Comprehensive Guide to Elbow Arthroscopy: Portal Placement and Surgical Anatomy
Key Takeaway
Safe and effective elbow arthroscopy relies on precise portal placement and a thorough understanding of periarticular neurovascular anatomy. By maximizing joint distention and maintaining 90 degrees of elbow flexion, surgeons can safely displace the radial and median nerves. This guide details the establishment of lateral, medial, and posterior portals, emphasizing step-by-step techniques, anatomical landmarks, and critical pearls to minimize complications and optimize intraarticular visualization.
Comprehensive Introduction and Patho-Epidemiology
Elbow arthroscopy has evolved from a nascent, highly experimental diagnostic modality into a sophisticated, indispensable therapeutic cornerstone within modern orthopedic surgery. Historically, the tightly encapsulated nature of the elbow joint, coupled with its dense, unforgiving surrounding neurovascular topography, rendered arthroscopic intervention a formidable challenge fraught with unacceptable complication rates. However, with the advent of specialized small-joint instrumentation, high-definition fiber-optic visualization, and a rigorously refined understanding of periarticular surgical anatomy, the indications for elbow arthroscopy have expanded exponentially. Today, it is recognized as the gold standard for addressing a myriad of intra-articular pathologies, offering the distinct advantages of minimized soft-tissue morbidity, accelerated rehabilitation, and superior visualization of complex articular recesses that are otherwise inaccessible via traditional open arthrotomies.
The patho-epidemiology of conditions amenable to arthroscopic intervention spans a broad demographic spectrum, affecting both the developing adolescent athlete and the aging degenerative patient. In the overhead throwing athlete, repetitive valgus extension overload syndromes frequently precipitate posteromedial osteophyte formation, chondromalacia, and the generation of intra-articular loose bodies. Conversely, the adolescent gymnast or baseball pitcher may present with osteochondritis dissecans (OCD) of the capitellum, necessitating arthroscopic debridement, marrow stimulation, or osteochondral fragment fixation. In the adult population, primary osteoarthritis and inflammatory arthropathies such as rheumatoid arthritis are highly prevalent, driving the need for arthroscopic osteocapsular arthroplasty, extensive synovectomy, and capsular release for severe arthrofibrosis. Furthermore, the management of lateral epicondylitis (tennis elbow) has seen a paradigm shift, with arthroscopic resection of the extensor carpi radialis brevis (ECRB) origin demonstrating exceptional clinical efficacy.
Despite its widespread adoption, elbow arthroscopy remains a technically demanding procedure that mandates a profound, three-dimensional spatial awareness. Unlike the knee or the shoulder, where the primary working spaces are relatively expansive and forgiving, the elbow joint possesses a maximal capsular capacity of merely 25 to 30 milliliters under optimal distention. The margin for error is measured in absolute millimeters. The radial, median, and ulnar nerves, along with the brachial artery, intimately invest the joint capsule, rendering them highly susceptible to iatrogenic injury during portal establishment or instrument manipulation. Consequently, the safe execution of this procedure is predicated upon an uncompromising adherence to established protocols regarding patient positioning, meticulous portal placement, and dynamic intra-articular fluid management.
This comprehensive textbook chapter serves as a definitive, evidence-based reference for the postgraduate orthopedic surgeon, detailing the intricate surgical anatomy, biomechanics of neurovascular displacement, and step-by-step methodologies required to master elbow arthroscopy. Through a rigorous examination of the lateral, medial, and posterior portal trajectories, this text aims to mitigate the steep learning curve associated with this advanced surgical discipline, ensuring optimal patient outcomes while minimizing the risk of catastrophic neurovascular complications.
