Comprehensive Management of Painful Amputation Stumps and Hand Reconstruction

Key Takeaway
The management of painful amputation stumps and subsequent hand reconstruction requires a meticulous, evidence-based approach. Pain is frequently driven by terminal neuromas, inadequate soft-tissue coverage, or bony prominences. Reconstructive options range from local advancement flaps and neuroma excision to complex procedures like the Krukenberg operation and thumb pollicization. This guide provides a comprehensive overview of surgical indications, biomechanics, step-by-step operative techniques, and postoperative protocols to optimize functional outcomes in upper extremity amputees.
Comprehensive Introduction and Patho-Epidemiology
Revision surgery is a frequent, highly specialized, and technically demanding elective procedure for the management of painful amputation stumps and the functional restoration of the severely mutilated hand. These procedures are particularly critical following high-energy traumatic injuries, such as industrial crush injuries, blast traumas, and severe avulsions, which inherently involve extensive zones of injury, devascularization, and gross contamination. The etiology of stump pain is notoriously multifactorial, presenting a complex clinical challenge that requires the operating surgeon to differentiate between neurogenic pain, somatic pain from inadequate soft-tissue envelopes, and centrally mediated phantom limb pain. Among these etiologies, a terminal neuroma located in an unpadded, mechanically vulnerable area near the distal end of the stump remains the most common and surgically correctable culprit.

Following peripheral nerve transection, a well-documented cascade of neurobiological events ensues. Wallerian degeneration occurs distally, clearing the axonal debris, while the proximal stump mounts a vigorous attempt at regeneration. The proximal axonal growth cones sprout numerous unmyelinated neurites. However, without an intact distal endoneurial tube to guide their trajectory toward target end-organs, these regenerating axons, alongside proliferating Schwann cells and fibroblasts, form a disorganized, bulbous, and highly sensitive mass—the neuroma. When this neuromatous mass is tethered to adjacent unyielding scar tissue, embedded in bone, or positioned directly beneath thin, non-glabrous skin, normal tactile pressure or even mild ambient temperature changes translate into severe, debilitating neuropathic pain.

The epidemiology of painful amputation stumps indicates a significant burden of morbidity, particularly in the working-age population who sustain occupational injuries. Studies suggest that symptomatic neuromas develop in up to 30% of major upper extremity amputations and a significant proportion of digital amputations. The chronification of this pain can lead to severe functional impairment, psychological distress, and the eventual abandonment of prosthetic devices. Furthermore, pain in an amputation stump is not exclusively neurogenic. It can frequently be caused by prominent bony exostoses covered only by thin, non-glabrous skin (such as a split-thickness skin graft) or by skin rendered tight, tethered, and ischemic by underlying cicatrix formation. Understanding this patho-epidemiology is the foundational step in planning a reconstructive intervention that addresses both the neural generators of pain and the biomechanical deficiencies of the residual limb.

Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy and biomechanics of the upper extremity is paramount when undertaking revision amputation and hand reconstruction. The peripheral nerves of the upper extremity possess a complex microanatomy consisting of the epineurium, perineurium, and endoneurium. The perineurium, which encases individual fascicles, acts as a critical blood-nerve barrier. In the context of neuroma formation, the disruption of this barrier leads to localized edema, ectopic impulse generation, and mechanosensitivity. When performing neuroma excision and proximal relocation, the surgeon must mobilize the nerve sufficiently to allow it to retract into a deep, well-vascularized muscle belly, completely free from the sheer forces of the superficial fascial layers and the prosthetic socket interface.
In instances where pain is driven by inadequate soft-tissue coverage over a bony prominence, the vascular anatomy of the integumentary flaps becomes the focal point. For digital tip amputations, the Moberg advancement flap relies on the robust arborization of the volar digital arteries. These vessels, along with the volar digital nerves, must be meticulously preserved during the elevation of the flap. Biomechanically, the volar skin of the digits is uniquely designed for prehension, characterized by fibrous septa that tether the dermis to the underlying periosteum, preventing shear during pinch. When reconstructing the digital tip, restoring this stable, sensate, and shear-resistant pad is essential. However, the proximal dissection of the Moberg flap in fingers is strictly limited by the vascular supply; extending proximal to the proximal interphalangeal (PIP) joint severely compromises perfusion and invariably leads to devastating flexion contractures.

