Advanced Arthroscopic Management of the Elbow: Synovial Plica, Radial Head Resection, and Arthrofibrosis

Key Takeaway
Arthroscopic management of the elbow requires a profound understanding of complex regional anatomy and joint biomechanics. This comprehensive guide details the surgical techniques for resecting pathological synovial plicae, performing arthroscopic radial head excision, and releasing severe post-traumatic arthrofibrosis. Emphasizing portal safety, dynamic intraoperative assessment, and evidence-based postoperative rehabilitation, these advanced procedures restore radiocapitellar kinematics and salvage functional range of motion in the compromised elbow joint.
Comprehensive Introduction and Patho-Epidemiology
The evolution of elbow arthroscopy represents one of the most profound paradigm shifts in the management of complex intra-articular upper extremity pathology. Historically, conditions such as symptomatic synovial plicae, malunited radial head fractures, and severe post-traumatic arthrofibrosis necessitated extensive, morbid open arthrotomies. These traditional open approaches, while allowing direct macroscopic visualization, carried significant intrinsic risks, including profound iatrogenic stiffness, devastating neurovascular injury, extensive soft-tissue stripping, and highly prolonged, painful rehabilitation trajectories. Today, advanced arthroscopic techniques offer a minimally invasive, highly effective, and biomechanically respectful alternative. However, the elbow remains an exceptionally unforgiving joint. The extreme proximity of major neurovascular structures—namely the radial, median, and ulnar nerves—demands meticulous portal placement, a profound, almost instinctual understanding of three-dimensional capsuloligamentous anatomy, and uncompromising adherence to evidence-based surgical principles.
The patho-epidemiology of these three distinct yet frequently overlapping clinical entities—synovial plica syndrome, radial head pathology, and arthrofibrosis—reveals the complex interplay between acute trauma, repetitive microtrauma, and the unique biological responsiveness of the elbow capsule. The synovial plica of the elbow is a normal embryological remnant of the mesenchymal septa that divide the developing joint. Most commonly located in the posterolateral radiocapitellar joint, it is present in up to 86% to 100% of cadaveric specimens. While typically a thin, asymptomatic synovial fold that glides effortlessly during flexion, extension, pronation, and supination, repetitive microtrauma can induce a localized, aggressive synovitis. This is particularly prevalent in throwing athletes, racquet sports players, and manual laborers subjected to repetitive valgus extension overload or rotational stress. Over time, this chronic inflammatory cascade leads to fibrotic hypertrophy, transforming a benign remnant into a mechanical block that alters the delicate kinematics of the radiocapitellar articulation.
Conversely, radial head pathology warranting resection typically arises from the sequelae of acute trauma, specifically late-stage, malunited Mason Type III or IV radial head fractures, or from advanced, primary, or post-traumatic radiocapitellar osteoarthritis. The radial head is a critical secondary stabilizer of the elbow, and its pathological deformation can lead to debilitating mechanical blocks, severe localized pain, and accelerated degenerative changes in the capitellum. The epidemiology of radial head fractures indicates they account for approximately 33% of all adult elbow fractures, and a significant subset of these will eventually require delayed excision due to painful malunion or hardware failure following open reduction and internal fixation (ORIF).
Arthrofibrosis of the elbow is a notoriously debilitating complication following fractures, dislocations, or severe inflammatory events (such as septic arthritis or severe rheumatoid flares). The elbow capsule is uniquely and aggressively prone to fibroblastic proliferation and contracture. The pathophysiology is driven by post-traumatic bleeding and a hyperactive cytokine cascade—heavily mediated by Transforming Growth Factor-Beta (TGF-β) and Platelet-Derived Growth Factor (PDGF)—which leads to the rapid deposition of dense, disorganized Type I and Type III collagen within the anterior and posterior capsules. This process obliterates the normal capsular recesses, drastically reducing joint volume. Furthermore, the formation of abutting osteophytes in the coronoid and olecranon fossae frequently exacerbates the soft-tissue mechanical block to motion, creating a complex, multi-factorial stiff elbow that presents one of the most formidable challenges in orthopedic surgery.