Detailed Surgical Anatomy and Biomechanics
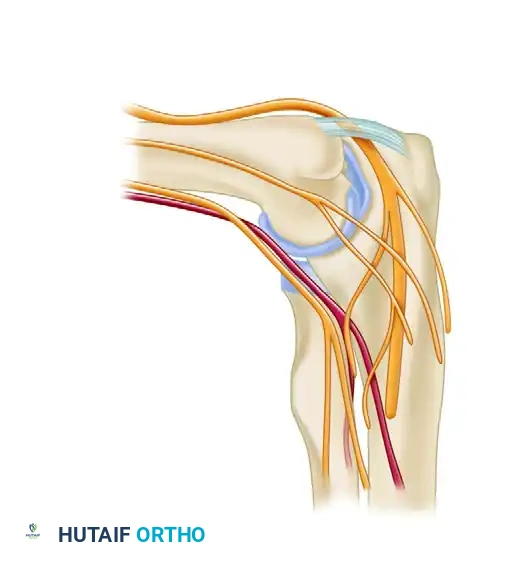
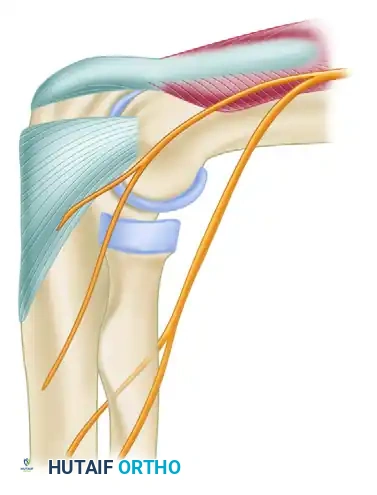
A masterful command of elbow arthroscopy is entirely dependent upon an intimate, unyielding knowledge of the periarticular neurovascular anatomy and the dynamic biomechanical alterations that occur during joint manipulation. The elbow is a highly congruent, complex hinge joint comprising three distinct articulations—the ulnohumeral, radiocapitellar, and proximal radioulnar joints—all enclosed within a single, continuous synovial capsule. The surrounding neurovascular structures traverse specific anatomical pathways that dictate the precise location and trajectory of every arthroscopic portal.
The anterior compartment is arguably the most treacherous anatomical zone. The brachial artery and the median nerve descend into the antecubital fossa, lying directly anterior to the brachialis muscle and the anterior joint capsule. In full extension, the brachialis muscle offers minimal protective cushioning, and these vital structures rest precariously close to the articular surface. The radial nerve, after piercing the lateral intermuscular septum, courses anterior to the lateral epicondyle between the brachialis and the brachioradialis before bifurcating into the superficial sensory branch and the deep posterior interosseous nerve (PIN). The PIN wraps around the radial neck, passing through the arcade of Frohse, placing it at significant risk during anterolateral portal placement or extensive anterolateral capsular releases.

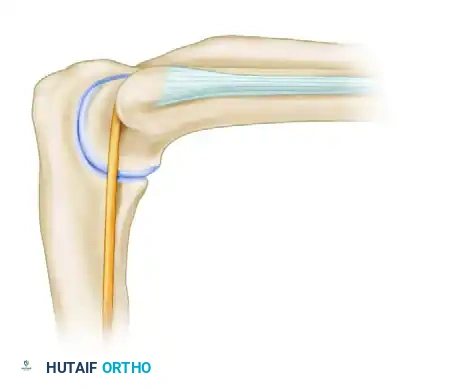
The medial compartment is dominated by the ulnar nerve and the medial antebrachial cutaneous nerve. The ulnar nerve resides within the cubital tunnel, posterior to the medial epicondyle, tightly bound by the Osborne ligament and the arcuate ligament of the flexor carpi ulnaris. Its proximity to the posteromedial capsule makes it highly vulnerable during posteromedial osteophyte resection or posterior portal establishment if instruments deviate medially. The medial antebrachial cutaneous nerve courses superficially along the anteromedial aspect of the elbow, frequently accompanying the basilic vein. These superficial structures are at extreme risk during the creation of the anteromedial portal, necessitating meticulous superficial dissection techniques.
The biomechanics of neurovascular displacement form the foundational safety mechanism in elbow arthroscopy. The fundamental principle is to maximize the distance between the joint capsule and the traversing nerves. This is achieved through a synergistic combination of precise joint flexion and maximal intra-articular fluid distention. When the elbow is flexed to exactly 90 degrees, the anterior capsule relaxes, and the brachialis muscle acts as a dynamic retractor, elevating the median nerve, radial nerve, and brachial artery away from the joint line. However, flexion alone is insufficient.