The biomechanics of the thumb are the cornerstone of hand function, providing the essential counter-post for all modes of prehension. A successfully reconstructed thumb must meet five non-negotiable biomechanical pillars: protective and tactile sensibility, skeletal stability to withstand pinch pressure without joint collapse, sufficient basal joint (CMC) mobility for opposition, adequate length to meet the opposing digits, and acceptable cosmesis. When evaluating a patient for the Krukenberg operation following a distal forearm amputation, the biomechanical paradigm shifts entirely. This procedure converts the forearm into a sensate pincer by separating the radius and ulna into two independent rays. The pronator teres becomes the primary motor for the radial ray, providing the adduction force necessary for grasp. The preservation of tactile sensibility and proprioception in the Krukenberg pincer provides a profound biomechanical advantage over standard prostheses, allowing for closed-loop sensory feedback during object manipulation.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for a painful amputation stump or complex hand reconstruction requires a meticulous risk-benefit analysis, balancing the patient's functional demands with the anatomical realities of the residual limb. Surgical excision of a neuroma is strictly indicated when conservative measures—including aggressive padding, prosthetic modifications, desensitization therapies, and pharmacological management (e.g., gabapentinoids, tricyclic antidepressants)—have failed to provide definitive relief, and when diagnostic local anesthetic blocks yield a transient but complete cessation of the localized pain.

For soft tissue contouring, the Moberg advancement flap is highly indicated for thumb tip amputations with exposed bone or painful, thin scar tissue, provided the defect is no larger than 1.5 cm. In the context of major hand amputations, the Krukenberg operation is exceptionally valuable for bilateral upper extremity amputees, particularly those who have concomitant visual impairments. For these patients, the preservation of tactile sensibility allows them to interact with their environment using direct sensory feedback, a capability impossible with standard myoelectric or body-powered prostheses. Conversely, thumb reconstruction via metacarpal lengthening (Gillies-Millard) is indicated when amputation occurs at the metacarpophalangeal joint or within the condylar area of the first metacarpal, provided the intrinsic thenar musculature remains intact and functional.
Contraindications to these procedures are equally critical to recognize. Active infection, severe peripheral vascular disease, and profound psychiatric instability or unrealistic patient expectations serve as absolute contraindications to elective stump revision. The Moberg flap is strictly contraindicated for large defects in the triphalangeal digits due to the high risk of PIP joint flexion contractures and dorsal skin necrosis. The Krukenberg procedure is contraindicated if there is insufficient proximal musculature (specifically a compromised pronator teres) or severe scarring that would preclude the independent motion of the radial and ulnar rays.
| Surgical Procedure | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Neuroma Excision & Relocation | Refractory localized neuropathic pain; positive Tinel's sign; positive response to diagnostic block. | Active local infection; pain entirely central (Phantom Limb Pain) without local somatic generator. | Severe CRPS; active systemic coagulopathy; unrealistic expectations. |
| Moberg Advancement Flap | Volar thumb tip defects < 1.5 cm with exposed bone; painful thin scar at thumb pulp. | Volar defects in triphalangeal digits requiring dissection proximal to PIP joint; compromised digital arteries. | Heavy tobacco use; significant prior volar scarring. |
| Krukenberg Operation | Bilateral distal forearm amputations; blind patients requiring sensate prehension. | Insufficient proximal motor function (damaged pronator teres); severe proximal radioulnar joint stiffness. | Unilateral amputation in a patient prioritizing cosmesis over sensate prehension. |
| Gillies-Millard Thumb Recon | Thumb amputation at MCP joint or proximal phalanx; intact thenar musculature. | Complete absence of the first metacarpal base and CMC joint; severe local vascular compromise. | Stiff, non-functional opposing digits; advanced age with low functional demands. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the linchpin of successful revision amputation surgery. The clinical evaluation must begin with precise mapping of the pain generators. A well-localized area of extreme tenderness associated with a palpable small mass, usually in line with a native digital or major peripheral nerve, is pathognomonic for a symptomatic neuroma. A positive Tinel's sign at the stump apex, which may radiate proximally along the nerve distribution, further confirms the diagnosis. The surgeon must utilize diagnostic local anesthetic blocks (e.g., 1% lidocaine or 0.5% bupivacaine injected precisely at the site of the suspected neuroma) to definitively differentiate neuroma-mediated pain from centrally mediated phantom limb pain or proximal nerve compression syndromes.
Radiographic imaging is mandatory to evaluate the skeletal architecture of the stump. High-quality orthogonal radiographs will reveal bony prominences, heterotopic ossification, osteophytes, or inadequate bone resection that may be tenting the skin and causing somatic pain. In complex cases, high-resolution ultrasound or magnetic resonance neurography (MRN) can be employed to visualize the exact size and location of neuromas, particularly those embedded within dense scar tissue. For reconstructive procedures such as the Gillies-Millard metacarpal lengthening, pre-operative templating is essential. The surgeon must calculate the exact length of the required iliac crest bone graft and plan the geometry of the local advancement flaps to ensure tension-free closure over the reconstructed skeletal ray.

