Proximal Interphalangeal Joint Arthroplasty: Comprehensive Surgical Techniques
Key Takeaway
Proximal interphalangeal (PIP) joint arthroplasty is a critical surgical intervention for advanced arthritis or severe deformity. This guide details the Swanson dorsal approach and the alternative volar approach. Key steps include precise medullary canal preparation, meticulous soft tissue balancing for swan-neck and boutonniere deformities, and rigorous postoperative rehabilitation to restore digital kinematics and preserve functional range of motion.
Comprehensive Introduction and Patho-Epidemiology
Proximal interphalangeal (PIP) joint arthroplasty represents a highly sophisticated and technically demanding surgical intervention designed to alleviate debilitating pain, restore functional kinematics, and correct severe multi-planar deformities in digits compromised by advanced joint disease. The PIP joint is arguably the most critical articulation for the functional sweep of the digit, contributing to the vast majority of the arc of motion required for power grip, fine pinch, and overall hand dexterity. Pathologies necessitating such intervention typically include advanced primary osteoarthritis (OA), inflammatory arthropathies such as rheumatoid arthritis (RA) or psoriatic arthritis, and post-traumatic arthropathy resulting from intra-articular fractures or chronic ligamentous instability.
The epidemiological profile of PIP joint arthropathy varies significantly based on the underlying etiology. Primary osteoarthritis of the hand predominantly affects post-menopausal women, frequently presenting with Heberden’s and Bouchard’s nodes, the latter directly involving the PIP joints. In contrast, rheumatoid arthritis often presents with a more symmetric, polyarticular distribution, characterized by aggressive synovial pannus formation that systematically destroys the articular cartilage, attenuates the collateral ligaments, and destabilizes the delicate balance of the extensor mechanism. This inflammatory cascade frequently culminates in classic, complex digital deformities such as the swan-neck or boutonniere configurations, which severely limit hand function and present unique challenges during reconstructive efforts. Post-traumatic arthritis, conversely, tends to be unilateral and isolated to a single digit, often secondary to a remote history of a pilon fracture, fracture-dislocation, or unrecognized volar plate avulsion.
Unlike the distal interphalangeal (DIP) joint, where surgical arthrodesis is universally well-tolerated and often considered the procedure of choice, arthrodesis of the PIP joint significantly impairs the functional sweep of the digit. Fusing the PIP joint diminishes overall grip strength, restricts the hand's adaptive grip span, and severely impedes the ability to grasp large or irregularly shaped objects. Consequently, PIP joint arthroplasty remains the gold standard intervention for the ulnar digits (middle, ring, and small fingers) in order to preserve the hand's dynamic capabilities. The primary goal of the procedure is not necessarily to restore a normal, anatomical arc of motion, but rather to achieve a pain-free, stable joint with a functional arc of motion—typically ranging from 10 to 70 degrees of flexion—that allows for the performance of activities of daily living.
While PIP arthroplasty is highly successful in the ulnar digits, it is generally contraindicated in the index finger, particularly for patients who perform heavy manual labor or require strong key pinch. The index PIP joint is subjected to immense lateral shear forces and profound radial deviation moments during key pinch and tripod grasp activities. Silicone elastomer implants and even modern surface replacement arthroplasties are ill-equipped to withstand these repetitive, high-magnitude torsional and shear stresses, predictably leading to early implant failure, profound instability, or catastrophic particulate synovitis. In such cases, arthrodesis of the index PIP joint at approximately 35 to 40 degrees of flexion provides a far more stable, durable, and functionally reliable construct.
Detailed Surgical Anatomy and Biomechanics
The proximal interphalangeal joint is a classic ginglymus (hinge) joint, characterized by the articulation between the bicondylar head of the proximal phalanx and the biconcave base of the middle phalanx. The proximal phalangeal head features two distinct condyles separated by an intercondylar groove, which articulates congruently with the two shallow depressions on the middle phalangeal base, separated by a median ridge. This highly conforming osseous architecture inherently restricts motion primarily to the sagittal plane (flexion and extension), while severely limiting radioulnar deviation and axial rotation. The instantaneous center of rotation of the PIP joint remains relatively constant throughout the arc of motion, located centrally within the head of the proximal phalanx, which is a critical consideration when aligning prosthetic implants to prevent eccentric loading and premature wear.
