Extensor Tendons: Anatomy, Surgical Repair & Tenodesis

Key Takeaway
Extensor tendon injuries require precise anatomical knowledge of the six dorsal compartments and juncturae tendinum for optimal surgical outcomes. This guide details the biomechanics, anatomical variations, and step-by-step surgical techniques for extensor tendon repair and tenodesis. Proper identification of the extensor indicis proprius and understanding the masking effect of juncturae tendinum are critical to preventing missed lacerations and ensuring successful postoperative rehabilitation.
Comprehensive Introduction and Patho-Epidemiology
The extensor mechanism of the human hand represents an evolutionary marvel of biomechanical engineering, characterized by a highly sophisticated, delicate network of tendons, retinacular structures, and intrinsic muscle insertions. Unlike their flexor counterparts, which are robust, cylindrical, and housed within well-defined, nutrient-rich synovial sheaths throughout their digital course, extensor tendons are anatomically distinct. They are flatter, thinner, possess significantly less collagen density, and are invested by a paratenon rather than a true synovial sheath distal to the extensor retinaculum. This morphological reality renders them exceptionally vulnerable to traumatic lacerations, attritional ruptures, crush injuries, and the formation of complex, motion-limiting adhesions following both trauma and surgical intervention.
Epidemiologically, extensor tendon injuries are among the most frequently encountered pathologies in hand surgery, representing a significant proportion of emergency department visits and elective reconstructive cases. The superficial location of these structures on the dorsal aspect of the hand and forearm, covered only by a thin layer of subcutaneous tissue and skin, provides minimal protection against sharp trauma, thermal burns, and abrasive forces. Consequently, occupational injuries, particularly those involving machinery or sharp implements, account for the vast majority of acute lacerations. Furthermore, the extensor tendons are highly susceptible to closed traumatic disruptions, such as the classic mallet finger (Zone I) and boutonnière deformity (Zone III), which result from sudden, forceful flexion of an actively extended digit.
Beyond acute trauma, the operating orthopedic surgeon must be intimately familiar with the patho-epidemiology of chronic attritional ruptures. These are most frequently observed in the setting of inflammatory arthropathies, particularly rheumatoid arthritis. In this patient population, synovial hypertrophy within the dorsal compartments leads to enzymatic degradation of the tendon substance, while concurrent carpal instability and dorsal subluxation of the ulnar head create abrasive bony prominences. This culminates in the classic Vaughan-Jackson syndrome, characterized by the sequential rupture of the extensor tendons beginning on the ulnar side (extensor digiti minimi) and progressing radially. Similarly, attrition ruptures of the extensor pollicis longus (EPL) are a well-documented complication following minimally displaced or non-operatively managed distal radius fractures, occurring as the tendon traverses the narrow, rigid fibro-osseous tunnel of the third dorsal compartment adjacent to Lister's tubercle.
Mastering the surgical management of extensor tendon injuries requires an exhaustive understanding of the topographical anatomy, the biomechanical interplay between the extrinsic and intrinsic systems, and the myriad anatomical variations that routinely present during surgical exploration. The topographical classification of these injuries relies on Verdan's zones, which divide the extensor mechanism into eight distinct regions (with a ninth zone in the forearm). Odd-numbered zones correspond to the articular regions (distal interphalangeal, proximal interphalangeal, metacarpophalangeal, and radiocarpal joints), while even-numbered zones correspond to the intervening diaphyseal segments. This comprehensive guide details the surgical anatomy, clinical evaluation, and advanced operative techniques—including primary repair, tenodesis, and pull-out wire fixation—required for the successful management of these complex injuries.
