Mastering Fixation of Monteggia Fractures in Adults
Key Takeaway
Discover the latest medical recommendations for Mastering Fixation of Monteggia Fractures in Adults. Monteggia fractures, defined as an ulna fracture with radial head dislocation, are classified by Bado based on injury patterns. Understanding their diverse pathogenesis, from direct blows to supination forces, is critical. Diagnostic imaging, including plain radiographs and CT scans, precisely evaluates the ulna, radial head, and associated injuries. This thorough assessment is vital for planning the effective fixation of Monteggia fractures.
Introduction and Epidemiology
The Monteggia fracture-dislocation represents a complex traumatic disruption of the forearm axis, classically defined as a fracture of the ulna with an associated dislocation of the radiocapitellar joint. Initially described by Giovanni Battista Monteggia in 1814—prior to the advent of radiography—this injury pattern remains one of the most challenging orthopedic trauma presentations to manage effectively. The term "Monteggia lesion" was later popularized by Bado in 1967 to encompass a broader spectrum of radioulnar disruptions, emphasizing that the functional integrity of the forearm relies heavily on the anatomic relationship between the radius and the ulna.

Monteggia lesions account for approximately 1% to 2% of all forearm fractures in adults. While pediatric Monteggia fractures can occasionally be managed with closed reduction and casting, adult Monteggia fractures are inherently unstable and universally mandate surgical intervention. The demographic distribution is bimodal: high-energy trauma (such as motor vehicle collisions or falls from height) typically affects young adult males, whereas low-energy falls predominantly affect older, osteopenic females.
Bado Classification and Jupiter Subclassification
The Bado classification system categorizes these injuries based on the direction of the radial head dislocation and the angulation of the ulnar fracture.
- Bado Type I: Anterior dislocation of the radial head with an anteriorly angulated fracture of the ulnar diaphysis.
- Bado Type II: Posterior or posterolateral dislocation of the radial head with a posteriorly angulated ulnar fracture.
- Bado Type III: Lateral or anterolateral dislocation of the radial head with a fracture of the ulnar metaphysis.
- Bado Type IV: Anterior dislocation of the radial head with fractures of both the radius and ulna at the diaphyseal level.

In adults, Bado Type II fractures are the most common. Recognizing the complexity of Type II lesions, Jupiter and colleagues introduced a subclassification based on the anatomic location of the ulnar fracture, which directly dictates the surgical approach and plate contouring:
* Type IIa: Fracture involves the distal aspect of the olecranon and the coronoid process.
* Type IIb: Fracture involves the diaphyseal-metaphyseal junction, distal to the coronoid.
* Type IIc: Fracture involves the ulnar diaphysis.
* Type IId: Comminuted fracture extending from the olecranon through the coronoid and into the diaphysis.
Monteggia Equivalent Lesions
Equivalent injuries exhibit variable pathology that mirrors the biomechanical disruption of the Bado system but may lack a classic radiocapitellar dislocation. Examples include isolated fractures of the ulnar diaphysis with a concomitant fracture of the radial neck, or proximal ulnar fractures with a plastic deformation of the radius. Recognizing these equivalents is critical, as they demand the same rigorous surgical principles to restore forearm stability.
Surgical Anatomy and Biomechanics
A profound understanding of proximal forearm anatomy is the foundation of successful Monteggia fracture management. The proximal ulna serves as the foundational strut of the elbow and forearm. The greater sigmoid notch articulates with the trochlea, providing primary elbow stability in the sagittal plane. The lesser sigmoid notch articulates with the radial head, forming the proximal radioulnar joint (PRUJ).

Osseous Architecture
The proximal ulna is not perfectly straight. It exhibits a characteristic Proximal Ulnar Dorsal Angulation (PUDA), which averages 5.7 degrees and is located approximately 47 mm distal to the olecranon tip. Furthermore, the ulna possesses a varus bow. Failure to recreate the PUDA and the varus bow during internal fixation will result in a translational mismatch at the PRUJ, preventing spontaneous reduction of the radial head and leading to chronic radiocapitellar subluxation.
Ligamentous Stabilizers
The annular ligament originates and inserts on the anterior and posterior margins of the lesser sigmoid notch, respectively, encircling the radial head. While it is a primary stabilizer of the PRUJ, the quadrate ligament and the interosseous membrane (IOM) also play critical roles in preventing proximal migration and lateral displacement of the radius.

