Arthroscopic Management of Elbow Valgus Extension Overload: A Masterclass

Key Takeaway
This masterclass guides fellows through arthroscopic treatment of valgus extension overload. We cover detailed anatomy, prone positioning, and meticulous intraoperative steps for posteromedial olecranon spur excision. Emphasizing ulnar nerve protection and UCL assessment, we discuss portal placement, instrument use, and postoperative care, preparing you for complex elbow cases and managing potential complications.
Comprehensive Introduction and Patho-Epidemiology
Valgus extension overload (VEO) of the elbow represents a complex, debilitating clinical entity predominantly observed in overhead throwing athletes, most notably baseball pitchers, javelin throwers, and elite tennis players. This condition is far more nuanced than the mere presence of a symptomatic bone spur; it is the culmination of a cascade of intricate biomechanical failures, requiring the orthopedic surgeon to possess a profound understanding of elbow kinematics, soft tissue restraints, and the protection of critical neurovascular structures. The goal of intervention is not simply excision, but the meticulous restoration of an athlete's career through joint preservation and biomechanical optimization.
The pathogenesis of VEO is characterized by a classic triad of distinct yet interrelated pathologies: medial compartment distraction, lateral compartment compression, and posterior compartment impingement. During the late cocking and early acceleration phases of the overhead throwing motion, the elbow is subjected to tremendous valgus torque, frequently exceeding the innate tensile strength of the ulnar collateral ligament (UCL). This repetitive valgus stress repeatedly distracts the medial side of the elbow, forcefully compresses the radiocapitellar joint on the lateral side, and violently drives the posteromedial tip of the olecranon into the olecranon fossa.
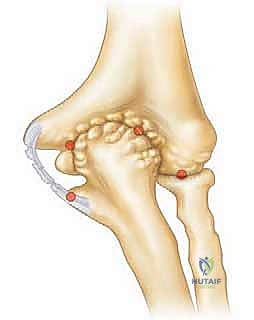
The ultimate consequence of this repetitive microtrauma, especially in the setting of inadequate rest and recovery, is the progressive attenuation or outright catastrophic failure of the UCL. As the primary restraint to valgus stress becomes insufficient, abnormal valgus rotation of the elbow ensues. This pathologic laxity significantly alters the kinematics of the highly constrained posterior elbow articulation. Specifically, it results in direct, eccentric bony impingement between the posteromedial aspect of the olecranon and the medial wall of the olecranon fossa. This repeated, forceful contact generates reactive osteophyte formation, chondral fissuring, and the genesis of the VEO syndrome.
As the condition progresses, the repetitive abutment leads to the formation of osteochondral loose bodies and significant chondromalacia within the posterior compartment. The presence of these osteophytes physically blocks terminal extension, creating a mechanical flexion contracture. Furthermore, the inflammatory milieu generated by this chronic impingement can lead to secondary capsular contracture and adjacent ulnar neuritis. Recognizing this continuum of pathology is paramount; treating the posterior impingement without addressing underlying medial instability is a frequent cause of surgical failure in the throwing athlete.
Detailed Surgical Anatomy and Biomechanics
Before contemplating arthroscopic intervention, the surgeon must possess a crystal-clear, three-dimensional understanding of the elbow's osseous and ligamentous anatomy. Chronic bony impingement, as seen in valgus extension overload, distorts native landmarks through significant chondral lesions and reactive osteophyte formation within the posterior compartment. The bony articulation of the ulnohumeral joint provides primary stability to varus and valgus forces primarily at the extremes of motion: specifically, at angles of less than 20 degrees of flexion and greater than 120 degrees of flexion.
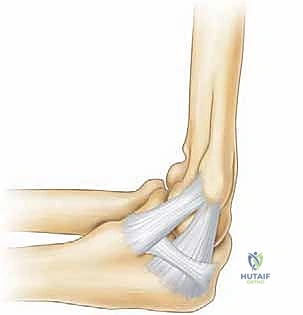
However, the crucial functional arc for overhead athletic activity lies between 20 and 120 degrees of flexion. Within this range, the osseous architecture offers minimal constraint, rendering the soft tissues as the chief stabilizers. The ulnar collateral ligament (UCL) complex is the primary static restraint to valgus stress. It is a highly specialized structure composed of three distinct bands: the anterior band, the posterior band, and the transverse ligament (Cooper's ligament). The anterior band, originating from the anteroinferior surface of the medial epicondyle and inserting onto the sublime tubercle of the ulna, is the most critical structure for valgus stability.
