Dupuytren's: Preventing Damage to Your Distal Interphalangeal Joint

Key Takeaway
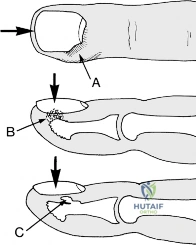
Discover the latest medical recommendations for Dupuytren's: Preventing Damage to Your Distal Interphalangeal Joint. Dupuytren's Contracture involves nodular thickening and contracture of the palmar fascia, mainly affecting men over 40. It causes progressive finger flexion, often of the ring and little fingers, impairing hand function. Severe, prolonged flexion can lead to secondary changes in interphalangeal joints, including the distal interphalangeal joint, potentially preventing finger extension even after surgical tissue removal.
Comprehensive Introduction and Patho-Epidemiology
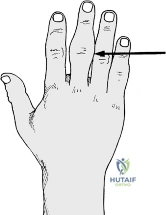
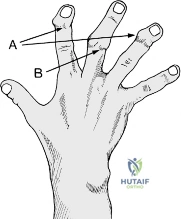
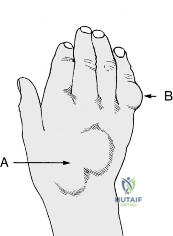
The preservation of hand function, particularly the intricate kinematics of the distal interphalangeal (DIP) and proximal interphalangeal (PIP) joints, is a paramount objective in orthopedic hand surgery. Dupuytren’s disease, a progressive fibroproliferative disorder of the palmar fascia, serves as a primary paradigm for understanding how soft tissue contractures can irreversibly damage joint mechanics. The condition initially manifests as nodular thickening in the palm, subsequently organizing into pathological cords that tether the digits in progressive flexion. While the ring finger is most frequently implicated, followed sequentially by the little, middle, index fingers, and occasionally the thumb, the insidious nature of the disease lies in its secondary effects on the interphalangeal articulations. Prolonged flexion contractures lead to capsular contractures, collateral ligament shortening, and articular cartilage degeneration, rendering joint salvage exceedingly difficult even after the offending fascial cords have been excised.
Epidemiologically, Dupuytren’s contracture exhibits a striking demographic and geographic predilection. It predominantly afflicts men over the age of 40, particularly those of Northern European descent, while remaining conspicuously rare in populations across Africa, India, and China. A robust genetic predisposition is identifiable in 60% to 70% of cases, often inherited in an autosomal dominant pattern with variable penetrance. Furthermore, the condition is frequently associated with systemic comorbidities, including diabetes mellitus, epilepsy (often linked to barbiturate use), and alcoholic cirrhosis. The concept of a "Dupuytren's diathesis" describes a particularly aggressive phenotype characterized by early onset (under age 40), bilateral involvement, and ectopic fibromatosis such as plantar fibromatosis (Ledderhose disease), penile fibromatosis (Peyronie’s disease), and dorsal knuckle pads (Garrod’s nodes). In younger patients, or regardless of sex, the onset or acceleration of the disease may be precipitated by localized trauma, leading to a remarkably rapid and recalcitrant clinical course.
Beyond Dupuytren's contracture, the interphalangeal joints are perpetually threatened by a myriad of other pathologies, ranging from environmental exposures to autoimmune destruction. Prolonged exposure to high-frequency vibration—endemic in occupations utilizing jackhammers, riveting machines, or hand-held buffers—precipitates Hand-Arm Vibration Syndrome (HAVS). This condition systematically dismantles the neurovascular and osteologic integrity of the hand, leading to episodic blanching, profound proprioceptive loss, and debilitating clumsiness. Similarly, systemic inflammatory arthropathies like Rheumatoid Arthritis (RA) target the synovial lining of joints and tendon sheaths, driving aggressive joint subluxation, tendon rupture, and catastrophic deformity. Conversely, primary Osteoarthritis (OA) manifests with focal cartilage loss and osteophyte formation, classically presenting as Heberden’s nodes at the DIP joints and Bouchard’s nodes at the PIP joints.