Detailed Surgical Anatomy and Biomechanics
The Six Dorsal Compartments
The topographical organization of the extensor tendons at the level of the radiocarpal joint is defined by the extensor retinaculum, a robust, transverse fibrous band that prevents bowstringing of the tendons during active wrist extension. The retinaculum compartmentalizes the dorsal wrist into six distinct fibro-osseous tunnels. From radial to ulnar, these compartments house specific tendon cohorts, each with unique biomechanical roles and clinical implications. The first compartment contains the extensor pollicis brevis (EPB) and the abductor pollicis longus (APL). This is the anatomical epicenter of De Quervain's tenosynovitis. Surgeons must maintain a high index of suspicion for anatomical variations here, as the APL frequently presents with multiple tendinous slips, and a distinct sub-compartmental septum separating the EPB and APL is present in a significant percentage of the population, failure to release which leads to refractory symptoms.
The second compartment houses the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB), the primary dorsiflexors of the wrist. The ECRB inserts centrally at the base of the third metacarpal, making it the most effective wrist extensor, while the ECRL inserts at the base of the second metacarpal. The third compartment contains the singular extensor pollicis longus (EPL). The EPL tendon takes a critical 45-degree ulnar-to-radial turn around Lister's tubercle, a bony prominence on the dorsal distal radius. This angulation creates a mechanical pulley but also subjects the tendon to significant friction and potential ischemia in the "watershed" area, predisposing it to delayed rupture following distal radius trauma.
The fourth compartment is the most capacious, containing the four tendons of the extensor digitorum communis (EDC) and the extensor indicis proprius (EIP). The EIP consistently lies ulnar and deep to the EDC of the index finger, a critical relationship to verify during tendon transfers. The fifth compartment contains the extensor digiti quinti (EDQ), also known as the extensor digiti minimi (EDM), which typically presents with two slips. Finally, the sixth compartment houses the extensor carpi ulnaris (ECU). The ECU is unique as it is stabilized within the ulnar groove by a dedicated subsheath distinct from the overlying extensor retinaculum. Disruption of this subsheath leads to painful snapping and volar subluxation of the ECU tendon during forearm supination and wrist flexion.
Anatomical Variations of the Extensor Tendons
The anatomy of the extensor tendons is notoriously variable, and relying rigidly on textbook descriptions without anticipating anomalies is a frequent source of surgical error, particularly during tendon transfers or when attempting to identify lacerated stumps in complex trauma. The EIP and EDQ are particularly prone to morphological variations. In landmark cadaveric studies, the anatomical patterns of the extensors to the fingers have been extensively mapped, revealing that the "standard" configuration is present in only a fraction of patients.
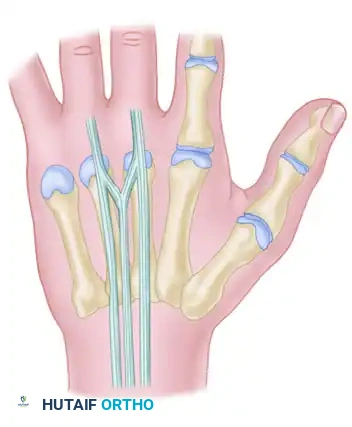
The most common patterns observed include a single extensor indicis proprius (EIP) inserting to the ulnar side of the index extensor digitorum communis (EDC). However, anomalous slips, such as an extensor indicis et medii communis (supplying both index and long fingers) or an extensor medii proprius, are occasionally encountered. The EDC itself demonstrates significant variability: a single EDC to the index finger and long finger is common, but a double EDC to the ring finger is frequently observed. Most notably, the EDC to the small finger is frequently absent or merely a vestigial slip, rendering the small finger entirely dependent on the EDQ for independent extension.