The anterior band is further subdivided into anterior and posterior bundles, which perform reciprocal functions to maintain stability throughout the functional arc. The anterior bundle is taut in extension, while the posterior bundle becomes taut in flexion. This intricate arrangement ensures continuous medial stability. UCL insufficiency can be biomechanically subtle yet clinically devastating; cadaveric ligament-sectioning studies have demonstrated that complete transection of the anterior band may lead to as little as a 3-degree increase in valgus laxity. While seemingly negligible, this microinstability is sufficient to alter the contact mechanics of the posteromedial olecranon, precipitating VEO.
It is postulated that the chronic impingement resulting from this microinstability leads to the characteristic posteromedial olecranon osteophyte formation. These osteophytes are not benign; their proximity to the cubital tunnel can directly cause mechanical irritation of the ulnar nerve, leading to progressive ulnar neuropathy. Additionally, they serve as a physical block to full elbow extension. The surgeon must recognize that the olecranon tip normally resides deep within the olecranon fossa during terminal extension; any osteophytic encroachment alters this highly congruous articulation, contributing to the early onset of posterior compartment osteoarthritis if left unaddressed.
Exhaustive Indications and Contraindications
The clinical evaluation of a patient with suspected VEO requires a meticulous history and a highly specific physical examination. The typical patient presents with a history of high-level, repetitive overhead activity, frequently a baseball pitcher. The primary subjective complaints include a progressive loss of terminal elbow extension accompanied by sharp, localized posterior or posteromedial elbow pain. Pitchers will characteristically localize their pain to the late acceleration and early follow-through phases of the throwing motion, corresponding precisely to the moments of peak valgus stress and maximal posterior impingement forces.

When examining the elbow, the differential diagnosis must be broad and systematically evaluated. The clinician must differentiate VEO from isolated UCL insufficiency, ulnar neuritis, medial epicondylitis, and flexor-pronator mass pathology. The Valgus Extension Overload Test is pathognomonic; the examiner applies a valgus stress to the elbow while forcefully moving it into terminal extension, simulating the throwing motion. A positive test yields a reproduction of the athlete's posterior elbow pain and a mechanical block.

Concurrently, the integrity of the UCL must be rigorously assessed. The Valgus Stress Test, performed at 20-30 degrees of flexion to unlock the olecranon from its fossa, and the Moving Valgus Stress Test (O'Driscoll) are critical. The Milking Maneuver further isolates the anterior band of the UCL. Pain, apprehension, or a subjective sense of "opening up" on the medial side indicates underlying UCL insufficiency. Direct palpation over the posteromedial olecranon will typically elicit exquisite point tenderness. Range of motion assessment often reveals a flexion contracture, signifying either mechanical osteophyte impingement or anterior capsular contracture.
Indications and Contraindications Summary
| Category | Specific Criteria | Clinical Rationale |
|---|---|---|
| Primary Indications | Symptomatic posteromedial impingement failing 3-6 months of conservative care. | Mechanical block and pain cannot be resolved without osseous resection. |
| Primary Indications | Presence of symptomatic posterior compartment loose bodies. | Loose bodies cause mechanical locking, catching, and accelerated chondral wear. |
| Relative Indications | Concomitant UCL insufficiency requiring reconstruction. | VEO debridement is often performed concurrently with UCL reconstruction to restore kinematics. |
| Absolute Contraindications | Severe bony or fibrous ankylosis. | Prevents safe arthroscopic access, instrument triangulation, and adequate visualization. |
| Absolute Contraindications | Active localized or systemic infection. | Risk of seeding the joint and causing catastrophic septic arthritis. |
| Relative Contraindications | Prior anterior transposition of the ulnar nerve. | Distorted anatomy severely increases the risk of iatrogenic ulnar nerve transection during portal placement. |
| Relative Contraindications | Advanced, end-stage osteoarthritis in a non-throwing patient. | Arthroscopic debridement offers diminishing returns in global joint degeneration. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful arthroscopic management of VEO. Radiographs are the mandatory initial step, requiring standard anteroposterior (AP) and lateral views. However, the standard views frequently obscure the posteromedial anatomy. Therefore, an axial view of the olecranon or an AP view taken in 110 degrees of flexion is highly advocated to accurately profile the posteromedial spur formation. These specialized views allow the surgeon to template the exact amount of osseous resection required.