Detailed Surgical Anatomy and Biomechanics
A masterful command of elbow anatomy is the foundational prerequisite for safe and effective advanced arthroscopy. The elbow is a highly congruent, constrained hinge joint (ginglymus) with a secondary pivot joint (trochoid) allowing for forearm rotation. The osseous anatomy comprises three distinct articulations within a single synovial cavity: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The joint capsule is relatively thin anteriorly and posteriorly but is reinforced medially and laterally by robust collateral ligament complexes. The medial ulnar collateral ligament (MUCL), specifically its anterior bundle, is the primary restraint to valgus stress. The lateral collateral ligament (LCL) complex, particularly the lateral ulnar collateral ligament (LUCL), is the primary restraint to varus and posterolateral rotatory instability (PLRI).
The biomechanics of the radial head are of paramount importance when considering resection. The radial head acts as a crucial secondary stabilizer against valgus stress and longitudinal radioulnar translation. In extension, the radial head provides approximately 30% of the valgus stability to the elbow. However, in the setting of an incompetent MUCL, the radial head becomes the primary valgus stabilizer. Therefore, arthroscopic radial head resection is strictly contraindicated if the MUCL or the interosseous membrane (IOM) is deficient, as excision in this setting will precipitate catastrophic proximal radial migration (Essex-Lopresti syndrome) or gross valgus instability. The intricate kinematics of the radiocapitellar joint also explain the mechanical impingement seen in plica syndrome. A thickened plica becomes incarcerated between the radial head and the capitellum during dynamic movement—specifically terminal extension and combined pronation-supination—producing a characteristic "catching" or "popping" sensation and leading to secondary chondromalacia.
The neurovascular anatomy dictates portal placement and defines the "danger zones" of elbow arthroscopy. The radial nerve descends anterior to the lateral epicondyle, passing between the brachialis and brachioradialis muscles. It lies perilously close (often within 3 to 7 mm) to the standard anterolateral portal. The median nerve and brachial artery course medially, passing anterior to the brachialis muscle. The median nerve is typically 4 to 14 mm from the standard anteromedial portal. The ulnar nerve courses posterior to the medial epicondyle within the cubital tunnel and is at extreme risk during posteromedial portal placement or posterior capsular releases, particularly if its anatomical course has been altered by prior trauma, subluxation, or previous transposition surgeries.
In the arthrofibrotic elbow, these anatomical relationships are drastically distorted. Gallay et al. definitively demonstrated that the volumetric capacity of a normal elbow joint is 15 to 25 mL of fluid, whereas the capacity of a severely arthrofibrotic elbow is reduced to a mere 6 mL. This drastic reduction in capsular compliance means that the neurovascular structures are not displaced away from the capsule during intra-articular fluid distension. Consequently, the safety margins between the skin portals, the capsule, and the nerves are dangerously narrowed, drastically increasing the risk of iatrogenic nerve transection or neuropraxia during initial trocar insertion and subsequent capsular release.
Exhaustive Indications and Contraindications
The decision to proceed with advanced arthroscopic intervention in the elbow requires a rigorous evaluation of the patient's pathology, functional demands, and the structural integrity of the surrounding capsuloligamentous constraints. Patient selection is paramount; inappropriate application of these techniques can result in catastrophic destabilization of the joint or irreversible neurovascular injury.
For symptomatic synovial plicae, surgical resection is indicated only after the exhaustion of a comprehensive, non-operative regimen. This includes a minimum of 3 to 6 months of relative rest, activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy focusing on periscapular and forearm stabilization, and judicious use of intra-articular corticosteroid or orthobiologic injections. The primary indication is persistent lateral-sided elbow pain exacerbated by terminal extension and supination, accompanied by a mechanical catching or snapping that limits the patient's ability to perform activities of daily living or competitive sports.
Arthroscopic radial head resection is reserved for patients with severe, isolated radiocapitellar arthritis, painful malunions of the radial head (late-stage Mason III/IV), or symptomatic non-unions that have failed conservative management. The critical prerequisite for this procedure is the absolute integrity of the MUCL and the interosseous membrane. If these primary stabilizers are compromised, the radial head cannot be safely removed without reconstructing the ligaments or replacing the radial head with a metallic prosthesis to prevent longitudinal dissociation of the forearm.