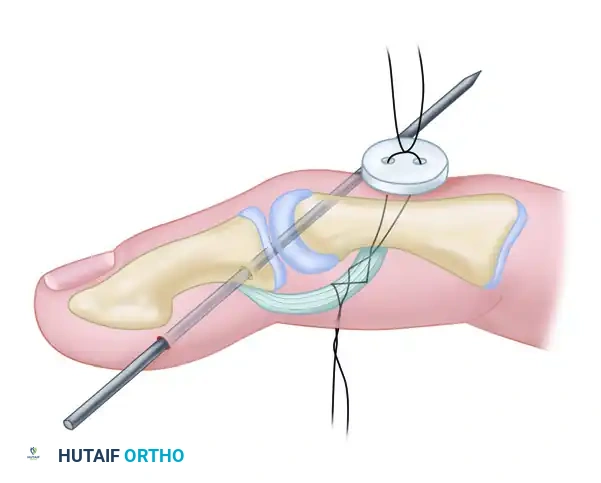
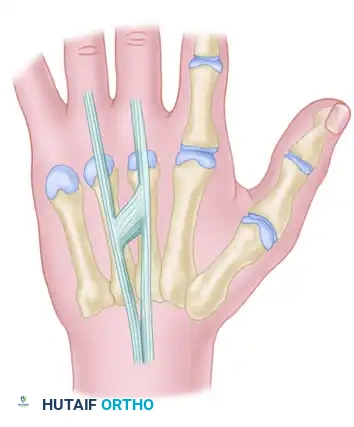
FIGURE 66-62: Most common pattern of extensor tendons on the dorsum of the hand, illustrating the single EIP, single EDC to index and long fingers, double EDC to the ring finger, absent EDC to the small finger, and double EDQ.
Extensor indicis proprius (EIP) anatomy, demonstrating its classic ulnar relationship to the EDC of the index finger.
The Juncturae Tendinum
The juncturae tendinum are intricate intertendinous connections located in the intermetacarpal spaces, proximal to the metacarpophalangeal (MCP) joints (Zone VI). These structures serve a vital biomechanical role by coordinating digital extension, distributing extensor forces across the dorsal hand, and stabilizing the EDC tendons over the metacarpal heads to prevent ulnar subluxation during flexion. However, they act as a double-edged sword in the setting of trauma; their force-transmitting capabilities can mask complete proximal tendon lacerations, leading to delayed diagnosis and treatment.
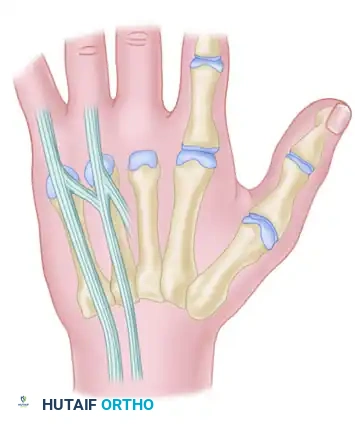
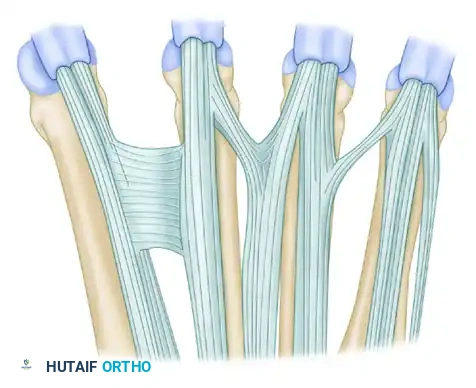
FIGURE 66-63: Overview of the Juncturae Tendinum classifications.
The juncturae are morphologically classified into three primary types based on their thickness, orientation, and location. Type 1 juncturae are thin, filamentous bands found predominantly between the EDC tendons of the long (EDC m) and index (EDC i) fingers. Notably, these filamentous connections do not connect to the EIP tendon, preserving the independent extension capability of the index finger. They are typically located in the second and third intermetacarpal spaces.
Type 2 juncturae are thicker, more robust, and highly organized fibrous connections found between the EDC tendons of the ring (EDC r) and long (EDC m) fingers. They are located exclusively in the third and fourth intermetacarpal spaces and play a significant role in restricting the independent extension of the ring finger when the adjacent digits are flexed.
