Surgical Restoration of Intrinsic Finger Function: Biomechanics and Tendon Transfers
Key Takeaway
The restoration of intrinsic finger function addresses the debilitating clawhand deformity caused by ulnar and median nerve palsies. By preventing metacarpophalangeal hyperextension, the long extensors can effectively extend the interphalangeal joints. This guide details the biomechanics, indications, and step-by-step surgical techniques for dynamic tendon transfers and static capsulodesis procedures to restore synchronized grasp and pinch kinematics.
Comprehensive Introduction and Patho-Epidemiology
The profound functional devastation resulting from the loss of intrinsic muscle function in the hand represents one of the most challenging reconstructive paradigms in orthopedic and hand surgery. The intrinsic musculature—comprising the lumbricals, dorsal and volar interossei, and the hypothenar and thenar groups—serves as the critical biomechanical modulator of the digital sweep. When these muscles are paralyzed, typically as a sequela of low median and ulnar nerve lesions, Hansen’s disease (leprosy), Charcot-Marie-Tooth disease, or devastating compartment syndromes, the hand undergoes a predictable and severely disabling collapse into the classic "clawhand" (main en griffe) deformity.
In low nerve lesions, the pathology is uniquely characterized by selective intrinsic paralysis while the long extrinsic muscles—innervated more proximally in the forearm—remain fully functional. This creates a severe, unopposed biomechanical imbalance. The extrinsic extensor digitorum communis (EDC) exerts an unchecked extension moment on the metacarpophalangeal (MCP) joints, while the flexor digitorum profundus (FDP) and flexor digitorum superficialis (FDS) exert an unopposed flexion moment on the interphalangeal (IP) joints. The resultant posture is one of rigid MCP hyperextension and IP flexion, fundamentally destroying the hand's capacity for synchronized digital flexion, powerful grasp, and stable pinch kinematics.
Epidemiologically, while Hansen's disease remains a leading cause of intrinsic minus hands globally, traumatic peripheral nerve injuries dominate the etiology in industrialized nations. The primary goal of surgical intervention is the dynamic restoration of intrinsic finger function. This exhaustive chapter details the intricate pathomechanics of intrinsic minus hands, the critical preoperative considerations, and the definitive textbook surgical techniques for dynamic tendon transfers and static stabilization, providing the reconstructive surgeon with the requisite knowledge to restore functional prehension.
Detailed Surgical Anatomy and Biomechanics
To effectively reconstruct the intrinsically paralyzed hand, the surgeon must possess a flawless, three-dimensional understanding of digital biomechanics and the extensor aponeurosis. The intrinsic muscles do not merely flex the MCP joints and extend the IP joints; they are the primary stabilizers of the digits in three-dimensional space. The lumbricals, originating from the FDP tendons, are unique in that they connect a flexor to an extensor, acting as highly sensitive proprioceptive modulators that prevent the FDP from overpowering the extensor mechanism during fine motor tasks.
The interossei, both dorsal (abductors) and volar (adductors), insert via complex lateral bands into the dorsal apparatus. Biomechanically, the intrinsic muscles possess a moment arm for MCP flexion that is significantly greater than their moment arm for IP extension. Therefore, their primary mechanical role is to stabilize the MCP joint in varying degrees of flexion, which subsequently allows the extrinsic EDC to transmit its excursion distally to extend the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints via the central slip and terminal tendon, respectively.