Arthroscopic management of elbow arthrofibrosis is indicated for patients with severe, recalcitrant stiffness (typically flexion contractures > 30 degrees or flexion < 110 degrees) that has plateaued after a minimum of 6 months of aggressive conservative care, including static progressive orthoses and dynamic splinting. The patient must be highly motivated and capable of adhering to a grueling postoperative continuous passive motion (CPM) and physical therapy protocol.
| Pathology | Primary Indications for Arthroscopic Management | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Synovial Plica Syndrome | Failed >3-6 months conservative therapy; mechanical catching/locking; MRI-confirmed fibrotic hypertrophy; localized radiocapitellar chondromalacia. | Active intra-articular infection; complex regional pain syndrome (CRPS) in acute flare. | Concomitant severe generalized elbow osteoarthritis; poorly controlled psychiatric barriers to rehab. |
| Radial Head Pathology | Isolated severe radiocapitellar osteoarthritis; painful late-stage malunion (Mason III/IV); mechanical block to pronation/supination. | Deficient MUCL; Deficient Interosseous Membrane (Essex-Lopresti); acute fracture amenable to ORIF. | Ulnohumeral arthritis (resection alone will not relieve pain); young, high-demand heavy laborers. |
| Elbow Arthrofibrosis | Recalcitrant stiffness failing >6 months of splinting/PT; functional arc of motion < 100 degrees; impingement from coronoid/olecranon osteophytes. | Active infection; severe architectural distortion of the ulnohumeral joint requiring total elbow arthroplasty (TEA). | Previous ulnar nerve transposition (requires open exploration first); severe heterotopic ossification bridging the joint. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful advanced elbow arthroscopy. For plica syndrome, Magnetic Resonance Imaging (MRI) is the gold standard. High-resolution, non-contrast MRI or MR arthrography will typically reveal a thickened, nodular band of tissue in the posterolateral gutter, often exceeding 3 mm in thickness, with associated focal synovitis and potential kissing lesions of chondromalacia on the radial head or capitellum. For radial head pathology and arthrofibrosis, high-quality orthogonal radiographs are mandatory. However, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is absolutely critical for mapping the precise location, volume, and morphology of impinging osteophytes within the coronoid and olecranon fossae, as well as identifying any loose bodies or heterotopic ossification (HO) that may complicate portal placement or capsular release.
Patient positioning is a matter of surgeon preference, but it significantly dictates the flow of the operation and the management of the airway. The three primary positions are lateral decubitus, prone, and supine suspended.
1. Lateral Decubitus: The patient is placed in the lateral position with the operative arm supported over a bolstered arm holder. This allows for excellent visualization of the posterior compartment and easy access to the airway by anesthesia. The arm is typically flexed to 90 degrees, allowing gravity to assist in joint distraction and naturally relaxing the anterior neurovascular structures, pulling them slightly away from the anterior capsule.
2. Prone: This position offers exceptional access to the posterior compartment and is favored by many for extensive arthrofibrotic releases. The arm is draped over a radiolucent arm board. However, airway management is more complex, and anterior portal placement can be ergonomically challenging for the surgeon.
3. Supine Suspended: The patient is supine, and the arm is suspended from a sterile traction tower. This provides excellent circumferential access to the elbow and simplifies fluoroscopic imaging.
Regardless of the position, a well-padded proximal arm tourniquet is applied high on the brachium. The limb is exsanguinated, and the tourniquet is inflated to 250 mmHg. A highly specialized fluid management system is utilized, maintaining a low baseline pressure (typically 30-40 mmHg) to minimize fluid extravasation into the forearm compartments, which can precipitate a devastating compartment syndrome. The joint is maximally distended with 15 to 25 mL of normal saline via a spinal needle introduced through the direct lateral "soft spot" before any scalpel incisions are made. This distension is a critical safety step to displace the nerves outward. Skin incisions must be superficial, employing a strict "nick and spread" technique with a small hemostat down to the level of the capsule to avoid transecting superficial cutaneous nerves.