The critical second component is maximal capsular distention. In a resting, non-distended state, the capacity of the elbow joint is approximately 10 to 15 milliliters. By forcefully injecting 20 to 30 milliliters of fluid, the anterior capsule balloons outward. Landmark cadaveric studies have unequivocally demonstrated that this combined maneuver of 90-degree flexion and maximal distention displaces the radial nerve anteriorly by an average of 11 to 14 millimeters, and the median nerve by up to 14 to 17 millimeters from the standard anterolateral and anteromedial portal sites, respectively. Failure to achieve or maintain this distention throughout the establishment of anterior portals drastically reduces this safety margin to a perilous 3 to 4 millimeters, exponentially increasing the risk of iatrogenic transection or neuropraxia.
Exhaustive Indications and Contraindications
The decision to proceed with elbow arthroscopy must be grounded in a rigorous clinical evaluation, advanced imaging, and a clear understanding of the procedure's capabilities and limitations. As surgical techniques and instrumentation have advanced, the indications have broadened significantly, transitioning from purely diagnostic explorations to highly complex reconstructive and therapeutic interventions.
Indications
The therapeutic indications for elbow arthroscopy are vast and encompass both the anterior and posterior compartments. In the setting of degenerative or post-traumatic osteoarthritis, arthroscopic osteocapsular arthroplasty—which includes extensive synovectomy, capsular release, and the resection of impinging osteophytes (particularly in the olecranon and coronoid fossae)—has demonstrated excellent long-term outcomes in restoring functional range of motion. For the overhead athlete, the arthroscopic management of valgus extension overload syndrome involves the precise excision of posteromedial olecranon osteophytes while meticulously preserving the stabilizing sublime tubercle and the ulnar collateral ligament.
Intra-articular loose bodies, whether cartilaginous or osteochondral, are perhaps the most classic and rewarding indication, as their arthroscopic removal immediately resolves mechanical catching and locking. Osteochondritis dissecans (OCD) of the capitellum, frequently seen in adolescent athletes, is optimally managed arthroscopically, allowing for staging of the lesion, microfracture of the subchondral bone, or internal fixation of unstable fragments. Additionally, inflammatory arthropathies such as rheumatoid arthritis respond exceptionally well to arthroscopic synovectomy, particularly when medical management fails. More advanced indications include the arthroscopic resection of the radial head for severe comminuted fractures or radiocapitellar arthritis, the release of the ECRB tendon for recalcitrant lateral epicondylitis, and the management of selected intra-articular fractures, such as capitellar or radial head shear fractures.
Contraindications
Despite its versatility, elbow arthroscopy carries strict contraindications that must be respected to prevent catastrophic complications. Absolute contraindications include active periarticular or intra-articular soft-tissue infections (unless the arthroscopy is specifically performed for irrigation and debridement of a septic joint). Severe architectural distortion of the bony anatomy, secondary to massive trauma, advanced congenital deformities, or severe heterotopic ossification, represents an absolute contraindication, as the standard anatomical landmarks required for safe portal placement are obliterated, rendering the neurovascular structures unpredictably displaced.
Relative contraindications require careful preoperative deliberation. A history of prior ulnar nerve transposition is a critical relative contraindication; the surgeon must assume the ulnar nerve is in an atypical, unprotected location, precluding the safe use of standard medial or posteromedial portals without formal open exploration and neurolysis. Similarly, prior extensive open elbow surgery or severe arthrofibrosis drastically reduces capsular compliance. In these cases, the joint cannot be adequately distended, negating the protective biomechanical displacement of the anterior neurovascular bundle. The surgeon must proceed with extreme caution, often utilizing alternative portal trajectories or converting to an open arthrotomy if safe access cannot be verified.