The lateral ulnar collateral ligament (LUCL) originates from the lateral epicondyle and inserts on the supinator crest of the ulna. In posterior Monteggia lesions (Bado Type II), the LUCL is frequently avulsed or disrupted, leading to posterolateral rotatory instability (PLRI) if not addressed.
Biomechanical Pathogenesis
The exact mechanism of injury dictates the fracture pattern. Bado Type I injuries typically result from a fall on an outstretched arm with forced hyperpronation. As the forearm pronates, the radial head is levered anteriorly against the capitellum, causing the ulna to fail in tension. Bado Type II injuries are hypothesized to occur secondary to an axial load combined with a supination force and a varus moment. The supination force tensions the lateral ligamentous complex; if the ligaments hold, the bone fails, resulting in a posterior fracture-dislocation.

Indications and Contraindications
In the adult population, the diagnosis of a Monteggia fracture is an absolute indication for surgical intervention. Closed management inevitably leads to loss of ulnar reduction, recurrent radial head dislocation, profound loss of motion, and early post-traumatic arthrosis.

| Clinical Scenario | Management Strategy | Rationale and Considerations |
|---|---|---|
| Acute Adult Monteggia Fracture (All Bado Types) | Operative (ORIF of Ulna) | Standard of care. Anatomic restoration of ulnar length and alignment is mandatory to reduce the radial head. |
| Monteggia with Radial Head Fracture | Operative (ORIF Ulna + ORIF/Arthroplasty of Radial Head) | Radial head must be addressed if it blocks reduction or is unfixable (requires arthroplasty). |
| Open Monteggia Fracture | Urgent Operative (I&D + ORIF) | Requires immediate irrigation, debridement, and rigid stabilization to protect soft tissues. |
| Pediatric Monteggia (Plastic Deformation) | Non-Operative (Closed Reduction + Casting) | Acceptable only in children with compliant bone, provided anatomic reduction of the PRUJ is maintained. |
| Medically Unstable Adult Patient | Non-Operative (Splinting / Damage Control) | Absolute contraindication to definitive ORIF. Spanning external fixation may be used for damage control. |
| Active Deep Infection at Surgical Site | Contraindication to Internal Fixation | Requires temporizing external fixation and aggressive antibiotic therapy prior to definitive plating. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning mitigates intraoperative complications. The initial examination must systematically evaluate skin integrity, compartment compartments, and neurovascular status. The posterior interosseous nerve (PIN) is particularly vulnerable to traction injury or direct trauma from the displaced radial head, especially in Bado Type I and III lesions.
Imaging Modalities
Standard orthogonal radiographs of the elbow, forearm, and wrist are mandatory. The "radiocapitellar line" must be assessed on every view; a line drawn through the center of the radial neck should bisect the capitellum regardless of the degree of elbow flexion.

While the ulnar fracture is easily identified on plain films, computed tomography (CT) is highly recommended for all adult Monteggia fractures. CT scanning delineates the extent of comminution, identifies occult coronoid fractures (crucial in Bado Type II lesions), and assesses the radial head for shear fractures or impaction. 3D CT reconstructions are invaluable for understanding the spatial relationship of fracture fragments and planning plate placement.

Equipment Preparation
The surgeon must have a comprehensive armamentarium available:
* Small fragment system (3.5 mm locking compression plates, dynamic compression plates).
* Minifragment system (2.0 mm / 2.7 mm) for coronoid or radial head fixation.
* Pre-contoured proximal ulna plates (essential for capturing the olecranon and accommodating the PUDA).
* Modular radial head arthroplasty system.
* Suture anchors for potential LUCL or annular ligament repair.
* Bone graft (autograft or allograft) for highly comminuted ulnar diaphyseal defects.
Patient Positioning
The preferred setup is the lateral decubitus position. The patient is secured with a beanbag, and the operative arm is draped free over a padded arm support. This position allows unimpeded access to the posterior aspect of the elbow, facilitates gravity-assisted reduction of the radiocapitellar joint in Bado Type II lesions, and provides excellent fluoroscopic visualization.