Stability of the PIP joint is conferred by a robust and highly specialized soft-tissue envelope. The collateral ligament complex is the primary restraint to varus and valgus stress. It consists of the true (proper) collateral ligament (PCL), which originates from the lateral condylar recess of the proximal phalanx and inserts onto the volar-lateral aspect of the middle phalanx base, and the accessory collateral ligament (ACL), which inserts more volarly into the lateral margins of the volar plate. The PCL is maximally taut in flexion, whereas the ACL and volar plate are maximally taut in extension. The volar plate itself is a dense, fibrocartilaginous structure that prevents joint hyperextension. Proximally, it attaches to the proximal phalanx via two flexible check-rein ligaments, allowing it to glide during flexion, while its distal insertion on the middle phalanx is rigid and unyielding.
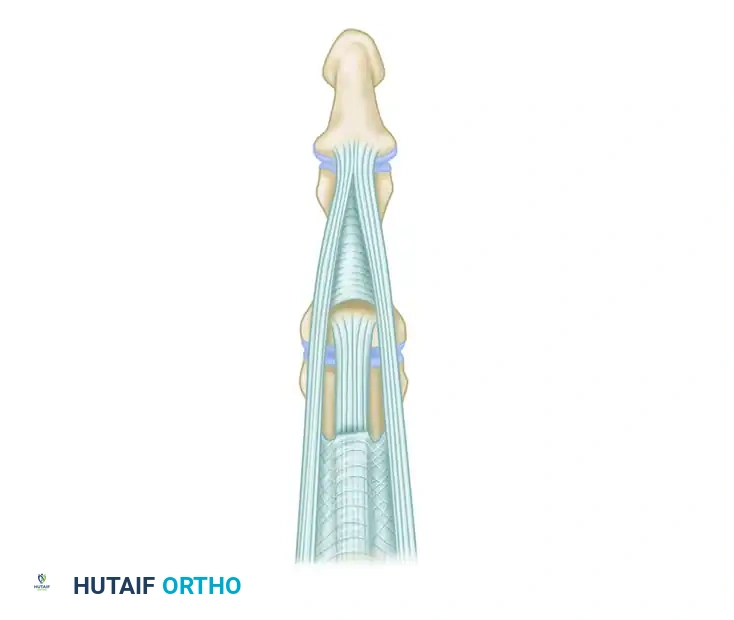
The extensor mechanism overlying the PIP joint is an intricate confluence of tendinous structures that must be meticulously managed during any dorsal surgical approach. The central slip of the extensor digitorum communis (EDC) inserts onto the dorsal base of the middle phalanx, providing the primary extensor force to the PIP joint. The lateral bands, formed by the convergence of the interosseous and lumbrical tendons, pass laterally to the PIP joint axis and converge distally to form the terminal tendon inserting on the distal phalanx. The delicate balance between the central slip and lateral bands is maintained by the triangular ligament dorsally (which prevents volar subluxation of the lateral bands) and the transverse retinacular ligament volarly (which prevents dorsal subluxation). Disruption of this precise anatomical balance by inflammatory pannus or trauma leads directly to boutonniere or swan-neck deformities.
From a biomechanical perspective, silicone elastomer implants (such as the classic Swanson design or modern pre-flexed variants) do not function as true articulating prostheses. Instead, they act as dynamic, flexible spacers that maintain joint alignment while relying on the phenomenon of "encapsulation." Postoperatively, a fibrous pseudocapsule forms around the silicone implant. The implant's flexible hinge absorbs shock and maintains the joint space, while the newly formed pseudocapsule provides the actual long-term stability. Precise surgical technique is paramount; the implant stems must be perfectly sized to prevent cortical abutment or "pistoning" within the medullary canal, which can lead to premature mechanical failure, silicone wear debris generation, particulate synovitis, and subsequent periprosthetic osteolysis.
Exhaustive Indications and Contraindications
Patient selection is the most critical determinant of success in proximal interphalangeal joint arthroplasty. The decision to proceed with arthroplasty versus arthrodesis must be individualized, taking into account the patient's age, occupation, functional demands, underlying pathology, and the specific digit involved. A thorough understanding of the indications and absolute contraindications is mandatory to prevent catastrophic surgical failures and ensure optimal functional outcomes.