| Category | Specific Condition | Rationale / Surgical Consideration |
|---|---|---|
| Absolute Indications | Symptomatic Loose Bodies | Immediate mechanical relief; prevents further chondral damage. |
| Absolute Indications | Capitellar OCD (Unstable/Detached) | Allows for debridement, microfracture, or fragment fixation. |
| Absolute Indications | Valgus Extension Overload | Precise resection of posteromedial osteophytes without destabilizing the UCL. |
| Relative Indications | Recalcitrant Lateral Epicondylitis | Arthroscopic ECRB release provides excellent visualization of the undersurface. |
| Absolute Contraindications | Active Cellulitis / Overlying Infection | High risk of seeding the sterile intra-articular space. |
| Absolute Contraindications | Severe Bony Distortion / Heterotopic Ossification | Obliteration of palpable landmarks; unpredictable neurovascular anatomy. |
| Relative Contraindications | Prior Ulnar Nerve Transposition | Ulnar nerve is no longer protected in the cubital tunnel; high risk of iatrogenic injury. |
| Relative Contraindications | Severe Arthrofibrosis / Stiff Elbow | Diminished capsular compliance prevents safe fluid distention and nerve displacement. |
Pre-Operative Planning, Templating, and Patient Positioning
The foundation of a successful elbow arthroscopy is laid long before the patient enters the operating theater. Meticulous preoperative planning is mandatory. A comprehensive clinical examination must document the preoperative range of motion, areas of point tenderness, and a highly detailed neurovascular baseline. Any preexisting paresthesias or motor deficits in the radial, median, ulnar, or anterior interosseous nerve distributions must be explicitly documented to differentiate them from potential postoperative iatrogenic complications. High-quality orthogonal radiographs are standard, but advanced imaging, specifically computed tomography (CT) without contrast, is invaluable for three-dimensional spatial templating of osteophytes, loose bodies, and heterotopic bone. Magnetic resonance imaging (MRI) is preferred for evaluating chondral defects, OCD lesions, and ligamentous integrity.
Anesthetic considerations play a crucial role in patient safety and postoperative assessment. While regional anesthesia (such as a supraclavicular or interscalene block) provides excellent intraoperative muscle relaxation and postoperative analgesia, dense, long-lasting blocks are highly controversial in elbow arthroscopy. A prolonged motor and sensory block masks the immediate postoperative neurological examination, delaying the diagnosis of a devastating iatrogenic nerve injury or an impending compartment syndrome secondary to fluid extravasation. Consequently, many high-volume arthroscopists prefer general anesthesia supplemented with a short-acting regional block or local intra-articular infiltration, ensuring the patient can participate in a reliable neurological exam in the recovery room.
Patient positioning is the most critical logistical decision, dictating the surgeon's ergonomic access, fluid management dynamics, and the gravitational behavior of the neurovascular structures. The two predominant orientations are the supine suspended position and the prone position, each with distinct biomechanical advantages.
The Supine Suspended Position
In the supine position, the patient is placed with the operative arm suspended vertically using a specialized overhead traction device. The shoulder is abducted to 90 degrees, and the elbow is flexed to 90 degrees. A non-sterile tourniquet is applied high on the brachium.

This setup provides excellent, unobstructed access to the anterior compartment and the medial and lateral gutters. The overhead traction system dynamically maintains the critical 90-degree flexion angle, which is biomechanically essential for anterior neurovascular displacement. Furthermore, it allows for seamless dynamic examination of the joint through its full range of motion under anesthesia. The primary disadvantage of the supine position is the relative difficulty in accessing the posterior compartment, as the surgeon must work against gravity, and the triceps muscle remains under tension, restricting posterior capsular volume.
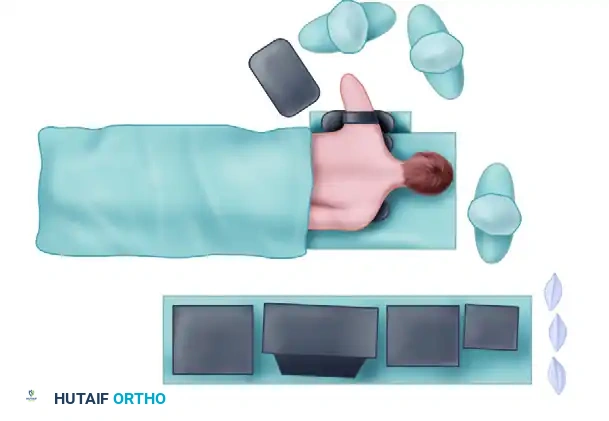
The Prone Position
Advocated by many master arthroscopists, particularly when extensive posterior compartment pathology (e.g., severe valgus extension overload or posterior arthrofibrosis) is anticipated, the prone position offers unparalleled stability and posterior access. The patient is carefully rolled onto chest rolls, ensuring all pressure points are padded and the airway is secure. The operative arm is abducted and placed over a specialized arm holder or a padded sandbag, allowing the elbow to flex freely to 90 degrees.