Alternatively, supine positioning with the arm draped across the chest can be utilized. If this approach is chosen, placing a saline bag under the ipsilateral scapula helps elevate the shoulder and prevents the arm from rolling externally during the procedure. However, the supine position can make maintaining reduction and obtaining orthogonal fluoroscopic views more cumbersome.
Detailed Surgical Approach and Technique
The overarching principle of Monteggia fracture surgery is that the ulna dictates the radius. Anatomic restoration of ulnar length, alignment, and rotation will almost universally result in spontaneous reduction of the radiocapitellar joint.
Incision and Superficial Dissection
A universal posterior approach to the elbow and forearm is utilized. The incision begins proximal to the olecranon tip, curving slightly laterally to avoid the tip itself, and extends distally along the subcutaneous border of the ulnar diaphysis.

Full-thickness fasciocutaneous flaps are elevated. It is critical to avoid creating separate fascial planes, as the posterior skin is prone to necrosis. The internervous plane for proximal extension (if accessing the radial head) lies between the anconeus (radial nerve) and the extensor carpi ulnaris (posterior interosseous nerve).

Historically, the Boyd approach (elevating the supinator and anconeus off the ulna as a single flap) was advocated to expose both the ulna and the proximal radius. However, this approach has a high rate of postoperative radioulnar synostosis. Modern techniques favor fixing the ulna through the standard posterior approach and, if the radial head requires direct intervention, utilizing a separate Kocher (between anconeus and ECU) or Kaplan (between EDC and ECRB) interval to minimize cross-periosteal stripping.
Ulnar Reduction and Fixation
The ulnar fracture site is exposed, and fracture hematoma is debrided. The fracture ends are mobilized. In transverse or short oblique fractures, anatomical reduction is achieved using reduction forceps. In comminuted fractures, length and rotation must be restored indirectly.

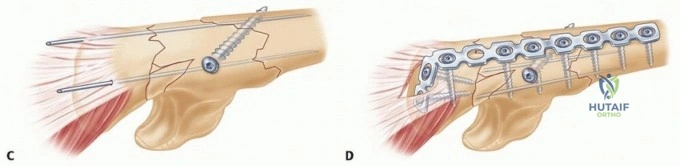
A robust 3.5 mm plate is selected. For proximal fractures (Bado Type II, Jupiter IIa/IIb), a pre-contoured proximal ulna locking plate is ideal. It is applied to the dorsal surface of the ulna. The plate acts as a tension band for proximal fractures and a neutralization or bridge plate for diaphyseal comminution. The surgeon must ensure the PUDA is respected; if a straight plate is applied to a proximal fracture, it will flatten the dorsal angulation, effectively shortening the ulna and causing persistent anterior subluxation of the radial head.

At least six cortices of fixation (three screws) are required proximal and distal to the fracture, though eight cortices are preferred in osteopenic bone. If a coronoid fracture is present, it must be rigidly fixed, either captured by the proximal ulna plate, fixed with independent anterior-to-posterior lag screws, or addressed via a separate medial approach if it involves the anteromedial facet.
Assessment of the Radiocapitellar Joint
Once the ulna is rigidly fixed, the radiocapitellar joint is assessed under direct vision and fluoroscopy. In over 90% of cases, anatomic ulnar fixation results in spontaneous reduction of the radial head.

If the radial head remains dislocated, the surgeon must suspect:
1. Inadequate ulnar reduction (persistent shortening or malrotation).
2. Soft tissue interposition (annular ligament, capsule, or osteochondral fragment).
3. Concomitant radial head or neck fracture.
If soft tissue interposition is suspected, a lateral arthrotomy (Kocher approach) is performed. The interposed annular ligament is extracted from the joint. If the radial head is fractured, it must be addressed. Simple, non-comminuted fractures are treated with ORIF using headless compression screws or a mini-fragment plate applied to the "safe zone" of the radial head.

If the radial head is unfixable (comminuted >3 fragments), a radial head arthroplasty is performed. Excision of the radial head without replacement in the acute trauma setting is strictly contraindicated, as it will lead to proximal migration of the radius and longitudinal forearm instability.
Ligamentous Reconstruction and Closure
Routine repair or reconstruction of the annular ligament is not required if the ulna is anatomically fixed and the radial head is stable through a full range of motion. However, if there is persistent posterolateral rotatory instability (frequently seen in Bado Type II lesions), the lateral ulnar collateral ligament (LUCL) must be repaired to its isometric origin on the lateral epicondyle using suture anchors.