The primary indication for PIP joint arthroplasty is debilitating, refractory pain associated with advanced articular cartilage destruction that has failed comprehensive conservative management (e.g., NSAIDs, splinting, intra-articular corticosteroid injections). Secondary indications include the restoration of a functional arc of motion in a severely stiffened joint and the correction of complex digital deformities (swan-neck or boutonniere) in patients with rheumatoid arthritis. The ideal candidate is a low-demand, older patient with primary osteoarthritis or inflammatory arthritis involving the ulnar digits, who requires a functional arc of motion for activities of daily living but does not subject their hands to heavy manual labor or repetitive high-impact loading.
Contraindications must be rigorously respected. Active or recent localized infection is an absolute contraindication to any joint replacement. Insufficient bone stock, often seen in end-stage rheumatoid arthritis with severe osteopenia or massive cystic changes, precludes the stable seating of implant stems and drastically increases the risk of intraoperative periprosthetic fracture. Furthermore, a non-functioning extensor mechanism or irreversible flexor tendon rupture that cannot be reconstructed concurrently renders the arthroplasty useless, as the implant relies entirely on the dynamic balance of the surrounding musculotendinous units for active motion.
| Category | Proximal Interphalangeal Joint Arthroplasty Considerations |
|---|---|
| Primary Indications | - Debilitating, refractory pain secondary to OA, RA, or post-traumatic arthritis. - Severe restriction of motion impairing activities of daily living. - Complex multi-planar deformities (Swan-neck, Boutonniere) in RA. - Involvement of the ulnar digits (middle, ring, small fingers). |
| Relative Contraindications | - Young, high-demand patients (heavy laborers, athletes). - Index finger involvement (due to lateral shear forces during key pinch). - Poor patient compliance anticipated for rigorous post-operative therapy. - Moderate bone loss requiring extensive grafting. |
| Absolute Contraindications | - Active or recent localized or systemic infection. - Absent or irreparably damaged flexor/extensor motor function. - Severe, uncorrectable neurovascular compromise to the digit. - Inadequate bone stock precluding stable implant stem fixation. - Known severe allergy to silicone or implant materials. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative clinical and radiographic evaluation forms the foundation of a successful PIP joint arthroplasty. The clinical examination must meticulously assess the active and passive range of motion, the presence of fixed contractures, and the integrity of the collateral ligaments. The surgeon must evaluate the extensor mechanism for central slip attenuation (suggestive of a boutonniere deformity) or volar plate laxity (suggestive of a swan-neck deformity). Furthermore, a comprehensive neurovascular assessment is required, documenting two-point discrimination and capillary refill, particularly in patients with severe deformities where neurovascular bundles may be contracted or displaced.
Radiographic evaluation requires high-quality, standardized posteroanterior (PA), true lateral, and oblique views of the affected digit, rather than just the entire hand. These precise views are critical to assess the remaining joint space, the extent of subchondral sclerosis, the presence of osteophytes, and the overall alignment of the phalanges. Digital templating is highly recommended to estimate the required implant size, evaluate the medullary canal width of both the proximal and middle phalanges, and identify any significant cystic changes or angular deformities that might require bone grafting or corrective osteotomies during the canal preparation phase. In patients with severe rheumatoid arthritis, a dual-energy X-ray absorptiometry (DEXA) scan may be considered to formally assess bone mineral density, as profound osteopenia significantly alters the tactile feedback during broaching and increases fracture risk.
Patient positioning and anesthesia are optimized to provide a bloodless, motionless surgical field. The procedure is typically performed on an outpatient basis. Regional anesthesia, specifically a supraclavicular or axillary brachial plexus block, is the modality of choice. This not only provides excellent intraoperative surgical anesthesia but also ensures prolonged postoperative analgesia, facilitating early mobilization and reducing the need for systemic opioids. General anesthesia is reserved for patients with contraindications to regional blocks or those undergoing extensive, multi-digit reconstructions.
The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic upper arm tourniquet is applied. The limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to typically 250 mmHg or 100 mmHg above the patient's systolic blood pressure. Prophylactic intravenous antibiotics (typically a first-generation cephalosporin, or clindamycin for penicillin-allergic patients) are administered at least 30 minutes prior to tourniquet inflation to ensure adequate tissue penetration. The hand is prepped and draped in a standard sterile fashion, ensuring the entire hand and wrist are exposed to allow for intraoperative assessment of digital cascade and alignment.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the PIP joint dictates the management of the soft tissue envelope and profoundly influences the postoperative rehabilitation protocol. The two primary approaches are the dorsal approach (traditional Swanson technique) and the anterior (volar) approach. The choice of approach depends on the underlying pathology, the presence of concurrent deformities, and the surgeon's preference.