Pathomechanics of the Clawhand Deformity
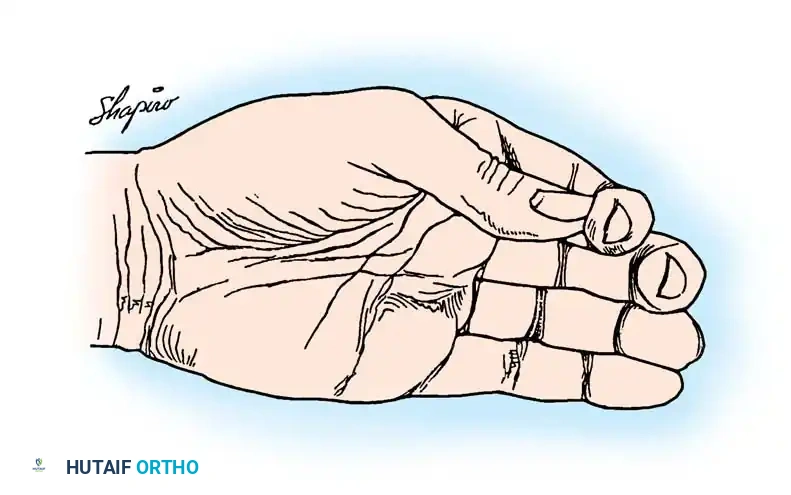
Loss of intrinsic muscle power leads directly to the collapse of the longitudinal and transverse arches of the hand. The hyperextension of the MCP joints is driven by the EDC, which, lacking the antagonistic flexion force of the intrinsics, pulls the proximal phalanx dorsally. However, MCP hyperextension itself is not the most disabling aspect of this paralysis; rather, it is the profound loss of grasp mechanics and the temporal dyssynchrony of digital flexion.
Clinical and biomechanical studies demonstrate that with intrinsic paralysis, overall grip strength is diminished by 50% to 70%. This profound weakness is directly attributable to the absence of primary flexion power at the MCP joints, forcing the hand to rely solely on the less mechanically advantaged extrinsic flexors. Furthermore, the paralysis induces a highly inefficient, asynchronous movement during digital flexion, clinically observed as the "roll-up maneuver."
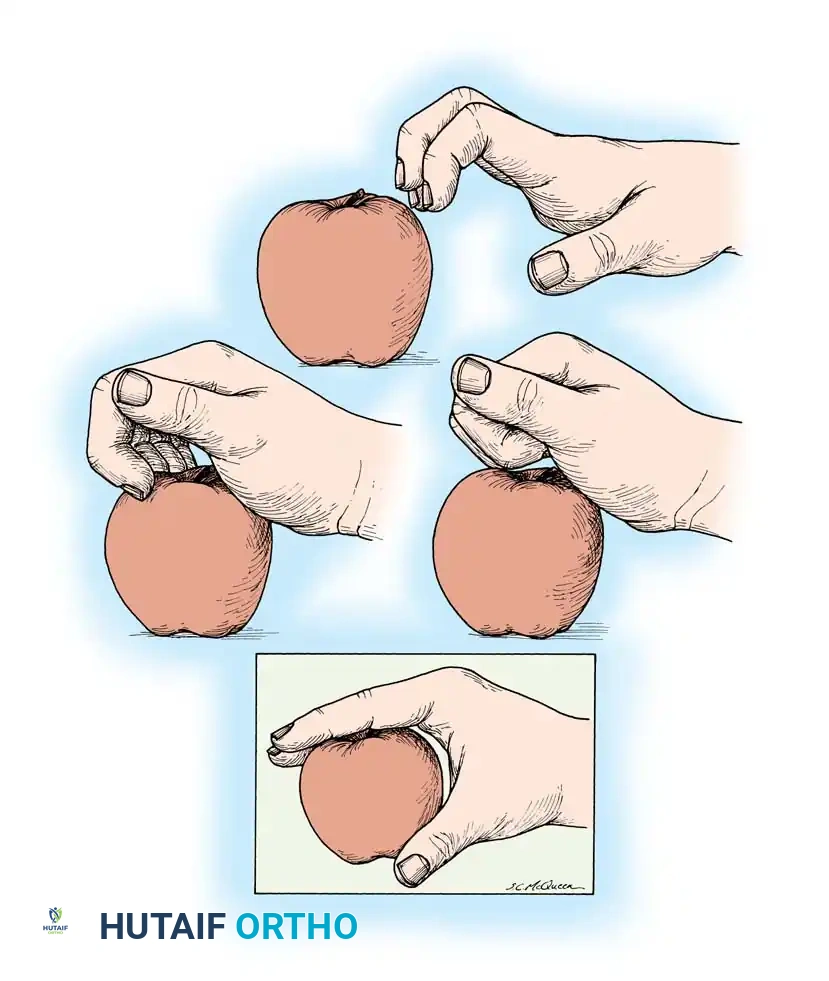
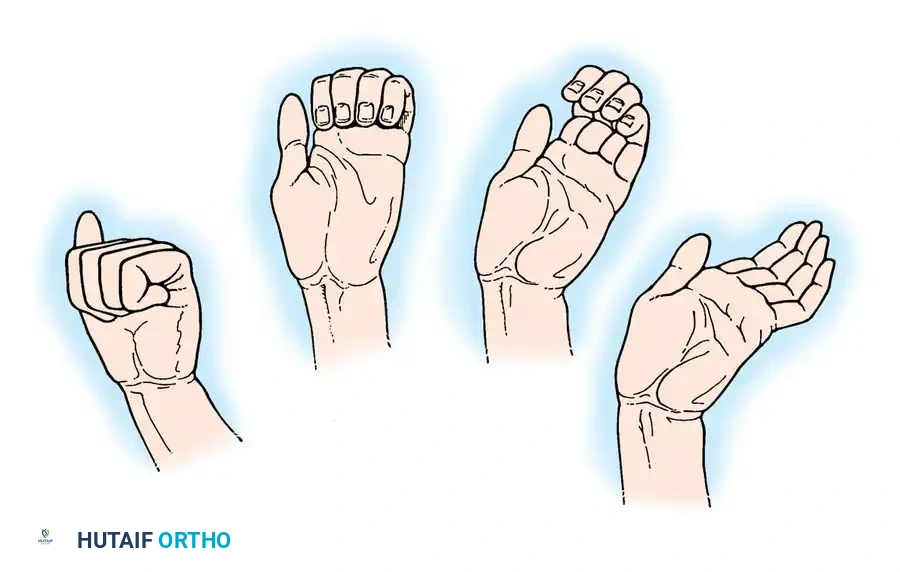
Because the intrinsic muscles normally initiate MCP flexion simultaneously with IP extension, their absence forces the long flexors to act alone. Consequently, the IP joints flex first, followed sequentially by the MCP joints. This out-of-phase flexion causes the fingers to curl prematurely into the palm. When attempting to grasp a large object, the fingertips strike the object and push it out of the hand, rather than enveloping it. This asynchronous cascade renders the hand functionally useless for handling anything larger than a small cylinder.
The Loss of Pinch Power and Lateral Stability
In addition to diminished gross grasp, the power of key pinch and tip-to-tip pinch is severely compromised. This deficit is exponentially compounded when the thenar musculature is also paralyzed, as seen in combined median and ulnar nerve lesions. Biomechanically, the collateral ligaments of the MCP joints are eccentrically attached; they are lax when the joint is in extension and taut in flexion. Without the stabilizing force of the intrinsic musculature holding the MCP joints in flexion, the digits lose critical lateral stability.
When the long extensor tendons fire, divergence of the fingers is automatic due to the anatomical splay of the metacarpals. Conversely, convergence of the fingertips during grasping is driven by the intrinsic muscles. The intrinsic muscles are therefore absolute prerequisites for stabilizing the fingers against lateral deviation forces—especially the first dorsal interosseous, which must provide rigid resistance in the index finger against the powerful pinch pressure exerted by the thumb. Without this stabilization, the index finger collapses into ulnar deviation during pinch attempts.
