic approach. Guidelines dictate that MRI or MR arthrography is a mandatory pre-operative prerequisite to evaluate ligamentous integrity before any bone resection is undertaken. Furthermore, clinical guidelines stress that post-operative rehabilitation must focus on the entire kinetic chain, recognizing that isolated elbow therapy is insufficient for the overhead athlete. The integration of biomechanical analysis, precise arthroscopic technique, and holistic rehabilitation remains the gold standard for managing VEO in the modern sports medicine paradigm.