The Dorsal Approach (Swanson Technique)
The dorsal approach is the most widely utilized technique, particularly favored for patients with rheumatoid arthritis who require concurrent extensor mechanism reconstruction or correction of complex digital deformities.
Make a dorsal, longitudinal, slightly curved (or lazy-S) incision centered over the PIP joint. This geometry mitigates the risk of dorsal scar contracture, which can limit postoperative flexion. Carefully dissect through the subcutaneous tissues, taking care to preserve the thin, delicate dorsal sensory nerve branches and the dorsal venous plexus to minimize postoperative edema. Expose the extensor mechanism fully from the mid-proximal phalanx to the distal interphalangeal joint.
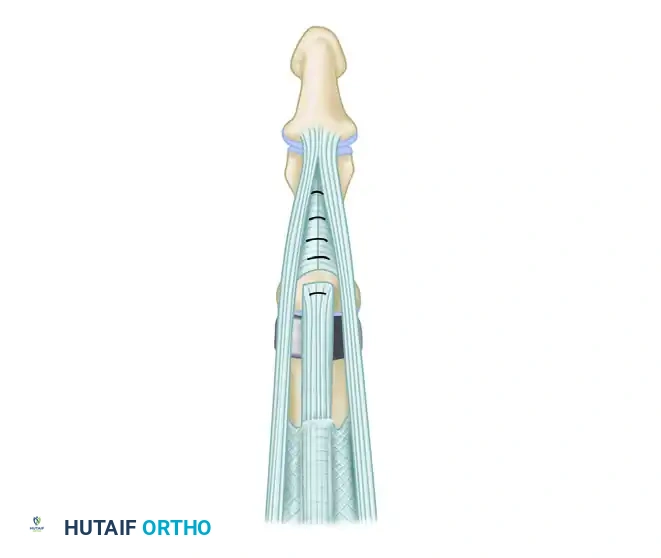
Incise the central tendon longitudinally, precisely in the midline (a tendon-splitting approach). Alternatively, a Chamay approach (creating a distally based triangular flap of the central slip) can be utilized. It is critical to preserve the distal insertion of the central slip at the dorsal base of the middle phalanx. Gently retract the split central tendon radially and ulnarly to expose the underlying joint capsule. Maintain the collateral ligament insertions on the middle phalanx as much as possible to preserve coronal plane stability.
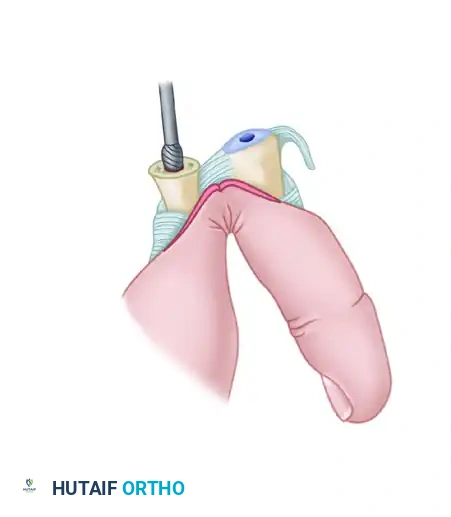
Expose the head of the proximal phalanx. Using an oscillating microsaw, resect the proximal phalanx head just proximal to the collateral ligament origins at the metaphyseal flare. The resection must be perfectly perpendicular to the long axis of the phalanx in both the coronal and sagittal planes. Inadequate resection will result in a tight joint space, leading to restricted flexion, excessive compressive forces on the implant hinge, and early mechanical failure.