The biomechanical advantage of the prone position cannot be overstated: gravity assists in pulling the anterior neurovascular structures (the median nerve and brachial artery) away from the anterior capsule, providing an added, passive margin of safety when establishing the anterior portals. Furthermore, the posterior compartment is easily accessible, and the surgeon can operate in a highly ergonomic, seated position. The disadvantages include the logistical complexities of prone positioning, the potential for airway compromise, and slightly more challenging access to the anterior joint compared to the supine setup.
Step-by-Step Surgical Approach and Portal Placement Technique
The safe establishment of arthroscopic portals is the most critical, high-stakes phase of the entire operation. The surgeon must adhere to a strict, sequential protocol, beginning with maximal joint distention and followed by meticulous superficial dissection.
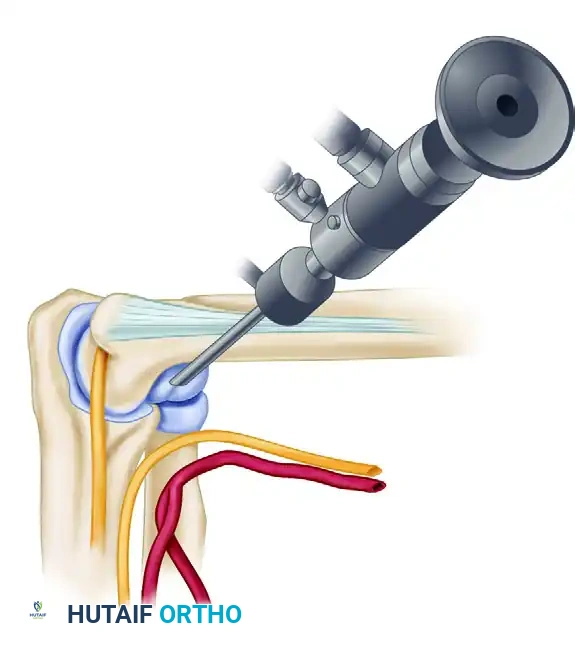
Initial Joint Distention Technique
Before any scalpel touches the skin, the joint must be maximally distended to displace the neurovascular structures. This is universally performed through the direct lateral "soft spot." The surgeon palpates the center of the anconeus triangle, bounded by the lateral epicondyle, the radial head, and the tip of the olecranon. An 18-gauge spinal needle is introduced into this soft spot, directed precisely toward the center of the radiocapitellar articulation. Aspiration is performed; the free backflow of synovial fluid confirms accurate intra-articular placement.
Subsequently, 20 to 30 milliliters of sterile normal saline is forcefully injected using a large syringe. The joint should become palpably tense, and the elbow will naturally assume a resting posture of approximately 70 to 80 degrees of flexion due to maximal capsular volume. It is imperative to avoid pushing the needle too far anteriorly into the antecubital fossa; extra-articular fluid extravasation will collapse the anterior joint space, completely negating the protective neurovascular displacement and drastically increasing the risk of nerve injury during subsequent portal placement.
Lateral Portal Establishment
The lateral portals are typically the first operative portals established, providing excellent visualization of the anterior compartment.
The Proximal Anterolateral Portal is widely considered the safest initial viewing portal. Located 2 centimeters proximal and 1 centimeter anterior to the lateral epicondyle, it is established using the "nick and spread" technique. A No. 11 blade is used to incise only the superficial epidermis. Deep penetration with a scalpel is strictly forbidden, as it risks severing the posterior antebrachial cutaneous nerve. A small mosquito hemostat is then used to bluntly dissect through the subcutaneous fat, spreading the fibers of the brachioradialis and the extensor carpi radialis longus down to the tense anterior capsule. A blunt trocar and cannula are then introduced, directed toward the center of the joint. By staying proximal to the joint line, this portal maximizes the distance from the radial nerve (averaging 13.7 mm of clearance).
The Mid-Anterolateral Portal is located just proximal and 1 centimeter anterior to the palpable radiocapitellar joint. It provides a superior trajectory for instrumenting the deep medial compartment and the coronoid process. However, it places the radial nerve at slightly higher risk (10.9 mm clearance) compared to the proximal portal. The historical distal anterolateral portal has been universally abandoned by modern surgeons due to its unacceptably close proximity to the radial nerve (often less than 7 mm).