Because radiographs alone routinely underestimate the true burden of intra-articular pathology, advanced cross-sectional imaging is essential. Magnetic Resonance Imaging (MRI), often enhanced with intra-articular gadolinium (MR arthrography), is the gold standard for evaluating the integrity of the UCL, assessing the extent of chondral lesions, and identifying radiolucent loose bodies. A coronal T1 fat-suppressed sequence is critical for identifying partial-thickness, undersurface tears of the anterior bundle of the UCL. Computed Tomography (CT), particularly with 3D reconstructions, is invaluable for precise spatial mapping of the osteophytes and preoperative surgical templating.
During the preoperative clinical assessment, the surgeon must definitively document the status and stability of the ulnar nerve. If the nerve is hypermobile, subluxating over the medial epicondyle during flexion, a concomitant ulnar nerve transposition may be indicated. This drastically alters portal placement, as medial portals become hazardous. Furthermore, the surgeon must synthesize the imaging and clinical exam to determine if UCL reconstruction is required. Failure to adequately address underlying valgus instability in the setting of VEO will inevitably lead to recurrent osteophyte formation and treatment failure.

For arthroscopic intervention targeting posterior compartment pathology, the prone position is overwhelmingly preferred. The patient is placed prone with the operative arm draped over a well-padded arm board or specialized elbow positioner, allowing the elbow to hang freely at 90 degrees of flexion. This position offers unparalleled advantages: it provides exceptional, unobstructed access to the posterior and posterolateral compartments, stabilizes the humerus effectively, and utilizes gravity to assist in joint distraction and fluid extravasation management away from the airway. Meticulous padding of all bony prominences, particularly the contralateral ulnar nerve and bilateral peroneal nerves, is mandatory to prevent positioning neuropathies.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with meticulous surface anatomy palpation and marking of the medial epicondyle, lateral epicondyle, olecranon tip, radial head, and the course of the ulnar nerve. Joint distension is achieved by injecting 15-20 mL of normal saline through the soft spot (center of the triangle formed by the lateral epicondyle, radial head, and olecranon). Standard diagnostic arthroscopy typically begins in the anterior compartment using a proximal anteromedial portal, established 2 cm proximal and 1 cm anterior to the medial epicondyle, carefully protecting the medial antebrachial cutaneous nerve.

Once the anterior compartment is evaluated and any loose bodies or anterior capsular contractures are addressed, attention is turned to the posterior compartment, which is the epicenter of VEO pathology. A direct posterior portal or a posterolateral portal is established. The posterolateral portal is placed 3 cm proximal to the olecranon tip, just lateral to the triceps tendon. This provides an excellent panoramic view of the olecranon fossa and the posteromedial olecranon articulation. A thorough diagnostic sweep is performed to identify the "kissing lesion"—the corresponding chondral damage on the medial wall of the olecranon fossa caused by the abutting osteophyte.

Osteophyte excision is the critical step of the procedure. Using an accessory posterocentral or direct posterior portal for instrumentation, a motorized shaver and a guarded arthroscopic burr are introduced. The surgeon must meticulously resect the posteromedial osteophyte, restoring the normal contour of the olecranon. It is imperative to maintain the burr blade facing laterally or anteriorly, away from the medial gutter, to strictly avoid iatrogenic injury to the ulnar nerve, which lies perilously close, separated only by the thin medial capsule.
