Navigating Monteggia Fractures in Adults: What You Need to Know
Key Takeaway
Here are the crucial details you must know about Navigating Monteggia Fractures in Adults: What You Need to Know. Monteggia lesions are a type of fracture in adults defined as a fracture of the ulna associated with a dislocation of the radiocapitellar joint. Equivalent injuries in adults are variable pathologies that may not always include a radiocapitellar dislocation but are categorized by the Bado classification, particularly Type I and II patterns.
Introduction and Epidemiology
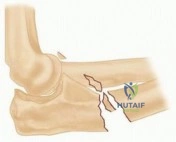
The Monteggia fracture-dislocation represents a complex injury pattern of the forearm and elbow that demands precise anatomic understanding and meticulous surgical execution. Initially described by Giovanni Battista Monteggia in 1814, the classic definition encompasses a fracture of the ulna associated with an anterior dislocation of the radial head. However, the contemporary understanding of this pathology has evolved significantly. In 1967, Jose Luis Bado introduced the term "Monteggia lesion" to describe a broader spectrum of injuries involving a fracture of the ulna at any level combined with a dislocation of the radiocapitellar joint in any direction.
Monteggia lesions are relatively uncommon, accounting for approximately 1% to 2% of all forearm fractures in the adult population. Unlike the pediatric demographic, where Type I and Type III lesions predominate and closed reduction is often successful, adult Monteggia fractures are predominantly Bado Type II (posterior dislocation) and almost universally require operative intervention.
Bado Classification System
The Bado classification system categorizes these injuries based on the direction of the radial head dislocation and the apex of the ulnar fracture angulation.
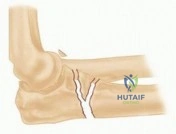
- Bado Type I: Anterior dislocation of the radial head with fracture of the ulnar diaphysis at any level with anterior angulation.
- Bado Type II: Posterior or posterolateral dislocation of the radial head with fracture of the ulnar diaphysis with posterior angulation.
- Bado Type III: Lateral or anterolateral dislocation of the radial head with fracture of the ulnar metaphysis.
- Bado Type IV: Anterior dislocation of the radial head with fracture of the proximal third of the radius and fracture of the ulna at the same level.
Jupiter Subclassification of Type II Lesions
Given the prevalence and complexity of Bado Type II fractures in adults, Jupiter and colleagues developed a subclassification based on the anatomic location and fracture pattern of the ulna, which directly dictates the surgical approach and fixation strategy.
- Type IIA: Involves the distal part of the olecranon and the coronoid process.
- Type IIB: Involves the diaphyseal-metaphyseal junction, distal to the coronoid process.
- Type IIC: Involves the diaphyseal shaft of the ulna.
- Type IID: Complex, comminuted fractures extending from the olecranon through the coronoid and into the diaphysis.
Monteggia Equivalent Injuries
Equivalent injuries exhibit variable pathology that aligns biomechanically with the Bado system but may lack the traditional concomitant radiocapitellar dislocation. Examples include an isolated dislocation of the radial head without a distinct ulnar fracture (often associated with plastic deformation of the ulna in pediatrics, but rare in adults), or an ulnar diaphyseal fracture combined with a radial neck fracture. Recognizing these equivalents is critical, as the fundamental principle of restoring ulnar length to stabilize the radiocapitellar joint remains the primary surgical objective.
Surgical Anatomy and Biomechanics
A profound understanding of proximal radioulnar and radiocapitellar anatomy is essential for the successful management of Monteggia lesions. The proximal ulna serves as the foundational strut of the forearm. The olecranon and coronoid processes form the greater sigmoid notch, articulating with the trochlea to provide primary sagittal plane stability to the elbow.
Proximal Ulna Osteology
The proximal ulna is not a perfectly straight bone. It possesses a characteristic proximal ulna dorsal angulation (PUDA), which averages 5.7 degrees and is located approximately 47 millimeters distal to the tip of the olecranon. Furthermore, there is a physiological varus bow. Failure to recognize and anatomically restore the PUDA and the varus bow during osteosynthesis will result in a translational mismatch at the radiocapitellar joint, leading to persistent subluxation or dislocation of the radial head.
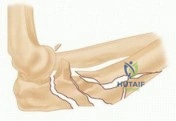
Ligamentous Anatomy
The stability of the radiocapitellar joint relies on both osseous architecture and the lateral collateral ligament (LCL) complex. The LCL complex originates from the lateral epicondyle and consists of the radial collateral ligament, the lateral ulnar collateral ligament (LUCL), and the annular ligament. The LUCL is the primary restraint to posterolateral rotatory instability (PLRI). In Monteggia fractures, particularly Bado Type II, the radial head dislocation often results in avulsion or mid-substance tearing of the LCL complex, necessitating evaluation and potential repair following osseous fixation.
Pathogenesis and Biomechanics
The exact mechanism of injury for Monteggia fractures remains a subject of biomechanical debate, with distinct mechanisms proposed for different Bado types.
- Bado Type I Pathogenesis: Historically attributed to a direct blow to the posterior aspect of the forearm (the "nightstick" mechanism). However, Evans proposed a hyperpronation theory, where a fall on an outstretched hand (FOOSH) with a hyperpronated forearm levers the radial head anteriorly, subsequently fracturing the ulna in tension. Another theory involves violent contraction of the biceps brachii, forcefully pulling the radial head anteriorly during a fall.
- Bado Type II Pathogenesis: Predominantly occurs via a FOOSH mechanism with the elbow flexed. A supination force is applied to the forearm, tensioning the lateral ligamentous structures. If the ligaments prove stronger than the bone, the force propagates through the radiocapitellar joint, dislocating the radial head posteriorly and resulting in a failure of the proximal ulna in tension.
- Bado Type III Pathogenesis: Typically results from a direct blow to the medial aspect of the elbow, or a severe varus stress applied to the extended elbow, driving the radial head laterally.