Finally, the structural integrity of the hand is frequently compromised by acute traumatic tendon lesions, space-occupying neoplasms, and aggressive pyogenic infections. Extensor mechanism disruptions, such as the mallet finger or boutonnière deformity, fundamentally alter the balance of forces across the interphalangeal joints, necessitating meticulous splinting or surgical reconstruction. Benign and malignant tumors, ranging from simple ganglions and mucous cysts to intraosseous enchondromas and metastatic deposits, can erode bone stock and compress neurovascular bundles. Infections, particularly suppurative flexor tenosynovitis or deep space abscesses, pose an immediate threat to digit survival, requiring emergent surgical decompression to prevent tendon necrosis and irreversible joint stiffness.
Detailed Surgical Anatomy and Biomechanics
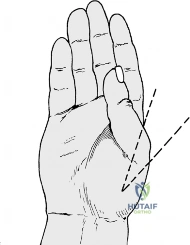
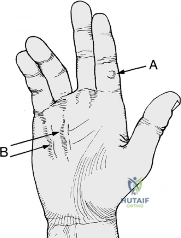
A profound mastery of the normal and pathological anatomy of the palmar fascia is non-negotiable for the operating surgeon. The normal palmar fascia consists of pretendinous bands, the superficial transverse palmar ligament, natatory ligaments, and the lateral digital sheets. In Dupuytren’s disease, these normal fascial structures undergo myofibroblast-mediated hypertrophy to become pathological cords. The central cord, arising from the pretendinous band, primarily causes metacarpophalangeal (MCP) joint contracture. The spiral cord—a complex amalgamation of the pretendinous band, spiral band, lateral digital sheet, and Grayson’s ligament—is notorious for causing PIP joint contracture. Crucially, as the spiral cord hypertrophies, it displaces the neurovascular bundle centrally and superficially, placing the digital nerve at extreme risk during surgical dissection. Contracture of the DIP joint, though less common, is typically driven by the retrovascular cord, which courses dorsal to the neurovascular bundle and inserts into the distal phalanx.

The biomechanics of the extensor mechanism are equally intricate and highly susceptible to disruption. The extensor digitorum communis (EDC) tendon trifurcates over the proximal phalanx into a central slip, which inserts onto the base of the middle phalanx to extend the PIP joint, and two lateral bands. The lateral bands converge dorsally to form the terminal tendon, which inserts onto the distal phalanx to extend the DIP joint. Avulsion of the terminal tendon, often with a bony fragment, results in a mallet finger—characterized by a profound inability to actively extend the DIP joint. Conversely, attenuation or laceration of the central slip allows the lateral bands to subluxate volarly past the axis of rotation of the PIP joint. This biomechanical disaster converts the lateral bands from PIP extensors into PIP flexors, while paradoxically increasing their extensor pull on the DIP joint, culminating in the classic boutonnière deformity.
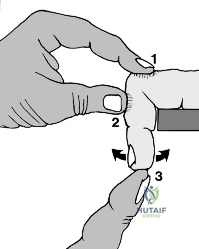
The flexor tendon system is governed by a precise arrangement of synovial sheaths and fibrous retinacular pulleys. The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons glide within a tightly constrained fibro-osseous canal. The FDS bifurcates at Camper’s chiasm to allow the FDP to pass superficially and insert into the base of the distal phalanx. The pulley system, comprising five annular (A1-A5) and three cruciform (C1-C3) pulleys, prevents tendon bowstringing. Trigger finger (stenosing tenosynovitis) arises from a size mismatch between the flexor tendon and the A1 pulley, often due to nodular thickening within the tendon itself or fibrocartilaginous metaplasia of the pulley. When the digit is extended, the nodule struggles to pass through the A1 pulley, causing the digit to lag before suddenly "triggering" into extension.