Exhaustive Indications and Contraindications
Surgical reconstruction of the intrinsic minus hand requires meticulous patient selection. The timing of surgery is critical; dynamic tendon transfers should only be performed when maximal spontaneous nerve recovery has plateaued, typically 12 to 18 months post-injury, or immediately in cases of irreversible nerve destruction. The cornerstone of preoperative decision-making is the Bouvier test. When the examiner passively prevents MCP hyperextension, a positive Bouvier test occurs if the patient can actively extend the PIP and DIP joints using their extrinsic extensors. A positive test indicates a simple claw deformity amenable to dynamic intrinsic transfers. A negative test indicates central slip attenuation or fixed PIP flexion contractures (complex claw), necessitating preliminary or concurrent joint release or arthrodesis.
| Parameter | Indications for Dynamic Transfer | Contraindications / Relative Exclusions |
|---|---|---|
| Neurological Status | Irreversible ulnar/median nerve palsy; stable progressive neuropathies (e.g., CMT) with functional donors. | Recovering nerve lesion; progressive, rapid neurodegenerative disorders (e.g., ALS). |
| Joint Mobility | Supple MCP and IP joints; Positive Bouvier test; full passive range of motion. | Fixed PIP flexion contractures >30°; rigid MCP hyperextension; Negative Bouvier test. |
| Donor Availability | Expendable, synergistic motor units with Grade 4/5 or 5/5 MRC strength (e.g., FDS, ECRL, ECRB). | Spasticity of donors; global weakness; lack of synergistic phase-firing donors. |
| Soft Tissue Envelope | Pliable, well-vascularized volar and dorsal skin; absence of severe scarring in routing pathways. | Severe volar scarring; inadequate soft tissue coverage; active infection. |
| Patient Factors | High compliance; cognitive ability to participate in complex motor re-education. | Non-compliance; severe cognitive impairment preventing postoperative rehabilitation. |
If a patient presents with rigid deformities or lacks expendable motor donors, static procedures such as the Zancolli capsulodesis, tenodesis, or MCP arthrodesis must be considered as salvage operations. Dynamic transfers are always the gold standard when conditions permit, as they restore the active, synchronized sweep of the digits.
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for intrinsic reconstruction is a highly analytical process requiring precise manual muscle testing (MMT) and joint assessment. The surgeon must inventory every functioning muscle in the forearm and hand. Ideal donor muscles for intrinsic replacement should have adequate excursion (approximately 3-4 cm), sufficient power, and ideally, synergistic phase firing (e.g., a wrist extensor acting to flex the fingers via tenodesis). The FDS, extensor carpi radialis longus (ECRL), extensor carpi radialis brevis (ECRB), extensor indicis proprius (EIP), and extensor digiti minimi (EDQ) are the most frequently utilized donors.
Patient positioning is standardized but requires careful attention to detail. The patient is placed supine with the operative extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm. Loupe magnification (minimum 2.5x to 3.5x) is mandatory for the meticulous dissection of the extensor aponeurosis and the precise execution of tendon weaves.
Templating involves mapping the exact routing pathways for the tendon grafts. For intrinsic restoration, the vector of pull must recreate the anatomical line of the lumbricals. This requires the grafts to pass volar to the deep transverse metacarpal ligament (DTML). The surgeon must mark the planned incisions: typically, a transverse or zigzag incision in the mid-palm to access the lumbrical canals, a dorsal longitudinal incision for donor harvest, and specific mid-axial or dorsal incisions over the proximal phalanges for graft insertion into the lateral bands.
Step-by-Step Surgical Approach and Fixation Technique
Tendon transfers to replace intrinsic function are among the most biomechanically complex and surgically demanding procedures in upper extremity reconstruction. The margin for error in tensioning and routing is minimal. No single procedure is universally accepted; the surgeon must tailor the operation to the specific functional deficits and available donors of the individual hand.
Core Principles of Surgical Reconstruction
The foundational principle of intrinsic reconstruction relies on a specific, immutable biomechanical truth: The long finger extensors are fully capable of extending the interphalangeal joints, provided that the metacarpophalangeal joints are stabilized and prevented from hyperextending.