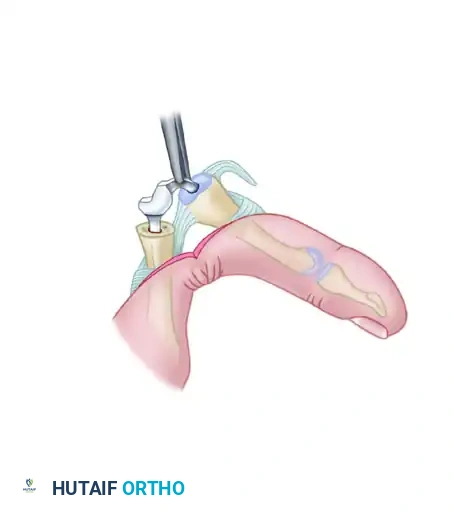
Accurately determine the central axis of the proximal phalanx medullary canal using a sharp awl. Fluoroscopy is highly recommended during this step to prevent inadvertent cortical perforation, especially in osteopenic bone. Ream and broach the medullary canal using proprietary rasps. The goal is to accommodate the largest possible implant stem without compromising the cortical integrity; a "press-fit" is not desired for silicone implants, as slight pistoning is required for the dynamic spacer concept. Next, address the middle phalanx. Enter the base of the middle phalanx with the awl. The articular surface of the middle phalanx is usually not resected to preserve the strong subchondral bone platform, unless severe bony distortion requires recontouring.
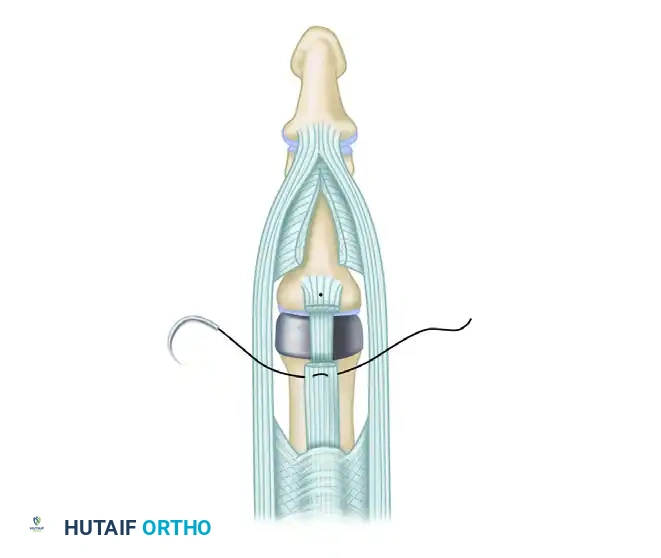
Insert a properly sized prosthetic implant trial. Fold the implant and place both stems into their respective canals simultaneously while the PIP joint is flexed. Assess the kinematics: the stems must be fully seated, the waist of the implant must not be compressed in full extension, and the cortices must not abut in full flexion. Once optimal sizing is confirmed, irrigate the canals copiously. Insert the permanent silicone implant using a strict no-touch technique to minimize contamination and lipid absorption onto the silicone surface. Repair the central tendon meticulously with non-absorbable or slowly absorbable horizontal mattress sutures.
Management of Concurrent Digital Deformities
Rheumatoid arthritis frequently presents with complex digital deformities that must be addressed concurrently with the arthroplasty. Failure to rebalance the soft tissues will inevitably lead to recurrent deformity and implant failure.
Swan-Neck Deformity Correction:
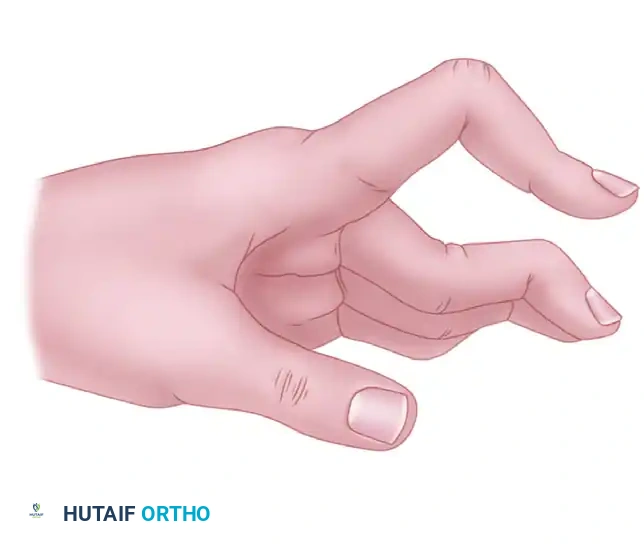
A swan-neck deformity is characterized by PIP joint hyperextension and DIP joint flexion, driven by volar plate laxity and dorsal subluxation of the lateral bands.
To correct this during the dorsal approach, the central tendon must be separated from the lateral tendons by dividing the connecting fibers. The central tendon is then step-cut transversely and dissected proximally, effectively lengthening it to reduce the hyperextension force.