Step-by-Step Surgical Approach and Fixation Technique
Procedure 1: Resection of Thickened Pathological Synovial Plica
The surgical objective is the complete excision of the fibrotic plica while meticulously preserving the lateral ulnar collateral ligament (LUCL) and the native articular cartilage.
1. Diagnostic Arthroscopy: Following joint distension, the anteromedial portal is established first using an inside-out or outside-in technique, depending on surgeon experience. This serves as the primary viewing portal. A thorough diagnostic sweep of the anterior compartment is performed, evaluating the coronoid, trochlea, and anterior radiocapitellar joint.
2. Dynamic Assessment: Under direct visualization, the elbow is ranged through full flexion, extension, pronation, and supination. The surgeon actively looks for the pathological catching or popping of the plica as it snaps across the radiocapitellar joint.
3. Anterior Debridement: The anterolateral portal is established under direct visualization. A 4.0-mm arthroscopic shaver is introduced. The anterior joint space is debrided of inflammatory synovitis, and the anterior extension of the thickened plica is shaved back to healthy tissue.
4. Posterior Compartment Evaluation: The arthroscope is transitioned to the posterolateral portal. Utilizing a 70-degree, 2.7-mm or 4.0-mm arthroscope is highly recommended to navigate the tight, convex confines of the posterior radiocapitellar joint. The main body of the hypertrophic plica is identified in the posterolateral gutter, often appearing as a thick, fibrotic, meniscus-like band.
5. Plica Resection: A direct lateral portal (soft spot portal) is established. An aggressive shaver or a small arthroscopic basket punch is introduced. The pathological tissue is resected piecemeal back to a stable, healthy synovial rim. The surgeon must remain acutely aware of the LUCL, which lies immediately deep and slightly posterior to the plica. Overzealous resection can result in iatrogenic posterolateral rotatory instability (PLRI).
Procedure 2: Arthroscopic Radial Head Resection
The surgical objective is the complete, impingement-free excision of the radial head and neck while preserving the annular ligament and avoiding injury to the posterior interosseous nerve (PIN).
1. Portal Setup and Synovectomy: The arthroscope is placed in the anteromedial portal for a panoramic view of the radiocapitellar joint. An arthroscopic burr (4.0-mm or 5.5-mm, hooded to protect adjacent soft tissues) is introduced through the anterolateral portal. A partial synovectomy and anterior capsulectomy are performed to expose the radial neck and define the safe resection margins.
2. Piecemeal Resection: The resection begins at the articular surface of the radial head. Using the hooded burr, the radial head is decorticated and resected in a piecemeal fashion. The forearm is continuously rotated by an assistant to bring different quadrants of the radial head into the cutting window of the burr.
3. Proximal Extension: The resection must be carried proximally past the level of the sigmoid notch of the ulna. Failure to resect enough of the radial neck is the most common cause of persistent postoperative pain and mechanical block.
4. Preservation of the Annular Ligament: The burr must be kept strictly within the confines of the radial head and neck. Iatrogenic transection of the annular ligament will lead to symptomatic instability.
5. Dynamic Impingement Check: Once visual resection is complete, the burr is removed. The forearm is actively pronated and supinated while the elbow is moved through a full arc of flexion and extension. The surgeon directly observes the resection space from both the anteromedial and posterolateral portals to ensure no residual bony prominences impinge against the ulna or the annular ligament.
Procedure 3: Arthroscopic Management of Elbow Arthrofibrosis
This is one of the most technically demanding procedures in orthopedic surgery, requiring extreme patience and precise spatial awareness due to the contracted, distorted anatomy.
1. Initial Access and Anterior Release: Due to the severely contracted capsule (often holding only 5-6 mL of fluid), portals must be established with extreme caution. A spinal needle is used to locate the joint space, frequently requiring fluoroscopic assistance. Once the anteromedial and anterolateral portals are established, the initial view is invariably obscured by dense, opaque fibrotic tissue.