All operations designed to correct intrinsic paralysis—whether dynamic tendon transfers or static blocks—are fundamentally based on this tenet. By preventing MCP hyperextension, the extrinsic extensors are forced to transmit their force distally to the IP joints. Furthermore, any tendon transferred from the dorsum or volar forearm to restore intrinsic function must pass volar to the deep transverse metacarpal ligament. If the graft passes dorsal to this ligament, it will act as an MCP extensor, exacerbating the claw deformity.
The Bunnell Transfer and Modifications
Originally described by Sterling Bunnell in 1942, this technique involved detaching the flexor digitorum superficialis (FDS) tendon from each finger, splitting it, and routing one slip to each side of the extensor aponeurosis via the lumbrical canals. While historically significant, the classic Bunnell transfer removes powerful flexors of the PIP joints and converts them into extensors. In supple hands, this transfer is frequently too strong, progressively pulling the PIP joints into rigid extension and creating a debilitating iatrogenic "intrinsic-plus" (swan-neck) deformity.
To mitigate this severe complication, a modified Bunnell procedure is utilized. In this iteration, only a single FDS tendon (usually harvested from the middle or ring finger) is utilized. It is split into four uniform slips and transferred to all four fingers. This modification significantly dilutes the force exerted on any single digit and is particularly useful in clawhands that already exhibit some preoperative restriction of motion in the PIP joints, where a stronger corrective force is desirable without the risk of overcorrection.
The Fowler Transfer
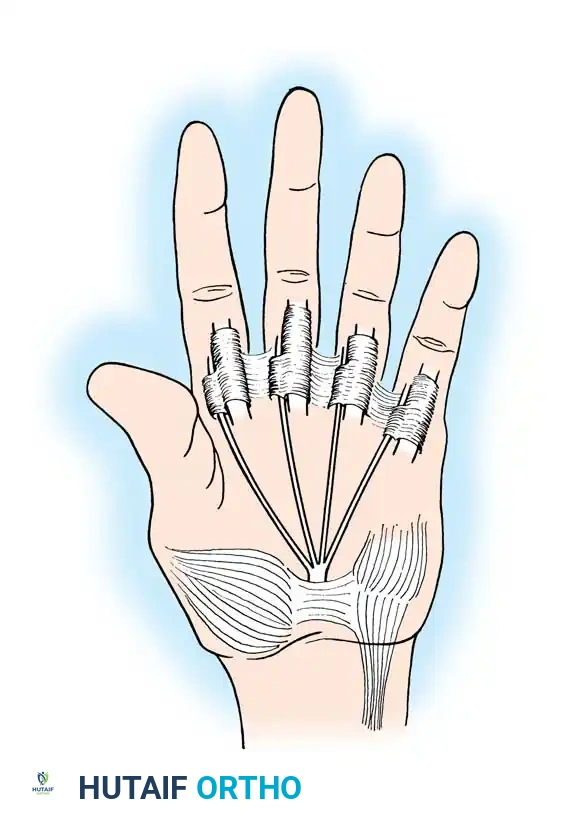
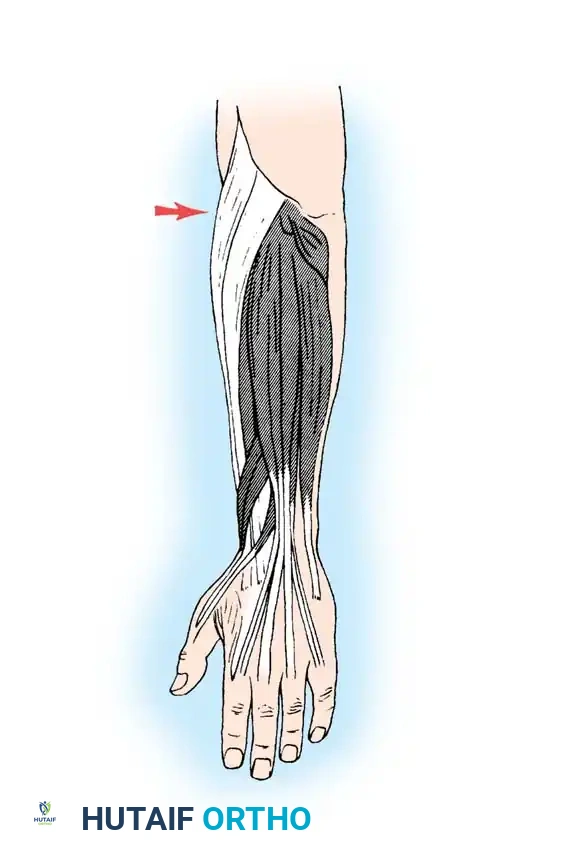
Fowler devised a highly effective transfer utilizing the extensor indicis proprius (EIP) and extensor digiti minimi (EDQ). These tendons are harvested via dorsal incisions, withdrawn proximally to the extensor retinaculum, and split longitudinally to form four distinct slips.