Medial Portal Establishment
Medial portals are essential for viewing the lateral gutter, the radiocapitellar joint, and addressing anterior capsular pathology. Strict adherence to anatomical landmarks is required to protect the median nerve, brachial artery, and ulnar nerve.

The Proximal Medial (Supracondylar) Portal, pioneered by Poehling, is the preferred medial portal, particularly in the prone position. It is located 2 centimeters proximal and slightly anterior to the medial epicondyle.
Before incision, the ulnar nerve must be physically palpated and mapped. After a superficial skin incision, a blunt trocar is introduced. The critical technical nuance of this portal is that the trocar must be inserted anterior to the medial intermuscular septum. The surgeon must feel the trocar maintain direct, hard contact with the anterior bony cortex of the distal humerus as it is directed distally and laterally toward the radial head.
By utilizing the anterior humerus as a physical, bony shield, the surgeon ensures the instrument stays safely posterior to the median nerve and brachial artery. This portal provides an unparalleled, panoramic view of the entire anterior compartment.

The Anteromedial Portal is located 2 centimeters distal and 2 centimeters anterior to the medial epicondyle. While useful, it places the medial antebrachial cutaneous nerve and the basilic vein at high risk. A critical clinical pearl is to place the arthroscope in the anterolateral portal, direct the light medially against the capsule, and dim the room lights. The superficial basilic vein and crossing cutaneous nerves can often be transilluminated and marked on the skin with a sterile pen, allowing the surgeon to adjust the incision site to avoid iatrogenic injury.
Posterior Portal Establishment
Posterior portals are utilized for addressing pathology in the olecranon fossa, resecting posteromedial osteophytes, and removing loose bodies in the posterior compartment.
For posterior access, the elbow is typically extended to 45 to 60 degrees in the supine position to relax the triceps, or allowed to rest at 90 degrees in the prone position.
The Posterolateral Portal is located 2 to 3 centimeters proximal to the tip of the olecranon, just lateral to the border of the triceps tendon. It is the primary viewing portal for the posterior joint. The Straight Posterior (Posterocentral) Portal is located in the midline, centered within the triceps tendon, approximately 2 centimeters medial to the posterolateral portal. It is established under direct intra-articular visualization. The surgeon must be acutely aware that the ulnar nerve lies approximately 2.5 centimeters medial to the center of the joint; medial deviation of the trocar during the establishment of the straight posterior portal places the ulnar nerve at catastrophic risk.
Complications, Incidence Rates, and Salvage Management
While elbow arthroscopy is generally safe when performed by experienced surgeons, the complication profile is significantly higher than that of knee or shoulder arthroscopy. The overall complication rate reported in the literature ranges from 5% to 11%, with transient neurological injuries being the most frequent adverse events. The unforgiving anatomy means that minor technical deviations can result in profound morbidity.
Neurological complications are the most feared. The ulnar nerve is the most commonly injured structure, typically resulting from errant posteromedial portal placement, over-aggressive resection of posteromedial osteophytes, or thermal necrosis from radiofrequency wands used near the cubital tunnel. The superficial sensory branch of the radial nerve and the posterior interosseous nerve (PIN) are at risk during anterolateral portal establishment, especially if the joint is inadequately distended. The medial antebrachial cutaneous nerve is frequently injured during anteromedial portal placement if the "nick and spread" technique is not strictly adhered to. Most neurological injuries are transient neuropraxias secondary to traction, fluid compression, or local anesthetic extravasation, and typically resolve within 3 to 6 months. However, complete neurotmesis (transection) requires immediate microsurgical exploration and repair, often with guarded prognoses.
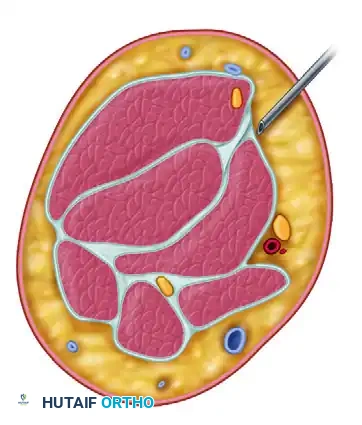
Fluid extravasation is a ubiquitous challenge. The elbow capsule is relatively thin, and the high-pressure fluid pumps necessary for visualization can rapidly force fluid into the surrounding fascial compartments of the forearm and brachium. Prolonged surgical times, elevated pump pressures, and multiple capsular punctures exacerbate this risk. In severe cases, massive fluid extravasation can precipitate an acute compartment syndrome, necessitating emergent multi-compartment fasciotomies. Surgeons must vigilantly monitor the tension of the forearm throughout the procedure and utilize gravity-fed fluid systems or low-pressure pump settings (typically 30-40 mmHg) whenever possible.