The synovial spaces of the hand dictate the catastrophic spread of deep infections. The flexor tendon sheaths of the index, middle, and ring fingers typically terminate at the level of the metacarpal necks. However, the synovial sheath of the little finger communicates proximally with the ulnar bursa, while the thumb sheath communicates with the radial bursa. In approximately 70% of individuals, there is a direct communication between the radial and ulnar bursae proximal to the carpal tunnel (the "horseshoe" connection). Consequently, an untreated infection in the little finger can rapidly spread to the thumb, and vice versa, leading to a devastating horseshoe abscess that threatens the entire hand.
Exhaustive Indications and Contraindications
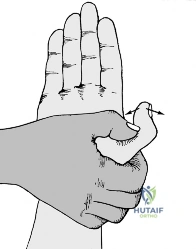
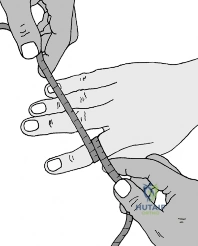
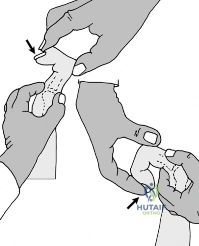
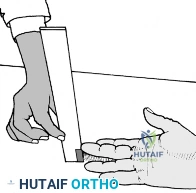
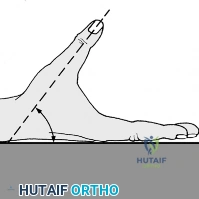
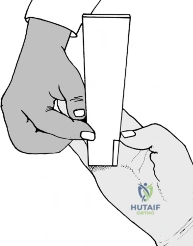
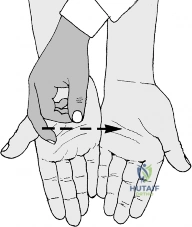
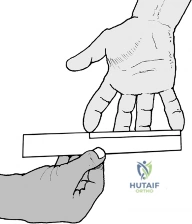
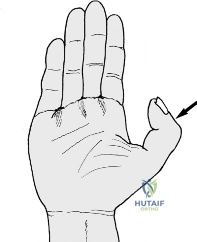
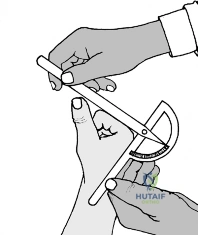
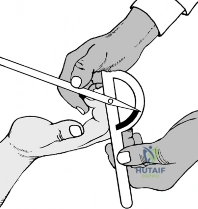
Surgical intervention in the hand requires a rigorous algorithmic approach, balancing the natural history of the disease against the inherent risks of surgery. For Dupuytren’s disease, a mere presence of palmar nodules is not an indication for surgery; a conservative "wait and see" policy is mandated. The classic indication for surgical fasciectomy is a positive Hueston’s tabletop test—the inability of the patient to place their palm completely flat on a hard surface. Quantitatively, surgery is generally advised for MCP joint contractures exceeding 30 degrees, or any degree of PIP or DIP joint contracture, as interphalangeal joint contractures are notoriously resistant to correction if left untreated. In cases of severe, long-standing PIP joint flexion where secondary capsular changes have occurred, simple fasciectomy may fail to restore extension, necessitating concurrent joint release or, in extreme cases involving the little finger, amputation.
Tendon injuries similarly demand precise surgical decision-making. Mallet fingers are predominantly treated non-operatively with strict, continuous DIP joint extension splinting for 6 to 8 weeks. However, surgical pinning or repair is indicated if there is volar subluxation of the distal phalanx or if the avulsed bony fragment encompasses more than 30% to 50% of the articular surface. Profundus tendon lacerations (Zone II injuries, historically termed "no man's land") require meticulous primary repair by an experienced surgeon within the first few weeks; delayed presentations or heavily contaminated wounds may necessitate staged free flexor tendon grafting. Extensor tendon divisions on the dorsum of the hand carry an excellent prognosis and are universally indicated for primary suture followed by 4 weeks of splintage.