Patient positioning and operating room setup must be optimized for microsurgical precision. The patient is typically positioned supine with the affected extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is absolutely critical for the meticulous dissection of scarred neurovascular structures. The surgeon should operate under loupe magnification (minimum 3.5x) or utilize an operating microscope for nerve handling and microvascular repairs. Prophylactic intravenous antibiotics are administered prior to tourniquet inflation. For procedures requiring bone grafting, such as thumb lengthening, the ipsilateral iliac crest is simultaneously prepped and draped to facilitate efficient graft harvest.
Step-by-Step Surgical Approach and Fixation Technique
Management of the Neuroma and Soft Tissue Contouring
When surgical intervention is indicated for a painful neuroma, the procedure begins with a careful incision through healthy tissue, avoiding the previous scar if possible. The neuroma must be meticulously dissected free from the surrounding scar bed, taking extreme care not to inadvertently injure adjacent intact neurovascular structures. Once isolated, the nerve is placed under gentle traction. It is then sharply divided with a microsurgical blade at a more proximal level, where the fascicular architecture appears healthy and unscarred. The newly transected end is allowed to retract into a healthy, well-padded soft-tissue bed. Modern techniques such as Targeted Muscle Reinnervation (TMR) or Regenerative Peripheral Nerve Interfaces (RPNI) may be employed at this stage, suturing the proximal nerve stump to a local motor nerve or wrapping it in a free muscle graft, respectively, to provide a physiological target for regenerating axons and prevent recurrent neuroma formation.
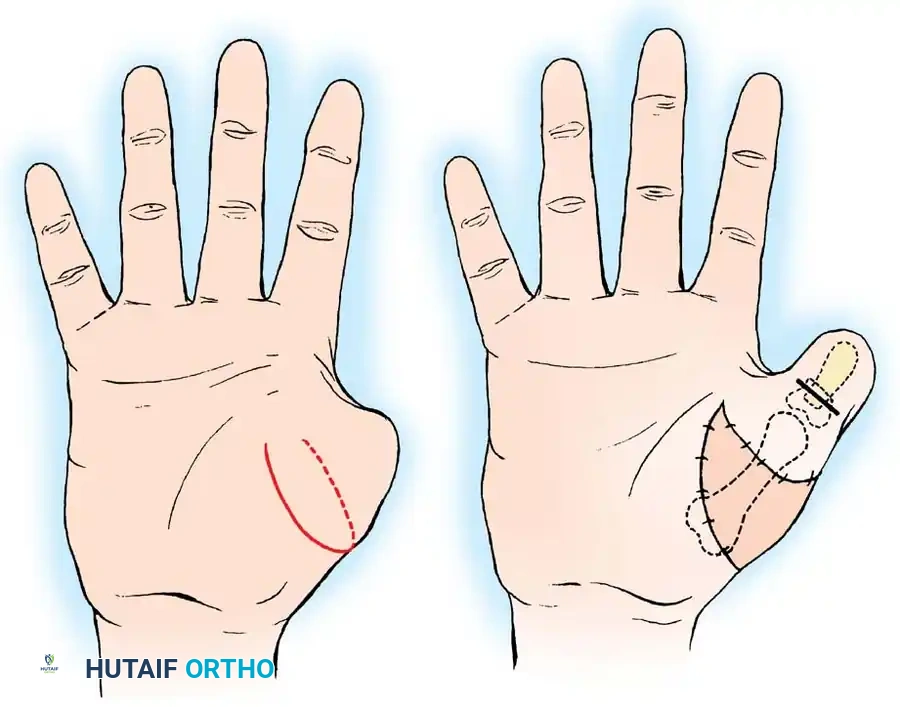
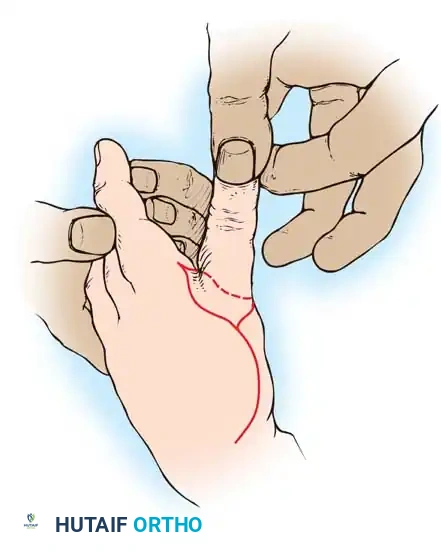
The Moberg Advancement Flap Technique
For painful thumb stumps requiring soft tissue contouring, the Moberg flap is executed with precision. The flap is outlined over the volar aspect of the digit, incorporating both neurovascular bundles to ensure robust perfusion and preserved sensibility. Mid-lateral incisions are made just dorsal to the neurovascular bundles. The flap is elevated deep to these bundles, carefully separating them from the underlying flexor tendon sheath. The flap is then advanced distally (typically up to 1.5 cm) to cover the terminal defect. If advancement is restricted, the interphalangeal joint may be slightly flexed, or a proximal V-Y release can be incorporated. The flap is secured with interrupted non-absorbable sutures, ensuring no tension on the distal tip.