Intraoperative fluoroscopy is utilized to confirm hardware placement, ulnar alignment, and concentric reduction of the PRUJ and radiocapitellar joint in all planes. The wound is irrigated, and the deep fascia is left open to prevent compartment syndrome. Only the subcutaneous tissue and skin are meticulously closed.
Complications and Management
Despite meticulous surgical technique, complications following Monteggia fracture fixation are prevalent. Anticipation and early recognition are paramount for limb salvage.

Neurologic Injury
Posterior interosseous nerve (PIN) palsy is the most common neurologic complication, reported in up to 10-17% of cases. It is most frequently associated with Bado Type I and III lesions due to anterior or lateral displacement of the radial head stretching the nerve against the supinator muscle. The vast majority of these are neurapraxias that resolve spontaneously within 3 to 6 months. Iatrogenic PIN injury can occur during radial head exposure; staying within the Kocher interval and avoiding aggressive anterior retraction minimizes this risk.
Malunion and Nonunion
Ulnar nonunion or malunion typically results from inadequate fixation, failure to recognize comminution, or failure to restore the PUDA. A malunited ulna inevitably leads to chronic radial head subluxation, restricted forearm rotation, and pain.

Management of a chronic Monteggia lesion requires a complex reconstructive procedure: ulnar osteotomy, structural bone grafting to restore length and bow, rigid internal fixation, and open reduction of the radial head. If the radial head is deformed from chronic dislocation, radial head excision or arthroplasty may be necessary.
Radioulnar Synostosis
Heterotopic ossification leading to cross-union between the radius and ulna is a devastating complication that abolishes forearm pronation and supination. Risk factors include delayed surgery, extensive periosteal stripping, severe head trauma, and utilizing a single surgical approach (Boyd) to access both bones. Treatment requires delayed surgical excision of the synostosis (once the bone scan is "cold" and margins are distinct) combined with prophylactic radiation or indomethacin.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Strategy |
|---|---|---|---|
| PIN Palsy | 10% - 17% | Traction from radial head dislocation; Iatrogenic retraction. | Observation for 3-6 months. EMG at 6 weeks. Tendon transfers if no recovery by 1 year. |
| Ulnar Nonunion | 2% - 5% | Inadequate fixation; Infection; Severe comminution. | Revision ORIF with rigid plating and autologous bone grafting. |
| Chronic Radial Head Dislocation | 5% - 10% | Failure to restore ulnar length/PUDA; Missed annular ligament interposition. | Ulnar corrective osteotomy, open reduction of radial head, possible annular ligament reconstruction. |
| Radioulnar Synostosis | 3% - 8% | Boyd approach; Delayed surgery; Massive soft tissue trauma. | Excision of heterotopic bone at 6-12 months post-injury, interposition of fat/muscle, NSAID prophylaxis. |
| Hardware Prominence | 15% - 20% | Subcutaneous nature of the proximal ulna; Bulky plates. | Hardware removal after complete radiographic union (minimum 12-18 months). |
Post Operative Rehabilitation Protocols
The primary goal of postoperative rehabilitation is to restore functional range of motion while protecting the osseous fixation and ligamentous repairs. Prolonged immobilization is detrimental and leads to profound elbow stiffness.

Acute Phase (0 to 2 Weeks)
Immediately postoperatively, the arm is placed in a well-padded posterior splint with the elbow at 90 degrees of flexion and the forearm in neutral rotation. If a Bado Type I (anterior) lesion was repaired, the forearm may be splinted in supination to relax the biceps and reduce anterior pull on the radius. If a Bado Type II (posterior) lesion was repaired, the forearm is splinted in pronation to improve radiocapitellar stability.
Sutures are removed at 10 to 14 days. If fixation is rigid and the joint is stable, the patient is transitioned to a hinged elbow brace.
Intermediate Phase (2 to 6 Weeks)
Active and active-assisted range of motion (ROM) exercises for elbow flexion/extension and forearm
Clinical & Radiographic Imaging