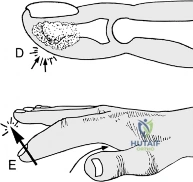
The management of hand tumors and infections is dictated by the threat to adjacent structures. Implantation dermoid cysts, ganglions, and highly vascular, exquisitely painful glomus tumors located in the nail bed are absolute indications for complete surgical excision. Mucous cysts, which invariably communicate with an osteoarthritic DIP joint, should generally be left alone unless they threaten skin viability, rupture to form a synovial fistula, or cause severe nail deformity; excision must include the underlying joint osteophyte to prevent recurrence. For infections, the presence of fluctuance in a paronychia or apical infection mandates immediate incision and drainage. Suppurative flexor tenosynovitis is a surgical emergency indicated by Kanavel’s four cardinal signs: flexed posture of the digit, fusiform swelling, severe pain with passive extension, and exquisite tenderness along the tendon sheath.
| Condition | Primary Indications for Surgery | Relative / Absolute Contraindications |
|---|---|---|
| Dupuytren’s Contracture | MCP flexion > 30°; Any PIP/DIP contracture; Positive tabletop test. | Palmar nodules only; Severe medical comorbidities; Non-compliant patient. |
| Mallet Finger | Volar subluxation of DIP; Bony fragment > 30-50% of articular surface. | Closed tendinous avulsion (treat with strict splinting for 6-8 weeks). |
| Zone II FDP Laceration | Acute, clean laceration within 1-3 weeks of injury. | Heavily contaminated crush injury; Delayed presentation > 4 weeks (requires graft). |
| Trigger Finger | Failure of corticosteroid injections; Locked digit. | Mild, intermittent triggering resolving with rest/NSAIDs. |
| Mucous Cyst | Impending skin necrosis; Synovial fistula; Severe nail deformity. | Asymptomatic cyst without skin compromise. |
| Flexor Tenosynovitis | Presence of Kanavel's signs; Failure of IV antibiotics within 12-24 hours. | Cellulitis without deep space or sheath involvement. |
Pre-Operative Planning, Templating, and Patient Positioning
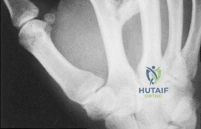
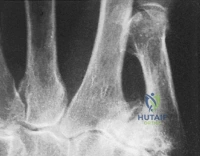
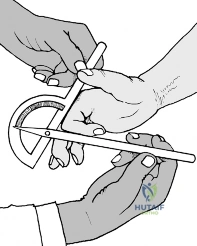
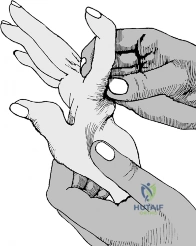
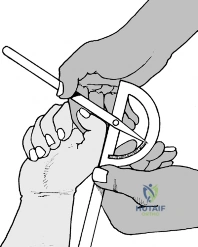
Thorough pre-operative planning begins with a meticulous physical examination and appropriate diagnostic imaging. In Dupuytren's disease, the surgeon must map the palpable cords, noting skin involvement, pitting, and the degree of fixed joint contracture. Vascular status must be assessed using the Allen test to ensure dual blood supply to the hand, as digital arteries may be encased in the fibrotic cords or inadvertently injured during dissection. Neurologic baseline mapping is critical, particularly assessing two-point discrimination, to document pre-existing deficits. For tumors such as osteoid osteomas or enchondromas, plain radiographs are essential. An osteoid osteoma typically presents as a radiolucent nidus surrounded by dense sclerotic bone in a distal phalanx, and an isotope bone scan will reveal an intense "hot spot." Enchondromas appear as expansile, centrally located radiolucent lesions with stippled calcification within the phalanges or metacarpals.