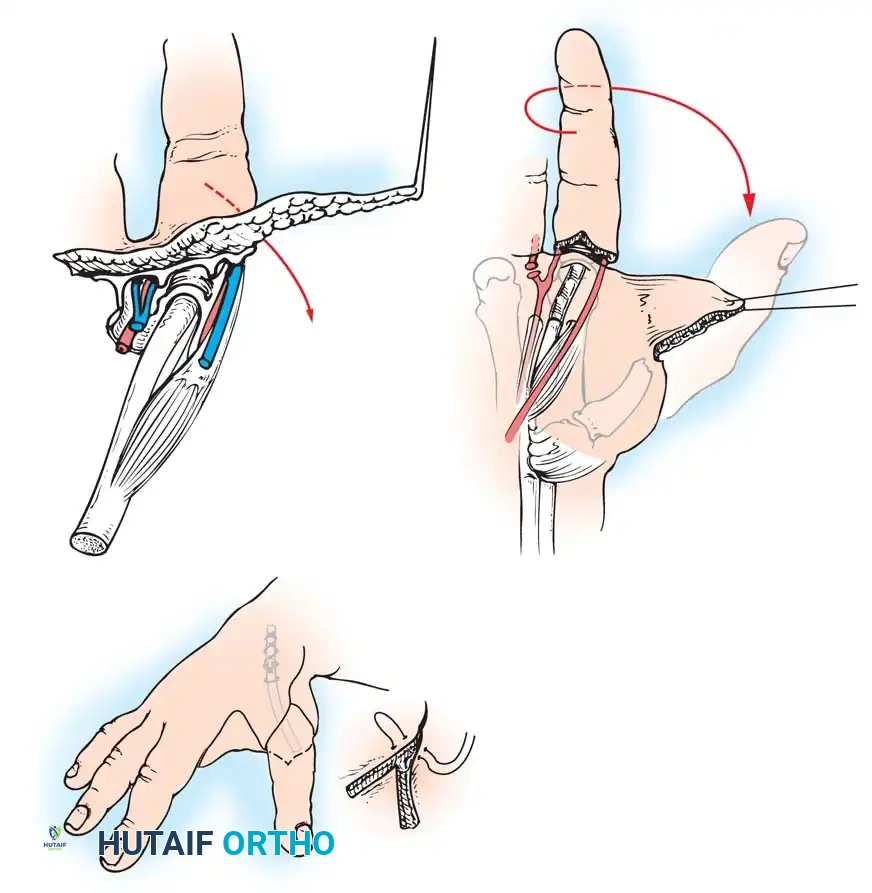
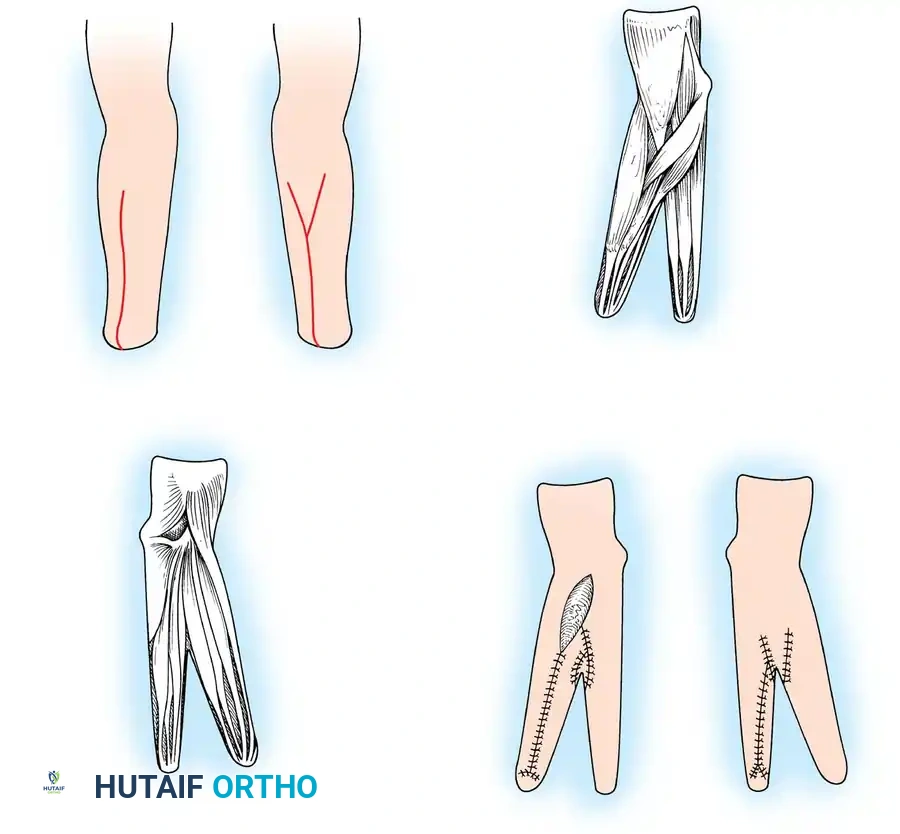
The Krukenberg Procedure
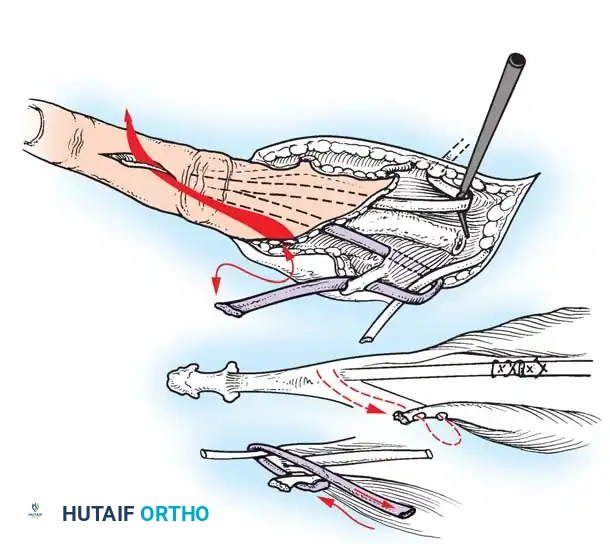
The Krukenberg operation represents a masterclass in anatomical reorganization. A longitudinal incision is made on the flexor surface of the forearm, biased slightly toward the radial side, with a corresponding dorsal incision biased toward the ulnar side. A V-shaped flap is elevated dorsally to form the new web space. The forearm musculature is systematically separated into two distinct functional groups: the radial ray (adductors/abductors including the pronator teres, brachioradialis, radial wrist flexors/extensors, and radial halves of FDS/EDC) and the ulnar ray (ulnar wrist flexors/extensors and ulnar halves of