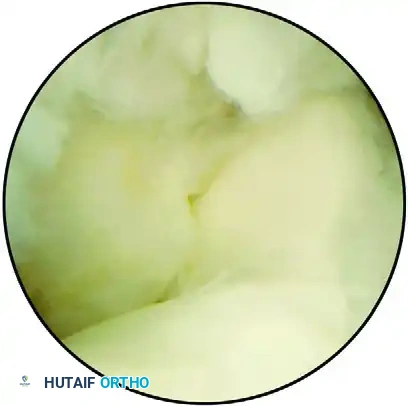
FIGURE 52-70 A: Arthroscopic view of an arthrofibrotic joint. The coronoid is visible on the left and the trochlea on the right, obscured by extensive, dense fibrosis superiorly.
- Anterior Capsulectomy: Using an arthroscopic shaver and a radiofrequency (RF) ablation wand, the fibrotic tissue is systematically resected. The surgeon must work from known anatomical landmarks (e.g., the radiocapitellar joint) towards the unknown. An anterior capsulectomy is performed, meticulously releasing the distal capsular insertion off the anterior humerus. The release is carried medially and laterally until the transverse fibers of the brachialis muscle are clearly visualized, confirming a complete anterior release.
FIGURE 52-70 B: View after the resection of fibrotic tissue and the release of the distal capsular insertion onto the humerus. The underlying bony architecture is revealed, showing the coronoid fossa completely filled by a large, impinging osteophyte.
- Osteophyte Resection and Fossa Recreation: Once the soft tissue contracture is released, the bony blocks to motion become apparent. An arthroscopic burr is introduced to aggressively resect the osteophytes filling the coronoid fossa. The fossa must be deepened and re-created to its native anatomical dimensions to accommodate the coronoid process during terminal flexion.

FIGURE 52-70 C: The coronoid fossa after complete resection of the osteophyte and re-creation of the anatomical fossa. This critical step restores the mechanical clearance necessary to allow full elbow flexion.
- Posterior Compartment Release: The arthroscope is moved to the posterior portals (posterocentral and posterolateral). A posterior capsulectomy is performed, excising any fibrous bands tethering the triceps or obliterating the olecranon recess. Olecranon tip osteophytes are burred away to restore terminal extension. Extreme care must be taken medially to avoid the ulnar nerve, which may be encased in scar tissue. If ulnar nerve symptoms were present preoperatively, an open ulnar nerve decompression and transposition must be performed prior to initiating the arthroscopic posterior release.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, advanced elbow arthroscopy carries a distinct complication profile. The most feared complication is iatrogenic neurovascular injury. Transient nerve palsies (neuropraxias) occur in approximately 2% to 5% of cases, most commonly affecting the superficial radial nerve or the medial antebrachial cutaneous nerve due to portal placement. Permanent motor nerve transection (e.g., the posterior interosseous nerve or median nerve) is rare (<1%) but catastrophic, usually resulting from aggressive anterior capsulectomy with a shaver facing the wrong direction, or from operating in a severely volume-depleted arthrofibrotic joint without adequate visualization.
Heterotopic ossification (HO) is a significant risk, particularly following arthrofibrotic releases, occurring in 3% to 10% of patients. HO can rapidly bridge the joint space, completely negating the intraoperative gains in range of motion. Iatrogenic instability is another major concern; over-resection of the radial head in the presence of an unrecognized MUCL injury leads to gross valgus instability, while aggressive plica resection that violates the LUCL results in posterolateral rotatory instability (PLRI).