Indications and Contraindications
In the adult population, the diagnosis of a Monteggia fracture-dislocation is an absolute indication for operative management. Nonoperative management historically yields dismal results, characterized by ulnar malunion, chronic radiocapitellar dislocation, severe restricted range of motion, and early onset post-traumatic osteoarthritis.
Operative vs Non Operative Management Parameters
| Management Strategy | Indications | Contraindications | Expected Outcomes |
|---|---|---|---|
| Operative (ORIF) | All acute adult Monteggia fractures; Bado Types I-IV; Monteggia equivalents; Open fractures (after debridement). | Active systemic infection; Medically unstable patient unfit for anesthesia; Severe soft tissue compromise precluding immediate internal fixation (requires temporizing ex-fix). | Restoration of ulnar length, spontaneous reduction of radial head, early mobilization, return to pre-injury function. |
| Non-Operative | Strictly limited to patients with unacceptable surgical/anesthetic risk; Non-ambulatory patients with minimal functional demands. | Acute, displaced fractures in healthy, functional adults; Any radiocapitellar subluxation. | Ulnar malunion/nonunion, chronic radial head dislocation, severe pain, restricted supination/pronation. |
The timing of surgical intervention is dictated by the condition of the soft tissue envelope. Severe swelling, fracture blisters, or open wounds may necessitate a staged approach, utilizing a spanning external fixator to maintain length and gross alignment until the soft tissues are amenable to definitive internal fixation.

Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is paramount. The surgeon must systematically evaluate the skin integrity, neurovascular status, and the precise bony morphology.
Imaging Protocols
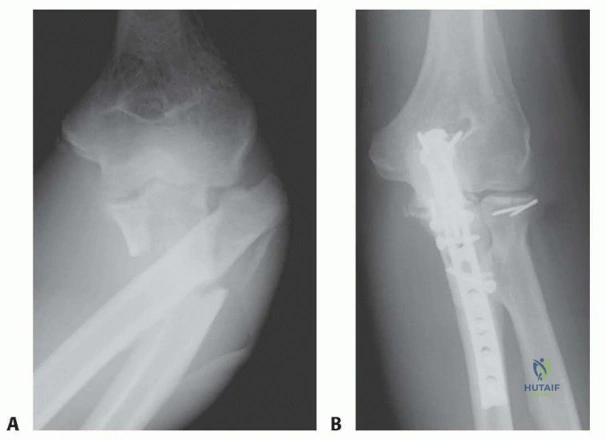
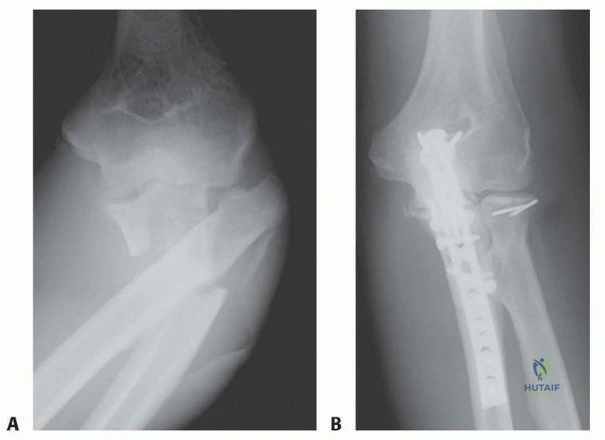
Standard orthogonal plain radiographs of the elbow, forearm, and wrist are mandatory. The ulnar fracture is typically obvious; however, the radial head dislocation can be subtle, particularly if it has spontaneously reduced. A true lateral radiograph of the elbow is critical: a line drawn through the center of the radial shaft and head (the radiocapitellar line) must intersect the center of the capitellum in all degrees of flexion and extension.
Computed tomography (CT) scans with 3D reconstructions are highly recommended, especially for Bado Type II fractures and Jupiter subclassifications. CT imaging delineates the extent of comminution, identifies occult coronoid fractures, and provides a spatial map for plate templating.