Classifying Vibration Syndromes: Taylor–Pelmear Scale
For patients presenting with suspected Hand-Arm Vibration Syndrome, a comprehensive occupational history is paramount. The differential diagnosis is broad and includes Raynaud’s disease, cervical rib, costoclavicular syndrome, cervical spondylosis, and beta-blocker sensitivity. The severity of the condition is universally staged using the Taylor–Pelmear scale. Pre-operative planning in these cases rarely involves surgery but rather precise documentation for occupational health and Social Security Act qualifications.
| Stage | Condition of digits | Work and social interference |
|---|---|---|
| 0 | No blanching of digits | No complaints |
| 0T | Intermittent tingling | No interference with activities |
| 0N | Intermittent numbness | No interference with activities |
| 1 | Blanching of one or more fingertips, with or without tingling or numbness | No interference with activities |
| 2 | Blanching of one or more fingers, with numbness; usually confined to winter | Slight interference with home and social activities; no interference at work |
| 3 | Extensive blanching. Frequent episodes, summer and winter | Definite interference at work, at home, and with social activities. Restriction of hobbies |
| 4 | Extensive blanching. Most or all fingers affected. Frequent episodes, summer and winter | Occupation changed to avoid further exposure to vibration because of severity of signs and symptoms |
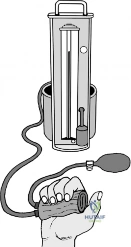
Patient positioning and operating room setup are critical for successful hand surgery. The patient is placed supine with the operative extremity extended onto a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless field, which is absolutely essential for identifying microscopic digital nerves and vessels. Exsanguination is achieved using an Esmarch bandage prior to tourniquet inflation, though this is contraindicated in the presence of purulent infections or malignant tumors to prevent systemic seeding. The surgeon must utilize loupe magnification (typically 2.5x to 4.5x) and specialized micro-instruments. Pre-operative templating for incisions—such as Brunner zig-zag incisions or multiple Z-plasties—is drawn with a sterile marker prior to skin incision to anticipate skin lengthening requirements over the extended joints.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a limited fasciectomy for Dupuytren’s contracture demands extreme precision. The skin is typically incised using a Brunner zig-zag approach to prevent longitudinal scar contracture, or via longitudinal incisions that are subsequently modified with Z-plasties. The skin flaps are elevated meticulously, leaving the subdermal vascular plexus intact. The pathological fascial cords are identified. The critical step is the identification and protection of the neurovascular bundles. Because the spiral cord displaces the nerve centrally and superficially, the surgeon must identify the nerve in the normal, un-diseased tissue proximally in the palm and trace it distally into the digit. Once the neurovascular bundles are safeguarded, the diseased fascia is sharply excised. If severe PIP joint contracture persists after fasciectomy, a sequential joint release is performed: first releasing the volar plate, followed by the accessory collateral ligaments, and rarely, the proper collateral ligaments.
Tendon repairs follow strict biomechanical principles. For an acute Zone II FDP laceration, the flexor sheath is exposed via a Brunner incision. The A2 and A4 pulleys are rigorously preserved to prevent bowstringing. The retracted tendon ends are retrieved, often requiring passage of a pediatric feeding tube or specialized tendon retriever. The primary repair is executed using a core suture of 3-0 or 4-0 non-absorbable braided material utilizing a multi-strand technique (e.g., 4-strand or 6-strand modified Kessler or cruciate repair) to provide sufficient tensile strength for early active motion. A continuous 6-0 epitendinous suture is then placed circumferentially to smooth the repair site and reduce gliding resistance. Extensor tendon lacerations on the dorsum of the hand (Zone VI) are more straightforward, repaired with a 4-0 non-absorbable core suture, and carry an excellent prognosis.

Tumor excision in the hand requires respect for surrounding anatomy. For a glomus tumor located beneath the nail, a transungual approach is utilized. The nail plate is carefully removed, and a longitudinal incision is made through the nail bed to expose the highly vascular, bluish tumor matrix. The tumor is enucleated entirely to prevent recurrence, and the nail bed is repaired with 6-0 absorbable sutures. For an enchondroma causing bony expansion or pathological fracture, a cortical window is created over the phalanx or metacarpal. The cartilaginous tumor is thoroughly curetted until healthy, bleeding bone is encountered. The resulting void is typically packed with autologous cancellous bone graft (often harvested from the distal radius) or allograft bone substitute.