Release the triangular ligament to allow the lateral bands to mobilize. The lateral tendons are then relocated palmarward (volarly) to restore their normal mechanical axis below the center of rotation of the PIP joint. After the implant is inserted, the cut ends of the lengthened central tendon are approximated with interrupted sutures, ensuring the knots are buried.
Boutonniere (Buttonhole) Deformity Correction:
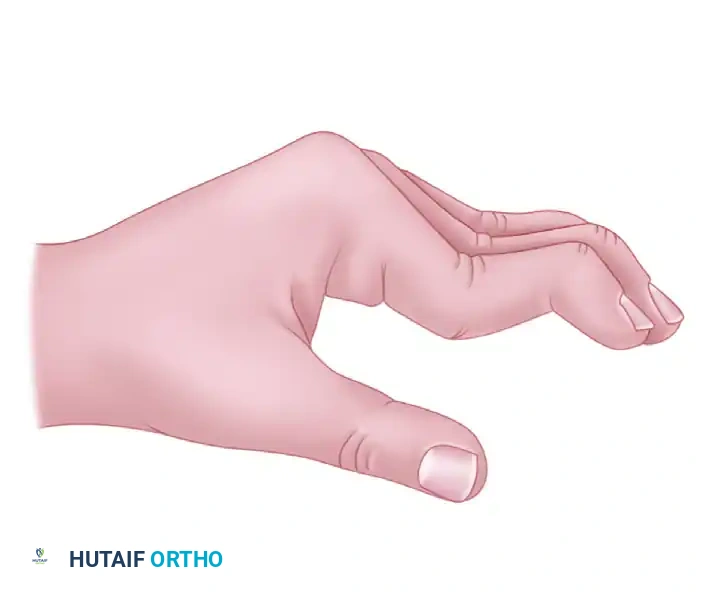
A boutonniere deformity presents with PIP joint flexion and DIP joint hyperextension, resulting from attenuation or rupture of the central slip and subsequent volar subluxation of the lateral bands.
Correction requires meticulous rebalancing. The triangular ligament must be released and imbricated to permit the lateral bands to shift dorsally, restoring PIP joint extension.
The attenuated central tendon is advanced distally and reinserted securely into the dorsum of the middle phalanx. Collateral ligaments may also require release or partial excision to permit satisfactory joint alignment, especially in joints severely distorted by chronic arthritic contractures.
The Anterior (Volar) Approach
The anterior (volar) approach is an excellent alternative for patients with primary osteoarthritis or post-traumatic arthritis without significant extensor mechanism compromise. This approach preserves the dorsal venous drainage and leaves the extensor apparatus entirely pristine, allowing for immediate, aggressive postoperative mobilization.
Make a V-shaped or Brunner zigzag incision over the volar aspect of the PIP joint. Elevate the skin flaps, taking extreme care to identify and protect the neurovascular bundles bilaterally throughout the procedure.
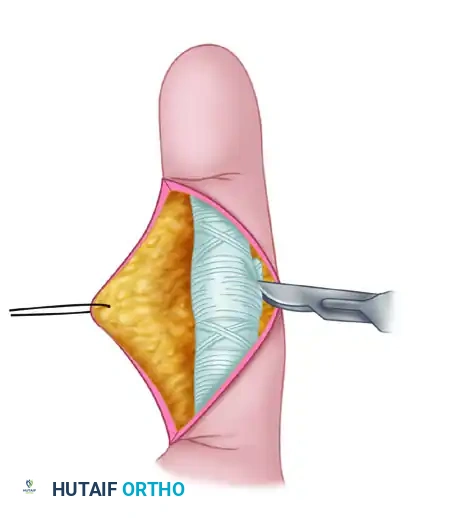
Expose the flexor tendon sheath. Divide the A3 pulley to allow mobilization of the flexor tendons.