| Complication | Estimated Incidence | Mechanism / Risk Factor | Salvage Management / Treatment |
|---|---|---|---|
| Transient Neuropraxia | 2% - 5% | Tourniquet time > 2 hours; fluid extravasation; retractor/portal pressure. | Observation; gabapentinoids; typically resolves in 3-12 weeks. |
| Nerve Transection (PIN/Median/Ulnar) | < 1% | Blind portal placement; aggressive shaver use anteriorly; altered anatomy. | Immediate open microsurgical exploration and primary nerve repair or grafting. |
| Heterotopic Ossification (HO) | 3% - 10% | Severe trauma history; aggressive burring; failure to use prophylaxis. | Wait for maturation (typically 6-12 months), then open or arthroscopic surgical excision. |
| Iatrogenic Instability (PLRI or Valgus) | 1% - 3% | Resection of LUCL during plica removal; Radial head resection with deficient MUCL. | Open ligamentous reconstruction (e.g., palmaris longus autograft for LUCL/MUCL). |
| Recurrent Arthrofibrosis | 10% - 15% | Poor patient compliance with CPM/splinting; inadequate intraoperative release. | Revision arthroscopic release vs. open lateral column procedure; manipulation under anesthesia (MUA). |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of advanced elbow arthroscopy—particularly for arthrofibrosis and radial head resection—is inextricably linked to the rigor and execution of the postoperative rehabilitation protocol. The elbow capsule will aggressively attempt to scar and contract within the first 48 hours post-surgery. Therefore, prolonged immobilization is strictly contraindicated.
Immediate Phase (Days 0-3):
The primary goal is profound analgesia and immediate mobilization. An indwelling interscalene or supraclavicular nerve block is highly recommended, left in place for 48 to 72 hours. This provides the pain-free window necessary to initiate immediate continuous passive motion (CPM). The patient is placed in a CPM machine in the recovery room, and the elbow is ranged continuously. A bulky compressive dressing is applied to manage edema, but a rigid splint is avoided. Cryotherapy is utilized continuously to mitigate hemarthrosis and inflammation.
Intermediate Phase (Weeks 1-6):
Once the nerve block is removed, the patient transitions to aggressive active and active-assisted range of motion (ROM) exercises multiple times daily under the supervision of a specialized upper extremity therapist. The focus is on maintaining the intraoperative arc of motion. Static progressive extension and flexion splints are custom-fabricated and utilized during sleep and rest periods. These splints provide a low-load, prolonged stretch that is critical for permanently elongating the healing collagen fibers of the capsule. Prophylaxis against heterotopic ossification (e.g., Indomethacin 75 mg sustained release daily for 3-6 weeks) is administered for high-risk patients.
Late Phase (Weeks 6-12 and Beyond):
Strengthening is gradually introduced only after the newly acquired ROM is stable, painless, and symmetrical to the intraoperative gains. Premature strengthening can incite an inflammatory flare, leading to recurrent stiffness. Isotonic and isokinetic exercises targeting the triceps, biceps, brachialis, and periscapular stabilizers are initiated. Return to competitive sports, heavy manual labor, or throwing activities is generally permitted between 3 to 6 months, contingent upon the complete resolution of pain, restoration of full functional ROM, and symmetrical dynamic strength.
Summary of Landmark Literature and Clinical Guidelines
The contemporary practice of advanced elbow arthroscopy is heavily informed by several seminal works in the orthopedic literature. The anatomical foundation for safe portal placement was definitively established by O'Driscoll and Morrey, whose cadaveric studies mapped the precise millimeter distances of the radial, median, and ulnar nerves to standard arthroscopic portals, establishing the "nick and spread" technique as an absolute standard of care.
Regarding arthrofibrosis, the landmark study by Gallay et al. (2001) revolutionized the understanding of capsular volume, proving that the fibrotic elbow holds only a fraction of normal fluid (6 mL vs. 15-25 mL), fundamentally altering how surgeons approach initial joint distension and portal establishment in the stiff elbow. Clinical guidelines published by the American Society of Shoulder and Elbow Therapists (ASSET) dictate the absolute necessity of immediate, aggressive postoperative mobilization and the use of static progressive splinting, noting that surgical release without specialized rehabilitation yields universally poor outcomes.
For synovial plica syndrome, the work of Kim et al. and Ruiz et al. has clarified the MRI diagnostic criteria (plica thickness > 3mm) and demonstrated that arthroscopic excision yields excellent outcomes in over 85% of carefully selected patients, provided the LUCL remains uncompromised. Similarly, long-term outcome studies on arthroscopic radial head resection confirm that in the setting of isolated radiocapitellar arthritis with an intact MUCL, arthroscopic excision provides equivalent pain relief and superior functional recovery times compared to traditional open resection, solidifying its place as a definitive, advanced technique in the armamentarium of the modern orthopedic surgeon.