Type 3 juncturae are the most complex and are further subdivided. Subtype 3y presents as a Y-shaped tendon bifurcation, appearing as a split tendon inserting into two adjacent digits, most commonly seen between the EDC tendons of the ring (EDC r) and long (EDC m) fingers. Subtype 3r is a more oblique, R-shaped junctura, typically bridging the EDC to the ring finger (EDC r) and the most radial of the EDQ tendons to the small finger. Understanding these specific connections is critical when evaluating a patient with a suspected Zone VII or VIII laceration.

Additional anatomical variations and interconnections of the dorsal extensor mechanism further complicate dorsal hand reconstruction. Surgeons must carefully dissect and preserve these structures when possible, or meticulously repair them if divided during exposure, to maintain the coordinated kinematics of the extensor apparatus.


Exhaustive Indications and Contraindications
The decision-making process for extensor tendon surgery requires a nuanced evaluation of the injury chronicity, the anatomical zone of disruption, the condition of the overlying soft tissue envelope, and the patient's physiological capacity to participate in rigorous postoperative rehabilitation. Primary end-to-end repair is the undisputed gold standard for acute lacerations (typically defined as those presenting within 7 to 14 days of injury). In these cases, the tendon ends can usually be approximated without excessive tension, and the paratenon can be preserved to facilitate optimal gliding.
For chronic injuries, delayed presentations, or attritional ruptures where a substantial tendon gap exists or the tendon substance is severely degraded, primary repair is often impossible or biomechanically unsound. In such scenarios, indications shift toward advanced reconstructive techniques. Tendon transfers (e.g., EIP to EPL transfer for chronic EPL ruptures) are highly indicated to restore function using a dispensable, synergistic motor unit. Interpositional tendon grafting (using palmaris longus or plantaris autografts) is indicated when multiple tendons are involved, or a suitable transfer is unavailable. Tenodesis and pull-out wire fixation are specifically indicated for bony avulsions of the terminal tendon (bony mallet finger with >30% articular surface involvement or volar subluxation) or robust central slip reconstructions.
Contraindications to definitive extensor tendon repair or reconstruction must be strictly observed to prevent catastrophic surgical failures. Active, uncontrolled infection in the surgical field is an absolute contraindication; in such cases, thorough debridement, irrigation, and delayed reconstruction are mandatory. A severely compromised soft tissue envelope—such as full-thickness necrosis, severe crush injury, or inadequate skin coverage—precludes immediate tendon repair, as tendons will not heal and will rapidly necrose if left exposed or covered by ischemic tissue. In these instances, staged reconstruction utilizing silicone tendon rods (Hunter rods) following soft tissue coverage (e.g., pedicled or free flaps) is the appropriate salvage pathway.
| Factor | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Acute Trauma (< 2 weeks) | Complete lacerations (>50% tendon width); Zone I-VIII disruptions; Open fractures with tendon injury. | Active purulent infection; Hemodynamic instability; Inadequate soft tissue envelope. |
| Chronic/Delayed (> 4 weeks) | Functional deficit with supple joints; Attritional ruptures (e.g., EPL, Vaughan-Jackson); Failed conservative management. | Fixed joint contractures (stiff joints must be mobilized first); Severe untreated carpal collapse/instability. |
| Specific Techniques | Tenodesis/Pull-out wire: Bony mallet with volar subluxation; Central slip avulsions. Tendon Transfer: Unrepairable gap; Degraded muscle belly. | Primary Repair: Gap > 3cm in chronic setting; Severely frayed, "mop-end" tendon stumps incapable of holding suture. |
| Patient Factors | High functional demand; Compliant with complex postoperative rehabilitation protocols. | Severe cognitive impairment precluding rehab compliance; Uncontrolled psychiatric conditions. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning begins with a meticulous clinical examination designed to isolate specific tendon functions and overcome the deceptive biomechanics of the hand. The masking effect of the juncturae tendinum is a classic diagnostic pitfall. When a single extensor tendon is divided at the wrist or proximal dorsum (Zone VII or VIII), partial or even complete extension of the affected finger may still be possible because intact adjacent tendons transmit extensor forces through the juncturae. The examiner must test independent extension of each digit against resistance. For example, to test the EDC, the examiner should ask the patient to extend the fingers with the MCP joints hyperextended and the IP joints flexed, effectively neutralizing the intrinsic muscles.