Equipment Requirements
The operating room must be equipped with a comprehensive array of hardware. Standard requirements include 3.5mm dynamic compression plates (DCP), limited contact dynamic compression plates (LC-DCP), and pre-contoured proximal ulna locking plates. Mini-fragment systems (1.5mm to 2.7mm) are essential for coronoid and radial head fixation. A radial head arthroplasty system must be available in the room, as comminuted radial head fractures (often seen in Bado Type IV or complex Type II) may be unrepairable. Autograft or allograft bone should be available to address structural voids in comminuted metaphyseal segments.

Patient Positioning
The lateral decubitus position is widely preferred by orthopedic traumatologists. The patient is placed in the lateral decubitus position with the operative arm draped over a padded L-bar or radiolucent arm support. This position allows unobstructed access to the posterior aspect of the elbow and proximal ulna, facilitates gravity-assisted reduction of posterior radial head dislocations, and provides excellent fluoroscopic visualization.

Alternatively, supine positioning can be utilized. The arm is brought across the chest for the posterior approach. Placing a saline bag or bump under the ipsilateral scapula assists in maintaining the arm position. While feasible, supine positioning often requires an assistant to hold the arm and can make intraoperative fluoroscopy more cumbersome compared to the lateral decubitus setup.
Detailed Surgical Approach and Technique
The fundamental tenet of Monteggia fracture surgery is that "the ulna dictates the radius." Anatomic restoration of ulnar length, alignment, and rotation will almost invariably result in spontaneous reduction of the radiocapitellar joint.
Surgical Approaches
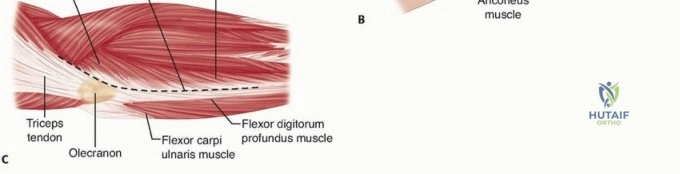
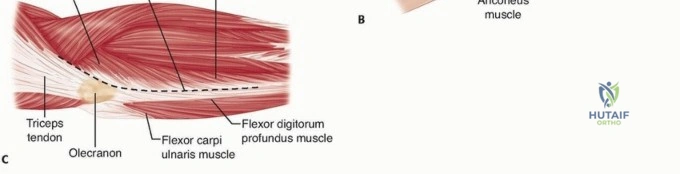
A universal posterior approach to the elbow and forearm is the workhorse incision. A longitudinal incision is made slightly lateral to the tip of the olecranon, curving medially to avoid the tip, and extending distally along the subcutaneous border of the ulna. Full-thickness fasciocutaneous flaps are elevated.
The internervous plane for proximal ulnar exposure lies between the extensor carpi ulnaris (ECU), innervated by the posterior interosseous nerve (PIN), and the flexor carpi ulnaris (FCU), innervated by the ulnar nerve. If access to the radial head is required, the Kocher approach (between the anconeus and ECU) or the Kaplan approach (between the extensor digitorum communis and extensor carpi radialis brevis) can be utilized through the same posterior skin incision by elevating a lateral flap.