Infections require aggressive, definitive drainage. For a paronychia, the cuticle is elevated, and if the infection tracks beneath the nail plate, the proximal third of the nail is excised to ensure complete drainage. A felon (pulp space infection) is drained via a mid-lateral incision, taking care to divide the fibrous septa spanning from the dermis to the periosteum to decompress the closed space fully, thereby preventing ischemic necrosis of the distal phalanx. Suppurative flexor tenosynovitis is managed with closed catheter irrigation. A proximal incision is made in the palm over the A1 pulley, and a distal incision is made over the A5 pulley. A pediatric catheter is introduced proximally, and the sheath is flushed with copious amounts of saline until the effluent is completely clear, followed by appropriate intravenous antibiotic therapy.
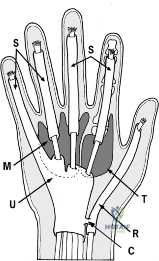
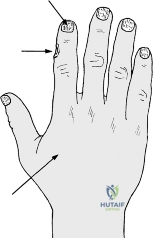
Fig. 7.A. Some potential sites of infection in the hand and fingers. S = synovial tendon sheaths; U = ulnar bursa; R = radial bursa; M = midpalmar space; T = thenar space. Note: C = communication between the radial and ulnar bursae.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications in hand surgery are frequent and can be devastating. In Dupuytren’s surgery, the most feared intraoperative complication is digital nerve laceration. The incidence of nerve injury is approximately 1% to 3% in primary surgeries but skyrockets to 5% to 10% in revision settings due to distorted anatomy and dense scar tissue. If a nerve is inadvertently divided, it must be repaired immediately under microscopic magnification using 8-0 or 9-0 nylon epineurial sutures. Post-operatively, hematoma formation is a significant risk that can lead to skin flap necrosis and deep infection. A unique complication of Dupuytren’s surgery is the "flare reaction"—an exaggerated, painful, edematous inflammatory response occurring in up to 10% of patients, characterized by profound stiffness and regional pain syndrome-like symptoms, requiring aggressive hand therapy and short courses of oral corticosteroids.
Tendon repairs are fraught with the dual risks of rupture and adhesion formation. Flexor tendon repairs in Zone II have a rupture rate of 4% to 9%, usually occurring between days 10 and 21 post-operatively when the tendon is at its weakest during the fibroblastic phase of healing. Conversely, overly conservative rehabilitation leads to dense peritendinous adhesions, resulting in a severe loss of active flexion. If adhesions restrict motion after 6 months of dedicated therapy, a surgical tenolysis may be indicated to free the tendon from the surrounding scar tissue. Extensor tendon repairs are less prone to rupture but frequently result in extensor lag or stiffness if splinted for excessive durations.
Salvage procedures are reserved for end-stage joint destruction, recalcitrant infections, or severe recurrent contractures. In the rheumatoid hand, advanced joint destruction with fixed deformities (such as severe ulnar drift at the MCP joints or swan neck deformities) often necessitates joint arthroplasty or arthrodesis. Silicone metacarpophalangeal joint replacements can provide excellent pain relief and functional alignment. For the DIP joint, whether destroyed by osteoarthritis, chronic mallet finger, or infection, arthrodesis in 0 to 5 degrees of flexion using headless compression screws or tension band wiring provides a stable, pain-free pinch grip.
| Complication | Incidence Rate | Prevention and Salvage Management |
|---|---|---|
| Digital Nerve Injury (Dupuytren's) | 1-3% (Primary); 5-10% (Revision) | Prevention: Trace nerve from proximal normal tissue. Salvage: Immediate microsurgical epineurial repair. |
| Zone II Flexor Tendon Rupture | 4-9% | ** |
Clinical & Radiographic Imaging Archive