Evaluating the Extensor Pollicis Longus (EPL) requires strict isolation due to the compensatory actions of the intrinsic thumb muscles and the Extensor Pollicis Brevis (EPB). An intact EPB can extend the thumb MCP joint, and the abductor pollicis brevis and adductor pollicis can assist with interphalangeal (IP) extension via their contributions to the dorsal apparatus. Proper EPL testing requires the examiner to stabilize the thumb MCP joint in neutral and test for active extension of the IP joint against resistance. Furthermore, the patient should be asked to place their hand flat on a table (palm down) and actively lift the thumb off the surface (retropulsion); inability to perform this maneuver is pathognomonic for EPL dysfunction.
Imaging modalities play a crucial adjunctive role. Standard orthogonal radiographs of the hand and wrist are mandatory to rule out concurrent fractures, foreign bodies, or bony avulsions (e.g., mallet fractures). High-resolution musculoskeletal ultrasound is increasingly utilized in the clinic to dynamically assess tendon continuity, measure gap distances, and identify retracted tendon stumps, thereby facilitating precise surgical incisions. MRI is rarely required for acute trauma but is invaluable for evaluating chronic attritional ruptures, tenosynovitis, or complex soft tissue masses compressing the extensor compartments.
Preoperative preparation and positioning are critical for optimal surgical execution. The procedure can be performed under regional anesthesia (axillary or supraclavicular block) or general anesthesia. However, Wide-Awake Local Anesthesia No Tourniquet (WALANT) has revolutionized extensor tendon surgery. By utilizing a mixture of lidocaine, epinephrine, and sodium bicarbonate, WALANT provides excellent hemostasis and profound local anesthesia without the need for a pneumatic tourniquet. Crucially, WALANT allows the surgeon to ask the awake patient to actively extend their fingers intraoperatively, enabling dynamic assessment of the tendon repair tension, evaluation of tendon gliding, and immediate identification of any gapping at the repair site. If traditional anesthesia is used, the patient is positioned supine with the arm extended on a radiolucent hand table, and a pneumatic tourniquet is applied to the proximal arm, inflated to 250 mmHg after exsanguination.
Step-by-Step Surgical Approach and Fixation Technique
Surgical exposure of the extensor tendons must be meticulously planned to preserve the delicate dorsal skin flaps and the underlying paratenon. Straight longitudinal incisions over the joints should be strictly avoided to prevent functionally limiting scar contractures. Instead, lazy-S, zig-zag (Brunner), or geometrically designed incisions are utilized to cross joint flexion creases obliquely. When exposing the dorsal compartments of the wrist, the extensor retinaculum should be preserved whenever possible. If division is absolutely necessary to retrieve retracted tendon stumps or decompress a compartment, the retinaculum should be stepped or Z-lengthened. This allows for an anatomical, tension-free repair at the conclusion of the case, preventing the catastrophic complication of postoperative tendon bowstringing.
For acute mid-substance lacerations (Zones IV-VIII), primary end-to-end repair is performed. The tendon ends are meticulously debrided of non-viable tissue. A core suture is placed using a 3-0 or 4-0 non-absorbable monofilament or braided synthetic suture. Biomechanical studies have demonstrated that multi-strand repairs (e.g., 4-strand modified Kessler or cruciate techniques) provide superior tensile strength, allowing for early active motion protocols. A 6-0 running epitendinous suture is then placed circumferentially around the repair site. This epitendinous stitch is critical; it not only increases the overall construct strength by 20-30% but also smooths the repair site, significantly reducing the risk of postoperative adhesions and improving tendon excursion.