A critical biomechanical principle must be adhered to during resection: the surgeon must not resect more than 3 millimeters of the native olecranon tip. Over-resection of the olecranon removes a critical osseous restraint to valgus stress. Biomechanical studies have unequivocally demonstrated that excising more than 3 to 4 mm of the olecranon exponentially increases the strain on the anterior band of the UCL, potentially converting a stable, symptomatic elbow into a grossly unstable one, thereby necessitating an otherwise avoidable UCL reconstruction.

Following adequate resection, the elbow is taken through a dynamic range of motion under direct arthroscopic visualization to confirm the complete elimination of impingement in terminal extension and valgus stress. The olecranon should seat smoothly within the fossa without abutment. Any remaining loose bodies within the posterior or posteromedial gutters are meticulously extracted. The joint is thoroughly lavaged, portals are closed with non-absorbable sutures, and a sterile compressive dressing is applied to minimize postoperative hemarthrosis and swelling.
Complications, Incidence Rates, and Salvage Management
While arthroscopic management of VEO is highly successful in properly selected patients, the highly constrained nature of the elbow joint and the proximity of major neurovascular structures render it an unforgiving anatomical region. Complications, though relatively infrequent in experienced hands, can be catastrophic to an athlete's career. The surgeon must maintain a high index of suspicion for potential pitfalls and possess the technical acumen to execute salvage procedures when necessary.
The most devastating complication is iatrogenic neurological injury, most commonly involving the ulnar nerve. The ulnar nerve is particularly vulnerable during the establishment of medial portals and during the aggressive debridement of the posteromedial gutter. Superficial nerves, such as the medial and lateral antebrachial cutaneous nerves, are also at risk during portal placement. Meticulous adherence to anatomical landmarks, the "nick and spread" technique for portal entry, and the use of guarded instruments are non-negotiable safety standards.
Another profound complication is iatrogenic valgus instability resulting from over-resection of the olecranon. As previously detailed, the olecranon provides crucial secondary valgus constraint. If the surgeon aggressively resects the native olecranon in an attempt to guarantee extension, the primary valgus restraint (UCL) is subjected to catastrophic stress loads. If this occurs, the patient will experience profound medial elbow pain and inability to throw, necessitating a salvage UCL reconstruction (Tommy John surgery) and a prolonged, year-long rehabilitation process.
Complications and Management Strategies
| Complication | Estimated Incidence | Etiology / Mechanism | Salvage / Management Strategy |
|---|---|---|---|
| Ulnar Nerve Injury | 1% - 3% | Direct trauma from burr/shaver in posteromedial gutter; thermal injury; fluid extravasation compression. | Immediate intraoperative exploration if recognized. Post-op: EMG/NCS at 6 weeks. May require neurolysis or transposition. |
| Iatrogenic Instability | 2% - 5% | Resection of >3mm of native olecranon tip; failure to recognize pre-existing UCL tear. | Staged or concurrent UCL reconstruction using palmaris longus or gracilis autograft. |
| Superficial Nerve Neuroma | 2% - 4% | Laceration of Medial or Lateral Antebrachial Cutaneous nerves during portal placement. | Conservative management with gabapentin/desensitization. Surgical excision and burying of stump for refractory cases. |
| Post-Operative Stiffness | 5% - 10% | Inadequate post-op pain control leading to guarding; aggressive heterotopic ossification; capsular scarring. | Aggressive physical therapy, dynamic splinting. Refractory cases may require arthroscopic capsular release at 6 months. |
| Recurrent Impingement | 5% - 8% | Inadequate initial resection; continued pitching with subtle, unaddressed UCL microinstability. | Revision arthroscopy for further debridement; mandatory reassessment of UCL integrity. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation program following arthroscopic debridement for VEO is as critical as the surgical execution itself. The protocol must be meticulously phased, balancing the need for early tissue mobilization to prevent stiffness with the imperative to protect the healing intra-articular environment. For the overhead throwing athlete, rehabilitation is not complete until kinetic chain mechanics are fully restored and a structured interval throwing program is successfully executed.