FDS/EDC). Debulking of deep muscles (pronator quadratus, FDP, FPL) is performed to allow tension-free closure, taking absolute care not to disturb the pronator teres. The interosseous membrane is incised longitudinally along its ulnar attachment, preserving the anterior interosseous neurovascular bundle. The rays are separated to achieve 6 to 12 cm of clearance at their tips. Skin is rotated and closed so suture lines do not lie on the opposing tactile surfaces, and split-thickness grafts are applied to residual defects.

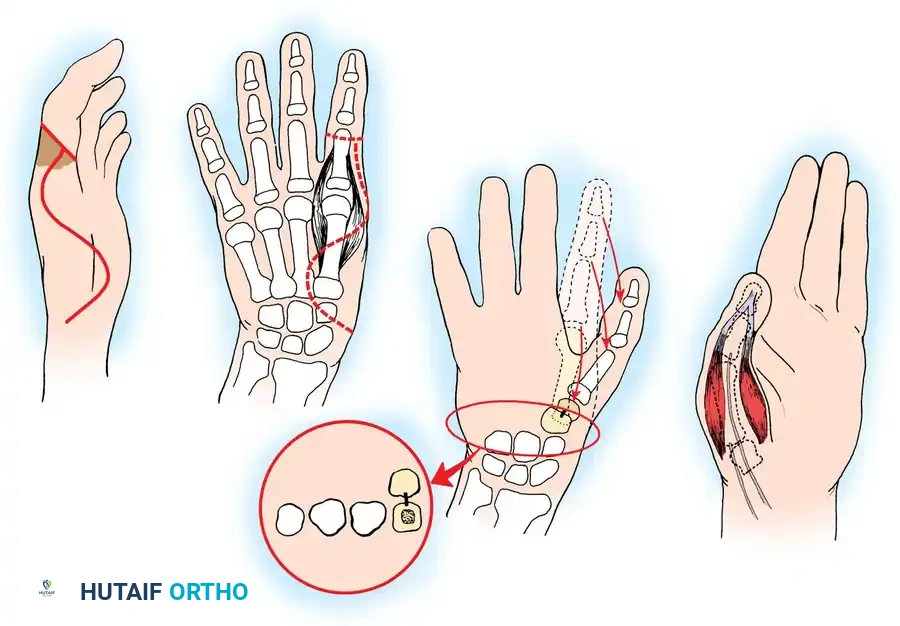
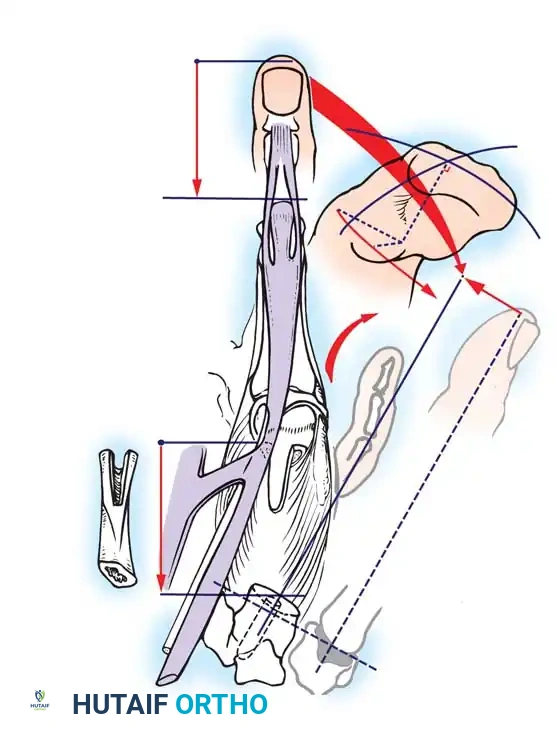
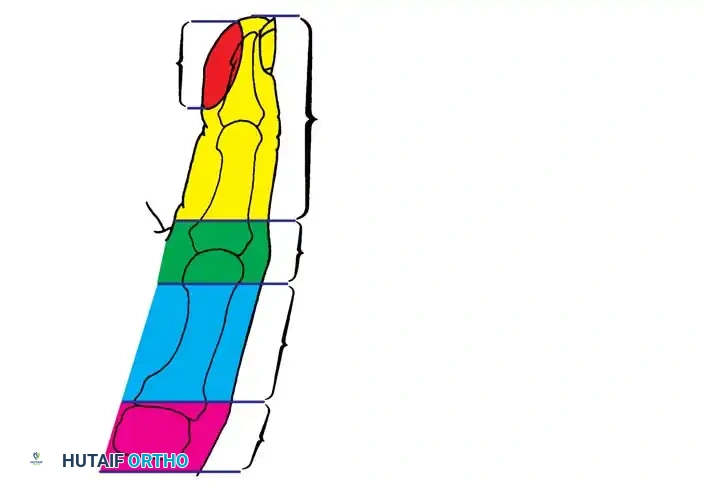
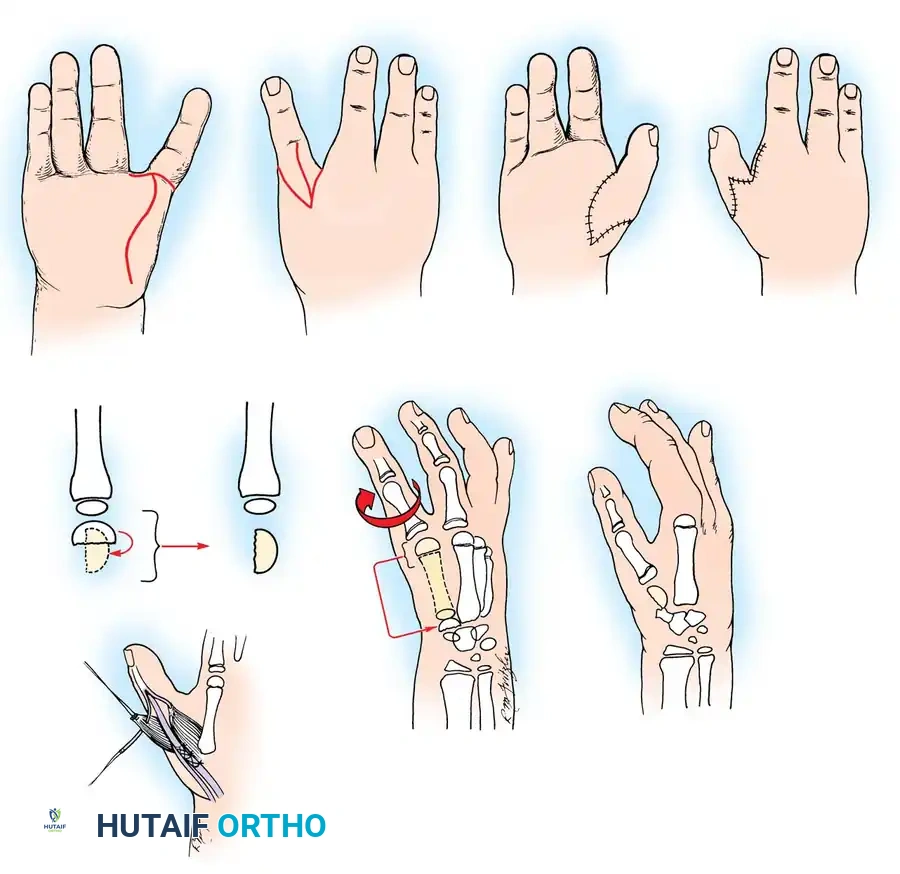
The Gillies-Millard "Cocked Hat" Procedure
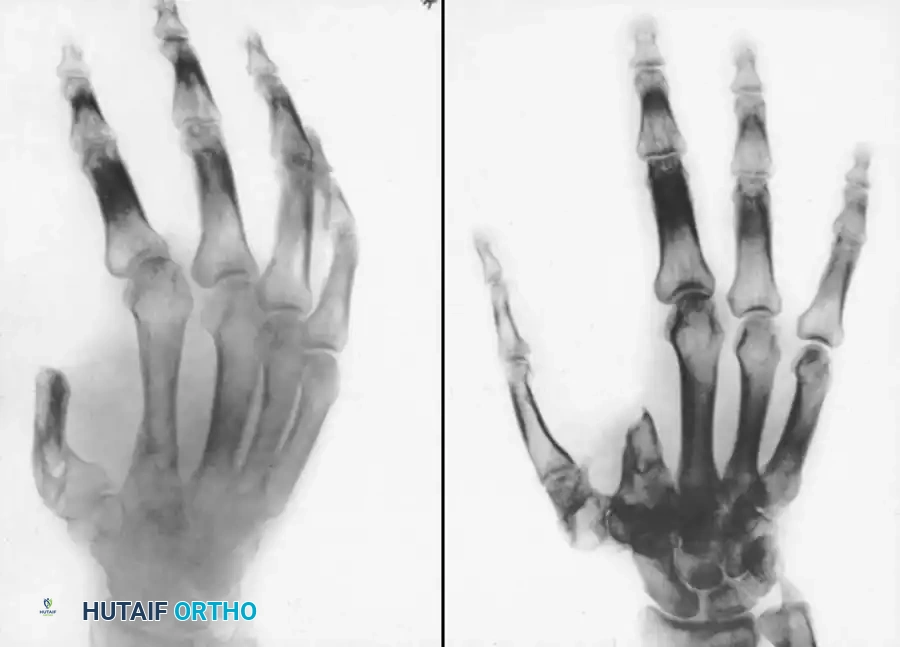
For thumb reconstruction via metacarpal lengthening, a curved, horseshoe-shaped incision is made around the dorsal, radial, and volar aspects of the base of the thumb. The skin is undermined distally, staying strictly superficial to the main venous drainage network to prevent venous congestion and subsequent flap necrosis. This undermining continues until a hollow, thimble-like flap is elevated and slipped off the end of the bony stump. A cortico-cancellous bone graft, harvested from the iliac crest, is meticulously shaped and pegged into the medullary canal of the remaining metacarpal. It is rigidly fixed using crossed Kirschner wires or a low-profile titanium mini-plate. The sensate "cocked hat" skin flap is then draped over the bone graft. The resulting proximal soft-tissue defect at the base of the thumb is subsequently covered with a split-thickness skin graft or a local transposition flap.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, revision amputation and hand reconstruction carry a significant risk of complications. The most vexing complication is the recurrence of a painful neuroma, which occurs in approximately 10-20% of standard excision and relocation procedures. Recurrent neuromas are notoriously difficult to manage, as the available nerve length diminishes with each subsequent resection. When a neuroma recurs, salvage management often dictates the utilization of advanced nerve handling techniques, such as RPNI or TMR, or the implantation of a peripheral nerve stimulator to modulate the pain signals centrally.