When anchoring an extensor tendon directly to bone—such as in the treatment of distal phalanx avulsions (bony mallet fingers), chronic central slip reconstructions, or specific ligamentous repairs—a more robust fixation method is required. The tenodesis button and pull-out wire technique, combined with transarticular Kirschner wire (K-wire) stabilization, provides exceptional biomechanical rigidity, neutralizing deforming forces while bony healing occurs.

Surgical diagram illustrating the trajectory of tendon repair and the complex interplay of the dorsal apparatus during fixation.
Step-by-Step Surgical Protocol for Tenodesis (Button and Pull-Out Wire):
- Joint Stabilization: The procedure begins by anatomically reducing the involved joint to the desired position (e.g., strict neutral or slight hyperextension for mallet injuries). A smooth Kirschner wire (typically 0.035 or 0.045 inch) is driven retrogradely or antegradely across the joint to rigidly neutralize deforming forces. The K-wire is cut flush beneath the skin to minimize the risk of pin tract infections.
- Bone Preparation: The anatomical footprint of the tendon insertion is identified. Using a micro-burr or a fine drill bit, a small cortical window or a series of osseous tunnels are created to expose bleeding cancellous bone, which is essential for robust tendon-to-bone integration.
- Tendon Preparation: A heavy non-absorbable suture (e.g., 2-0 or 3-0 Prolene) or a fine stainless steel wire is woven through the distal stump of the tendon using a Bunnell or Krackow grasping technique. This provides a secure hold on the flat, thin extensor tendon.
- Passing the Suture: Straight Keith needles are attached to the suture ends and passed through the prepared bony tunnels, exiting the volar aspect of the digit. Tensioning these sutures draws the tendon stump directly into the cortical window.
- Dorsal Button Fixation: The needles are passed through the volar skin. The sutures are then tied securely over a sterile surgical button resting on the volar pad of the finger. The button acts as a load-distributing device, preventing the sutures from cutting through the skin and causing ischemic necrosis.
- Pull-Out Wire Routing: A secondary pull-out loop is often incorporated dorsally, allowing for the eventual removal of the entire suture construct once definitive bony or fibrous union has been achieved (typically at 4-6 weeks).
- Wound Closure: The wound is copiously irrigated. The skin is closed with 5-0 or 6-0 nylon in a simple interrupted fashion. Meticulous care is taken to approximate the paratenon over the repair site to facilitate gliding and prevent skin adherence.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, extensor tendon repairs are fraught with potential complications, primarily due to the delicate nature of the tendons, their superficial location, and the complex biomechanics of the hand. The most frequent complication is the formation of dense peritendinous adhesions. Because the extensor tendons lack a true synovial sheath over the digits and metacarpals, they rely on the surrounding paratenon and subcutaneous tissues for vascularity. Surgical trauma and subsequent hematoma organization inevitably lead to scar tissue that tethers the tendon to the overlying skin or underlying bone, resulting in a profound loss of digital flexion.
Conversely, aggressive early rehabilitation or inadequate surgical fixation can lead to stretching of the repair site or complete rupture, manifesting clinically as an extensor lag. An extensor lag is defined as a deficit in active extension despite full passive extension. A lag of 10-15 degrees at the DIP joint is relatively common following mallet finger treatment and is often functionally tolerated. However, a significant lag at the PIP or MCP joint severely compromises hand function and grip strength. Infection, while less common, is a devastating complication that can lead to rapid tendon necrosis, osteomyelitis, and complete failure of the reconstruction.