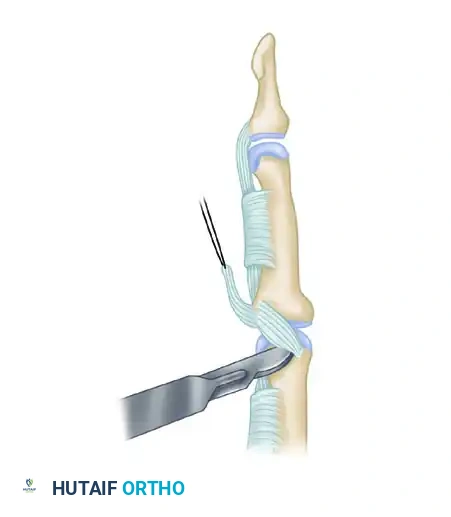
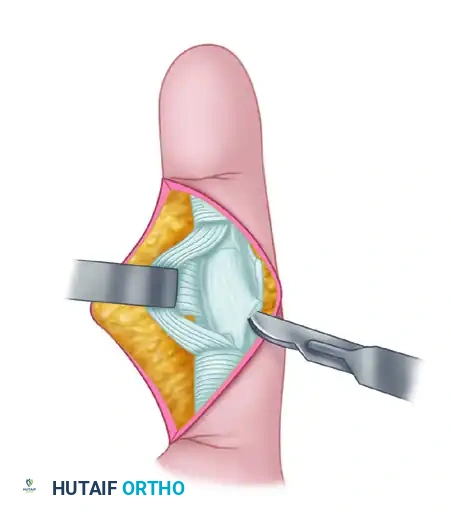
Retract the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons laterally using a blunt retractor to expose the underlying volar plate. Detach the volar plate proximally from its origin on the proximal phalanx (releasing the check-rein ligaments), leaving its distal insertion on the middle phalanx intact.
Identify the collateral ligaments. To achieve adequate exposure, the collateral ligament origins on the proximal phalanx must be completely released from their bony attachments.
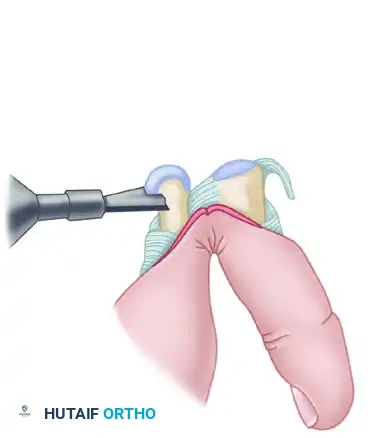
Once the collaterals and volar plate are released, hyperextend the PIP joint (the "shotgun" maneuver) to fully expose the articular surfaces of both the proximal and middle phalanges. This provides unparalleled visualization of the joint surfaces.
Using an oscillating microsaw, remove the head of the proximal phalanx at the metaphyseal flare. Prepare the medullary canals of the proximal and middle phalanges using properly sized power burrs and broaches. Ensure the central axis is maintained to prevent angular deformity.
Insert provisional trial implants to assess sizing. Perform a trial of active and passive motion to ensure there is no impingement, cortical abutment, or instability.
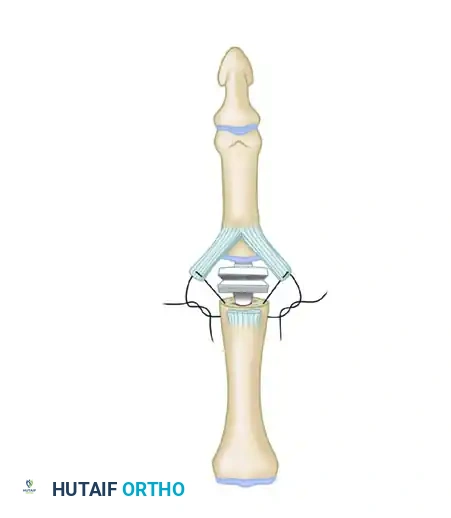
Once satisfied with the kinematics, insert the permanent silicone implant. A critical step in the volar approach is the reconstruction of the collateral ligaments to restore coronal stability. The proximally detached volar plate can be split longitudinally. The two halves are then sutured to the lateral aspects of the proximal phalanx using suture anchors or transosseous tunnels to reconstruct the collateral ligaments and prevent postoperative hyperextension.
Repair the A3 pulley if possible, or ensure the A2 and A4 pulleys are completely intact to prevent flexor tendon bowstringing. Close the skin meticulously with interrupted non-absorbable sutures.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and rigorous postoperative rehabilitation, complications following PIP joint arthroplasty are not uncommon. The surgeon must be prepared to identify and manage these complications promptly to salvage digital function. Complications can be broadly categorized into biological (infection, synovitis), mechanical (implant fracture, subsidence), and functional (stiffness, recurrent deformity).