Soft tissue complications, particularly flap necrosis and delayed wound healing, are prevalent in patients with compromised vascularity, such as heavy smokers or those with severe crush injuries. Partial necrosis of a Moberg flap or a Gillies-Millard advancement flap can expose the underlying bone or bone graft, leading to osteomyelitis. Incidence of flap necrosis ranges from 5-15% depending on patient comorbidities. Salvage in these scenarios requires immediate aggressive debridement of necrotic tissue and the application of more robust coverage, such as a cross-finger flap, a reverse radial forearm flap, or even a free microvascular tissue transfer. Flexion contractures are another severe complication, particularly if the Moberg flap is extended proximal to the PIP joint in a triphalangeal digit.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Prevention |
|---|---|---|---|
| Recurrent Neuroma | 10 - 20% | Failure to resect proximal to zone of injury; inadequate soft tissue bed; lack of target end-organ. | Revision excision with TMR (Targeted Muscle Reinnervation) or RPNI; peripheral nerve stimulation. |
| Flap Necrosis (Partial/Total) | 5 - 15% | Undue tension on closure; venous congestion; arterial insufficiency; smoking. | Aggressive debridement; salvage with regional flaps (e.g., cross-finger flap) or free tissue transfer. |
| Bone Graft Nonunion / Resorption | 5 - 10% | Inadequate rigid fixation; poor vascularity of the soft tissue envelope; infection. | Revision bone grafting with rigid plate fixation; utilization of vascularized bone grafts if necessary. |
| Severe Flexion Contracture | 10 - 25% (if improperly designed) | Extending volar advancement flaps proximal to the PIP joint; inadequate post-op splinting. | Surgical release of adherent flexor tendons; Z-plasty of volar skin; aggressive hand therapy. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following stump revision and hand reconstruction is as critical as the surgical execution itself. The protocol is meticulously phased to protect surgical repairs while aggressively preventing joint stiffness and cortical reorganization associated with chronic pain. Phase 1 (Weeks 0-2) focuses on wound healing, edema control, and strict protection of the surgical site. The limb is immobilized in a bulky, non-compressive dressing and strictly elevated. For bone grafting procedures like the Gillies-Millard, a rigid thumb spica splint is utilized. Pain management during this phase is multimodal, utilizing scheduled acetaminophen, NSAIDs, and short courses of targeted neuropathic agents.
Phase 2 (Weeks 2-6) commences following suture removal. This phase marks the initiation of rigorous desensitization therapies. Patients are instructed to gently massage the stump with varying textures (silk, cotton, Velcro) to bombard the somatosensory cortex with non-noxious stimuli, thereby downregulating pain pathways. Gentle active range of motion (AROM) of the adjacent uninvolved joints is initiated to prevent tendon adhesions. For patients who have undergone the Krukenberg procedure, intensive rehabilitation begins at 2 to 3 weeks to train the patient in the independent abduction and adduction of the newly formed radial and ulnar rays, focusing heavily on utilizing the pronator teres for grasp.
Phase 3 (Weeks 6-12 and beyond) involves aggressive strengthening, sensory re-education, and functional integration. For bone reconstructions, clinical and radiographic union must be confirmed before initiating resistive exercises. Prosthetic fitting, if applicable, is initiated during this phase. The prosthetist works closely with the surgical team to ensure the socket design provides total contact without loading the newly reconstructed soft tissues or nerve beds. Sensory re-education is paramount for procedures like the Moberg flap or thumb reconstructions, utilizing stereognosis exercises to maximize the functional utility of the newly positioned sensate skin.
Summary of Landmark Literature and Clinical Guidelines
The evolution of amputation stump management and hand reconstruction is deeply rooted in landmark surgical literature. The classical description of the volar advancement flap by Erik Moberg revolutionized the management of thumb tip amputations, establishing the principle that sensate, durable coverage is paramount for prehension. His original warnings regarding the vascular limitations of this flap in triphalangeal digits remain a fundamental tenet of modern hand surgery. Similarly, the Krukenberg operation, initially described in 1917, has withstood the test of time. Despite the advent of advanced myoelectric prosthetics, contemporary literature continues to validate the Krukenberg procedure for specific patient populations, particularly blind, bilateral amputees, emphasizing the irreplaceable value of biological proprioception and tactile feedback.
In the realm of neuroma management, clinical guidelines have shifted significantly over the past decade. Historically, simple excision and proximal retraction into muscle or bone (as classically described by Dellon and Mackinnon) were the gold standard. However, recent landmark studies by Dumanian et al. on Targeted Muscle Reinnervation (TMR) and Cederna et al. on Regenerative Peripheral Nerve Interfaces (RPNI) have established new paradigms. These techniques redirect regenerating axons into functional muscle targets, significantly reducing the incidence of recurrent neuromas and phantom limb pain. Current clinical guidelines now strongly recommend the integration of TMR or RPNI during primary amputations and revision neuroma surgeries to optimize both pain outcomes and future prosthetic interfacing.
The principles of thumb reconstruction, heavily influenced by the works of Gillies and Millard, continue to guide surgical decision-making. Their "cocked hat" procedure remains a highly elegant solution for proximal amputations with intact thenar musculature. Modern literature underscores that while microvascular toe-to-thumb transfers offer superior outcomes for total thumb loss, local osteoplastic reconstructions like the Gillies-Millard technique remain highly relevant and effective, offering robust sensibility and stability without the donor site morbidity associated with free tissue transfer. Mastery of these classical techniques, combined with modern neuro-modulatory adjuncts, empowers the orthopedic surgeon to restore profound function and quality of life to patients suffering from devastating upper extremity trauma.