Salvage management requires careful timing and patient selection. Tenolysis (the surgical release of adhesions) is indicated for severe stiffness but must be delayed until the soft tissues have reached maximal medical improvement (typically 4 to 6 months post-injury). The patient must have supple joints passively and be highly motivated, as post-tenolysis rehabilitation is grueling. If the tendon has ruptured or stretched beyond functional utility, staged reconstruction utilizing tendon grafts or transfers becomes necessary.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Peritendinous Adhesions | 20% - 40% | Prolonged immobilization; Severe crush injury; Poor hemostasis; Failure to repair paratenon. | Intensive hand therapy; Dynamic flexion splinting; Surgical tenolysis (delayed 4-6 months). |
| Extensor Lag (Stretching) | 15% - 30% | Inadequate core suture strength; Premature aggressive active flexion; Non-compliance with splinting. | Reinstitute extension splinting (nighttime); If functionally limiting and chronic, consider secondary shortening or tendon transfer. |
| Tendon Rupture | 3% - 7% | Technical failure of knot; Overly aggressive therapy; Undiagnosed infection; Attritional wear. | Revision primary repair (if acute); Tendon grafting or tendon transfer (if chronic/retracted). |
| Infection | 1% - 3% | Contaminated open wounds; Exposed K-wires; Button necrosis on volar pad. | Immediate hardware removal (if unstable); I&D; Intravenous antibiotics; Delayed reconstruction. |
| Bowstringing | Rare (<1%) | Failure to reconstruct or step-cut the extensor retinaculum during Zone VII exposures. | Surgical reconstruction of the retinaculum using local fascial flaps or extensor retinacular grafts. |
Phased Post-Operative Rehabilitation Protocols
The ultimate functional outcome of an extensor tendon repair is equally dependent on the precision of the surgical execution and the strict adherence to a scientifically designed postoperative rehabilitation protocol. The delicate balance between protecting the healing tendon from excessive tension (which causes gapping or rupture) and providing sufficient excursion to prevent restrictive adhesions (which cause stiffness) is the central challenge of hand therapy. Historically, extensor tendons were managed with static immobilization for 4 to 6 weeks. However, this reliably produced severe adhesions. Modern protocols heavily favor Early Active Motion (EAM) or Relative Motion Extension (RME) splinting.
The Immediate Postoperative Phase (0-3 Weeks) focuses on wound healing, edema control, and controlled tendon gliding. Immediately post-surgery, a bulky, non-compressive dressing is applied. Within 3 to 5 days, the patient is transitioned to a custom orthosis. For Zones IV-VII, the Relative Motion Extension (RME) splint (often referred to as the ICAM protocol) has revolutionized care. This splint holds the injured digit in 15-20 degrees of relative extension compared to the adjacent uninjured digits at the MCP joint. Because the EDC tendons share a common muscle belly and are interconnected by the juncturae tendinum, this relative extension significantly unloads the tension on the repaired tendon while allowing the patient to actively flex and extend the wrist and digits. This promotes differential tendon gliding and dramatically reduces adhesion formation.
The Intermediate Phase (3-6 Weeks) marks the transition from early healing to active remodeling. At 3 to 4 weeks, pull-out wire sutures (if utilized for tenodesis) are removed in the clinic. Transarticular K-wires are typically removed between 4 and 6 weeks, once radiographic or clinical evidence of sufficient tendon-to-bone healing is confirmed. Once hardware is removed, active range of motion (AROM) of the involved joints is aggressively progressed. Flexion is introduced gradually; the therapist carefully monitors for the development of an extensor lag. If a lag develops, the therapy is decelerated, and extension splinting is increased.
The Late Phase (6+ Weeks) focuses on restoring full functional capacity, grip strength, and endurance. Heavy resistance activities, forceful gripping, and return to manual labor or contact sports are strictly prohibited until at least 8 to 10 weeks postoperatively, as the tendon remodeling phase continues for several months. If severe adhesions limit flexion during this phase, dynamic flexion splinting (e.g., a dynamic PIP flexion orthosis) may be initiated. Conversely, if an extensor lag persists, prolonged nighttime extension splinting for up to 12 weeks may be necessary to allow the tendon to shorten and remodel at the proper resting length.
Summary of Landmark Literature and Clinical Guidelines
The evolution of extensor tendon surgery is deeply rooted in landmark anatomical studies and paradigm-shifting biomechanical research. Claude Verdan's original topographical classification system (Zones I-VIII) remains the universal language by which hand