Phase I: Immediate Post-Operative Phase (Weeks 0-2)
The primary goals during this initial phase are the protection of the surgical site, mitigation of inflammation and hemarthrosis, and the early restoration of range of motion. The patient is typically placed in a soft compressive dressing and a sling for comfort, which is discontinued within the first 3 to 5 days. Cryotherapy is utilized aggressively. Gentle, active-assisted range of motion (AAROM) exercises for elbow flexion, extension, pronation, and supination are initiated immediately. Isometrics for the wrist and shoulder are encouraged. The goal by the end of week two is to achieve full, symmetric range of motion, particularly focusing on regaining the terminal extension that was mechanically blocked preoperatively.
Phase II: Intermediate Phase (Weeks 2-6)
Once full, painless range of motion is achieved, the focus shifts to muscular endurance and isotonic strengthening. Scapular stabilization exercises and rotator cuff strengthening are paramount, as proximal kinetic chain deficits significantly increase distal stress at the elbow. Isotonic exercises for the biceps, triceps, wrist flexors, and extensors are progressively loaded. Proprioceptive neuromuscular facilitation (PNF) patterns are integrated. The surgeon must monitor for any return of posterior impingement pain or medial-sided symptoms during this loading phase, which may indicate underlying, unaddressed instability.
Phase III: Advanced Strengthening Phase (Weeks 6-12)
This phase bridges the gap between basic strength and athletic performance. Plyometric exercises are introduced to train the stretch-shortening cycle of the upper extremity musculature. Two-hand plyometric chest passes and overhead throws progress to single-arm exercises. Core and lower extremity strengthening are heavily emphasized; the throwing motion generates power from the ground up, and any weakness in the legs or core forces the shoulder and elbow to overcompensate, leading to recurrent pathology.
Phase IV: Return to Sport and Interval Throwing (Weeks 12+)
The final phase involves a highly structured, progressive Interval Throwing Program (ITP). The athlete must have full, painless ROM, normal strength testing, and a stable clinical exam before initiating the ITP. The program begins with short-distance, flat-ground throwing (e.g., 45 feet) and gradually progresses in distance and intensity over several weeks. Pitchers eventually transition to throwing off the mound, initially focusing on fastballs before reintroducing breaking pitches, which place higher torque on the elbow. Return to competitive play is authorized only when the athlete can complete the entire ITP without symptoms and demonstrates flawless throwing mechanics.
Summary of Landmark Literature and Clinical Guidelines
The evolution of our understanding and surgical management of Valgus Extension Overload is deeply rooted in landmark orthopedic literature. A thorough grasp of these foundational studies is essential for any surgeon managing the overhead throwing athlete. The biomechanical basis of VEO was elegantly elucidated by Fleisig and Andrews, who quantified the extraordinary kinematics and kinetics of the baseball pitch, demonstrating that valgus torque during late cocking frequently approaches the ultimate failure load of the native UCL.
The clinical presentation and initial arthroscopic management strategies were pioneered by Andrews and Timmerman in the mid-1990s. Their seminal work highlighted the "kissing lesion" phenomenon and established the parameters for safe arthroscopic resection. They emphasized that while osteophyte excision provides excellent short-term relief, long-term outcomes are heavily dependent on the integrity of the medial soft-tissue restraints.
Furthermore, the critical danger of over-resection was biomechanically proven by Kamineni and O'Driscoll. Their cadaveric studies demonstrated that the olecranon tip is a vital secondary stabilizer to valgus stress. They established the clinical guideline that resection must be strictly limited to the abnormal osteophyte, typically preserving the native olecranon architecture to prevent catastrophic load shifting to the UCL.
Recent literature has focused heavily on the concurrent management of VEO and UCL insufficiency. Studies by Cain and Dugas have shown that in throwing athletes with symptomatic VEO and concomitant UCL tears, isolated arthroscopic debridement yields unacceptably high failure rates and early return of symptoms. In these scenarios, simultaneous arthroscopic VEO debridement followed by open UCL reconstruction has become the gold standard, demonstrating superior rates of return to previous levels of athletic competition. This underscores the masterclass principle: successful management of the throwing elbow requires treating the joint as an integrated biomechanical envelope, rather than isolating individual pathologies.