Infection, while rare (incidence <1%), can be devastating, leading to rapid chondrolysis and severe arthrofibrosis. Portal site leakage and superficial wound dehiscence are more common, particularly at the posterior portals where the subcutaneous tissue is thin. These are generally managed conservatively with brief immobilization and oral antibiotics.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Ulnar Nerve Neuropraxia | 2% - 5% | Errant posteromedial portals; thermal injury; prior transposition. | Strict adherence to midline for posterior portals; avoid RF wands medially; observe for 3-6 months. |
| Radial Nerve Injury (PIN) | 1% - 3% | Distal anterolateral portal use; inadequate joint distention. | Utilize proximal anterolateral portal; ensure >20mL fluid distention; emergent exploration if transection suspected. |
| Superficial Cutaneous Nerve Injury | 2% - 4% | Deep scalpel incisions; failure to use "nick and spread" technique. | Incise skin only; blunt dissection to capsule; transilluminate veins/nerves prior to medial incisions. |
| Compartment Syndrome | < 1% | Prolonged surgical time (>2 hours); high pump pressures; capsular rents. | Monitor forearm tension closely; use low pump pressures; emergent fasciotomy if clinically diagnosed post-op. |
| Deep Joint Infection | < 1% | Prolonged surgery; inadequate sterilization; prior local injections. | Emergent arthroscopic or open irrigation and debridement; targeted IV antibiotic therapy. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following elbow arthroscopy is highly contingent upon the specific pathology addressed and the extent of the surgical intervention. However, unlike traditional open arthrotomies, the minimally invasive nature of arthroscopy generally permits highly accelerated rehabilitation protocols, which are essential for preventing the rapid onset of capsular adhesions and debilitating arthrofibrosis.
Phase 1: Immediate Postoperative Phase (Days 0 to 7)
The primary objectives in the immediate postoperative period are the mitigation of edema, pain control, and the preservation of existing range of motion. Immediately following wound closure, a bulky, compressive soft dressing is applied to minimize postoperative hemarthrosis and extra-articular fluid accumulation. Strict elevation of the extremity above the level of the heart and aggressive cryotherapy are paramount in the first 72 hours. Unless a specific structural repair was performed (such as an osteochondral fragment fixation or a ligamentous plication), patients are encouraged to initiate active and active-assisted range of motion (ROM) exercises for the elbow, wrist, and hand within 24 to 48 hours. Prolonged immobilization is strictly contraindicated in routine diagnostic or debridement procedures, as the elbow joint is notoriously prone to rapid stiffening.
Phase 2: Intermediate Rehabilitation Phase (Weeks 1 to 4)
Upon removal of the compressive dressings and confirmation of portal site healing, the focus shifts to achieving full, symmetric range of motion and initiating early strengthening. Gentle, sustained terminal stretching is incorporated to address any residual flexion or extension deficits. Dynamic splinting (e.g., turnbuckle orthoses) may be prescribed for patients exhibiting recalcitrant stiffness, particularly following extensive capsular releases for severe arthrofibrosis. Isotonic strengthening of the biceps, triceps, and forearm musculature is gradually introduced, utilizing light resistance bands and progressive weight-bearing exercises.
Phase 3: Advanced Strengthening and Return to Play (Weeks 4 and Beyond)
The final phase of rehabilitation is tailored to the patient's specific functional demands. For the overhead throwing athlete, this phase involves advanced plyometric training, eccentric strengthening of the decelerator musculature, and a highly structured, progressive interval throwing program. Return to competitive play or heavy manual labor is typically authorized once the patient demonstrates full, painless range of motion, normal neurovascular function, and isokinetic strength equal to at least 90% of the contralateral, uninjured extremity. Routine clinical