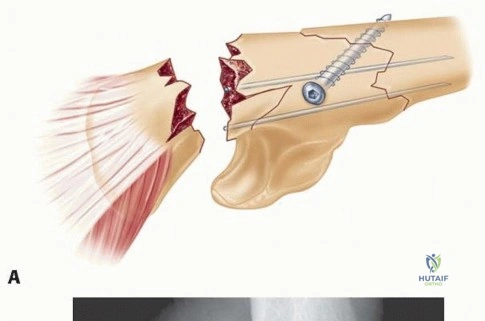
Ulnar Osteosynthesis
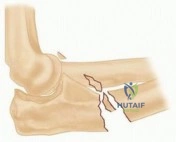
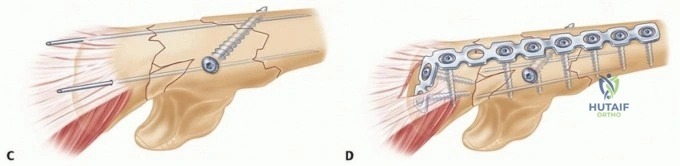
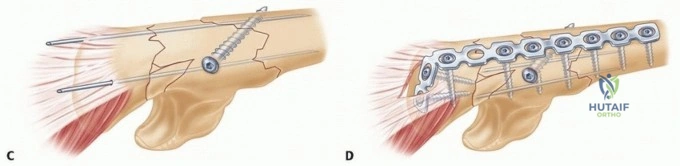
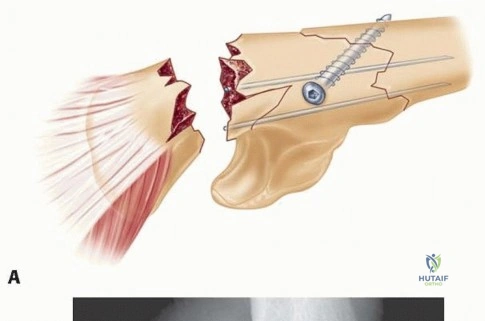
The fracture site is exposed, and hematoma is evacuated. In simple fracture patterns (Jupiter Type IIC), anatomic reduction is achieved using reduction forceps, and absolute stability is obtained via a 3.5mm LC-DCP applied in compression mode. The plate is typically positioned on the posterior or tension band surface of the ulna.
For comminuted or proximal metaphyseal fractures (Jupiter Type IIA, IIB, IID), a pre-contoured proximal ulna locking plate is preferred. The PUDA must be meticulously restored. If the fracture involves the coronoid process, it must be reduced and stabilized either with lag screws extending from the posterior ulnar plate or via a separate anterior approach, as coronoid incompetence will lead to persistent elbow instability.

Radiocapitellar Assessment and Radial Head Management
Following rigid ulnar fixation, the radiocapitellar joint is assessed under direct vision and fluoroscopy. In the majority of cases, anatomic ulnar fixation results in concentric reduction of the radial head.
If the radial head remains dislocated, the surgeon must systematically evaluate for:
1. Ulnar Malreduction: Even a few millimeters of shortening or a slight angular deformity can prevent radial head reduction. The ulnar fixation must be critically reassessed and revised if necessary.
2. Interposed Soft Tissue: The annular ligament, capsule, or osteochondral fragments may be incarcerated within the radiocapitellar joint. An arthrotomy via a Kocher approach is required to extract the interposed tissue.
3. Radial Head Fracture: If a concomitant radial head fracture is present, it must be addressed. Small, non-articulating fragments can be excised. Reparable fractures should undergo ORIF with headless compression screws or mini-fragment plates. If the radial head is severely comminuted (more than 3 parts) and unrepairable, radial head arthroplasty is indicated to restore the lateral column strut.

Soft Tissue Reconstruction
Once the bony architecture is restored and the radiocapitellar joint is concentrically reduced, stability is assessed through a full range of motion, particularly noting stability in pronation and supination. If the radial head subluxates in terminal extension and supination, LUCL incompetence is highly likely. The LUCL is identified at its isometric origin on the lateral epicondyle and repaired using suture anchors. The annular ligament can often be primarily repaired, though its reconstruction is secondary in importance to LUCL repair and osseous alignment.

Complications and Management
Despite meticulous surgical technique, Monteggia fractures are associated with a significant complication profile. Anticipation and early recognition are vital for joint preservation.
Peripheral Nerve Injuries
Neurologic injury is common, particularly involving the posterior interosseous nerve (PIN). The PIN is highly vulnerable as it courses through the arcade of Frohse and wraps around the radial neck. PIN palsy is most frequently observed in Bado Type I and Type III injuries due to the anterior or lateral displacement of the radial head stretching the nerve.
The vast majority of these injuries are neuropraxias secondary to traction or contusion. The standard management is watchful waiting. Electromyography (EMG) and nerve conduction velocities (NCV) can be obtained at 6 to 12 weeks if no clinical improvement is noted. Iatrogenic nerve injury during the surgical approach (particularly the anterior approach to the radius) must be avoided by maintaining strict adherence to internervous planes and avoiding aggressive retraction.