Infection is a devastating complication, occurring in approximately 1% to 3% of cases. Superficial infections can often be managed with oral antibiotics and local wound care. However, deep periprosthetic infections require aggressive surgical intervention. The standard of care involves immediate operative irrigation and debridement, complete removal of the silicone implant, and placement of an antibiotic-impregnated cement spacer. Once the infection is definitively eradicated (confirmed by normal inflammatory markers and negative cultures), the surgeon may attempt revision arthroplasty or, more commonly, conversion to a definitive arthrodesis.
Implant fracture and mechanical failure are among the most frequently cited long-term complications, with radiographic fracture rates reported as high as 10% to 30% at ten years for silicone implants. Interestingly, radiographic fracture does not always correlate with clinical failure. Because the silicone implant acts as a dynamic spacer, the fibrous pseudocapsule often maintains joint stability and alignment even if the hinge is fractured. If the patient remains asymptomatic, observation is the appropriate course of action. However, symptomatic failure, characterized by pain, gross instability, or progressive deformity, requires revision. Particulate synovitis (silicone lymphadenopathy) is a severe inflammatory reaction to silicone wear debris, leading to aggressive periprosthetic osteolysis. This requires implant removal, thorough synovectomy, bone grafting of cystic lesions, and conversion to arthrodesis.
Stiffness remains the most common functional complication, particularly following the dorsal approach where scarring of the extensor mechanism restricts flexion. Aggressive hand therapy is the first line of management. If conservative measures fail and the patient has a functional deficit, surgical tenolysis or capsulotomy may be considered, though results are often unpredictable. Recurrent deformity is typically the result of inadequate soft tissue balancing during the index operation or patient non-compliance with postoperative splinting protocols.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Stiffness / Loss of ROM | 15% - 25% | Extensor mechanism scarring, inadequate resection, poor therapy compliance. | Aggressive hand therapy, dynamic splinting. Surgical tenolysis (rarely successful). |
| Radiographic Implant Fracture | 10% - 30% (at 10 yrs) | Shear forces, eccentric loading, improper sizing, index finger placement. | Asymptomatic: Observe. Symptomatic: Revision arthroplasty or Arthrodesis. |
| Recurrent Deformity | 5% - 15% | Failure to correct swan-neck/boutonniere, collateral ligament insufficiency. | Soft-tissue revision/rebalancing. Conversion to Arthrodesis if uncorrectable. |
| Particulate Synovitis | 2% - 5% | Silicone wear debris generation, micro-motion of stems. | Implant removal, synovectomy, bone grafting, definitive Arthrodesis. |
| Deep Periprosthetic Infection | 1% - 3% | Contamination, poor soft tissue envelope, systemic immunosuppression (RA). | I&D, implant removal, antibiotic spacer. Delayed Arthrodesis. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional success of a proximal interphalangeal joint arthroplasty is inextricably linked to a rigorous, specialized, and closely monitored hand therapy protocol. The rehabilitation strategy must be carefully tailored to the specific surgical approach utilized and the nature of any concurrent soft-tissue reconstructions. Communication between the operating surgeon and the certified hand therapist is paramount.
For the Dorsal Approach (Uncomplicated):
Because the central slip of the extensor mechanism is violated and repaired during the dorsal approach, the primary goal in the early postoperative phase is to protect this repair while preventing flexor tendon adhesions.
- Days 1-5: The hand is immobilized in a bulky compressive dressing with the PIP joint in full extension (0 degrees) to eliminate tension on the central slip repair. The MCP joints are left free to allow early motion.
- Weeks 1-4: A custom static or dynamic extension splint is fabricated. Active flexion is permitted within the constraints of the splint (usually limited to 30-40 degrees initially), but passive flexion is strictly avoided to prevent central slip rupture or attenuation. The patient performs active extension exercises to maintain extensor tone.
- Weeks 4-6: The splinting is gradually weaned during the day. Active and gentle passive range of motion exercises are advanced. The goal is to achieve 70 degrees of flexion by week 6.
- Weeks 6+: Progressive strengthening exercises commence. Dynamic flexion splinting may be introduced if stiffness persists.
For Deformity Corrections (Rheumatoid Arthritis):
Rehabilitation following deformity correction is highly restrictive and prioritizes the healing of the rebalanced soft tissues over the rapid acquisition of motion.
- Swan-Neck Correction: The PIP joint is splinted in 10 to