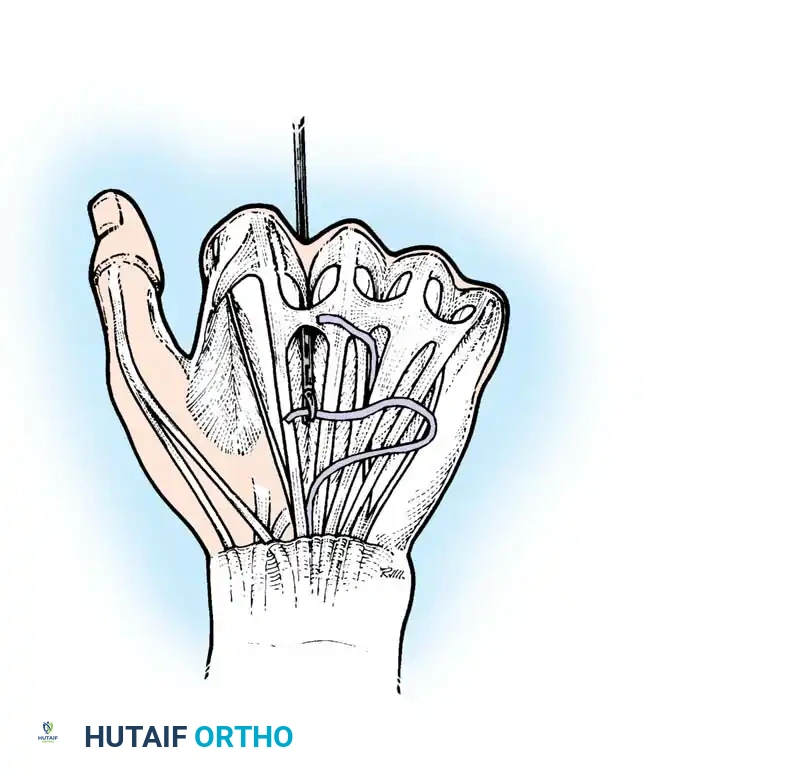
Crucially, these slips must be routed through the interosseous spaces and passed volar to the deep transverse metacarpal ligament. This precise anatomical routing is what converts the dorsal extensors into effective MCP flexors.
While the Fowler transfer is highly efficient and benefits from a synergistic tenodesing effect during wrist flexion (which naturally tightens the dorsal donors), it requires the tendon slips to be advanced approximately 2.5 cm to reach their insertion sites on the lateral bands. This places the transfer under considerable tension. If the tissue bed is scarred or the tension is miscalculated, it can occasionally lead to intrinsic overpull or graft rupture.
The Riordan Transfers
To avoid the excessive tension inherent in the Fowler transfer, Riordan introduced several elegant modifications utilizing free tendon grafts to bridge the gap between the donor motor and the insertion sites.