Malunion and Chronic Dislocation
The most devastating complication is ulnar malunion leading to chronic radiocapitellar dislocation. This almost exclusively results from failure to restore the anatomic length and PUDA of the proximal ulna during the index procedure.
Patients present with restricted range of motion, progressive valgus deformity, and elbow pain. Management requires a complex reconstructive procedure involving a corrective ulnar osteotomy. The ulna is osteotomized, lengthened, and angularly corrected to restore the normal radiocapitellar relationship. Bone grafting is typically required, followed by rigid internal fixation. Open reduction of the radial head and extensive capsular release are performed concurrently.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Etiology | Management / Salvage Strategy |
|---|---|---|---|
| PIN Palsy | 10% - 20% | Traction from radial head dislocation (Bado I/III) or iatrogenic retractor injury. | Observation. Baseline EMG at 6 weeks. Tendon transfers if no recovery by 6-12 months. |
| Ulnar Nonunion | 2% - 5% | Inadequate fixation, infection, severe comminution with devascularization. | Revision ORIF with autologous bone grafting (iliac crest). Rule out indolent infection. |
| Radiocapitellar Subluxation | 5% - 10% | Unrecognized ulnar malreduction (shortening or angulation); LUCL incompetence. | Acute: Revision ulnar osteosynthesis and/or LUCL repair. Chronic: Ulnar corrective osteotomy. |
| Heterotopic Ossification | 5% - 15% | Severe soft tissue trauma, delayed surgery, concurrent head injury. | Prophylaxis with Indomethacin or single-fraction radiation in high-risk patients. Surgical excision after maturation (12-18 months). |
| Radioulnar Synostosis | 1% - 3% | Disruption of interosseous membrane, hematoma ossification between radius and ulna. | Surgical excision of synostosis with interposition of fat or synthetic barrier; high recurrence rate. |

Post Operative Rehabilitation Protocols
The primary goal of postoperative rehabilitation is to restore functional range of motion while protecting the osteosynthesis and ligamentous repairs. The protocol is highly dependent on the stability of the fixation and the status of the lateral ligamentous complex.
Phase One Early Protection
Immediately postoperatively, the arm is placed in a well-padded posterior splint with the elbow flexed to 90 degrees. The forearm rotation position depends on the specific injury pattern and repair:
* If an LUCL repair was performed, the forearm is typically splinted in pronation to relax the lateral structures.
* If the injury was a Bado Type I (anterior dislocation), the forearm may be splinted in supination.
At 7 to 14 days, the splint is removed, and sutures are evaluated. If rigid internal fixation was achieved, early active and active-assisted range of motion (ROM) is initiated. A hinged elbow brace with an extension block may be utilized if there are concerns regarding soft tissue stability.
Phase Two Progressive Mobilization
From 2 to 6 weeks, the focus shifts to regaining terminal extension and full pronation/supination. Passive stretching is generally avoided to minimize the risk of heterotopic ossification. Strengthening exercises are contraindicated during this phase to prevent displacement of the ulnar fracture prior to clinical union.
Phase Three Strengthening
At 6 to 8 weeks, radiographic evaluation is performed to confirm progression of callus formation and maintenance of radiocapitellar reduction. Once clinical and radiographic union is evident, progressive isometric and isotonic strengthening of the biceps, triceps, and forearm musculature is initiated. Full return to unrestricted heavy labor or contact sports may require 4 to 6 months.

Summary of Key Literature and Guidelines
The modern surgical approach to Monteggia fractures is heavily influenced by foundational literature emphasizing precise anatomic restoration.
Jupiter et al. fundamentally changed the approach to adult Monteggia fractures by identifying the high failure rate of simple diaphyseal plating techniques when applied to complex proximal ulnar fractures. Their subclassification of Bado Type II lesions highlighted the necessity of contoured plating that captures the coronoid and restores the proximal ulnar dorsal angulation.
Ring, Jupiter, and Simpson further reinforced the concept that the ulna acts as the critical strut for the forearm. Their retrospective reviews demonstrated that nearly all cases of persistent radial head dislocation post-ORIF were directly attributable to subtle ulnar malreductions, specifically shortening or failure to restore the normal varus bow.
Current academic guidelines strongly advocate for:
1. Immediate operative intervention in medically stable adults.
2. Utilization of pre-contoured locking plates for proximal third ulnar fractures.
3. Direct visualization and dynamic intraoperative fluoroscopic assessment of the radiocapitellar joint following ulnar fixation.
4. A low threshold for radial head arthroplasty in the setting of severe radial head comminution to prevent proximal radial migration and subsequent radiocapitellar instability.
Clinical & Radiographic Imaging