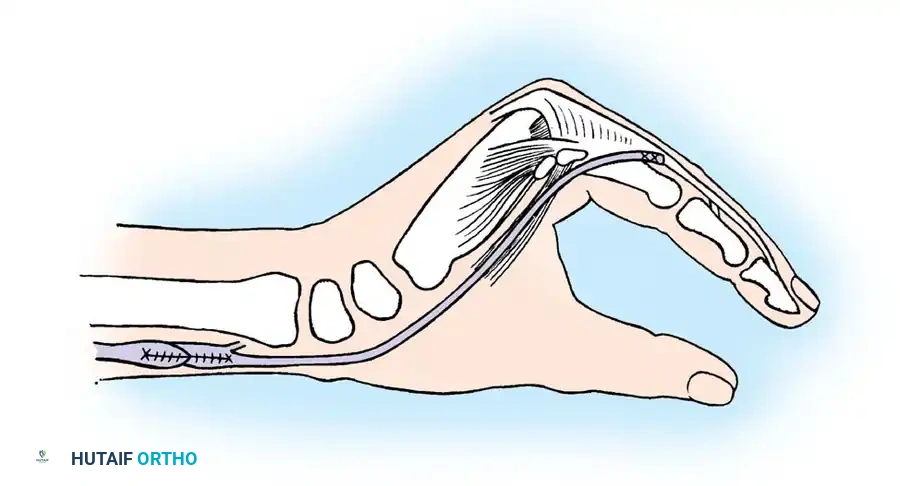
In one primary variation, the detached EIP is split into two slips, passed volar to the DTML, and attached to the radial side of the ring and little fingers. A free tendon graft (such as palmaris longus or plantaris) is then harvested and meticulously sutured to the musculotendinous junction of the EIP using a Pulvertaft weave. The distal end of this free graft is split into two slips and routed to the middle and index fingers.
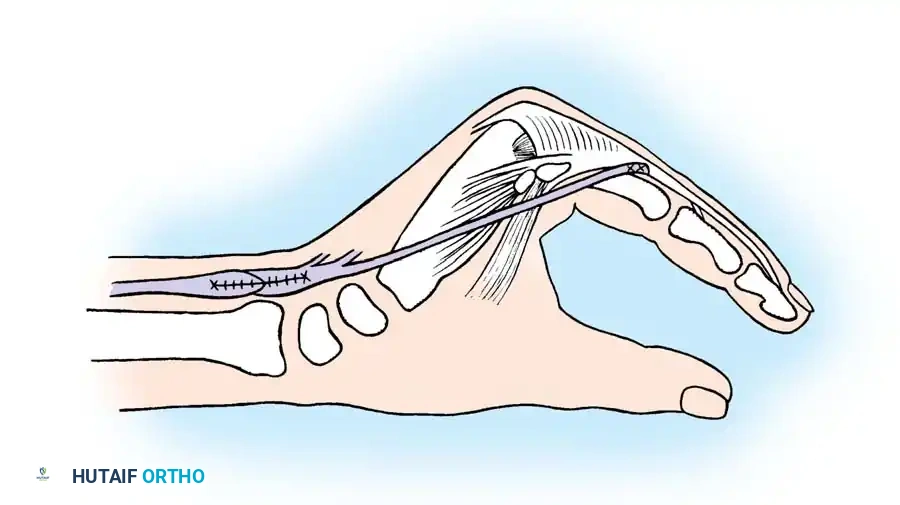
For patients with severe, long-standing clawing who have developed a chronic habit of flexing the wrist to passively extend the digits via tenodesis, Riordan advised transferring the flexor carpi radialis (FCR). The FCR insertion is freed, transferred to the dorsum of the wrist, and prolonged with a four-tailed plantaris graft. This transfer is particularly powerful and intercepts the patient's pathological wrist flexion habit, converting it into a functional intrinsic grasp.

The Brand Transfers
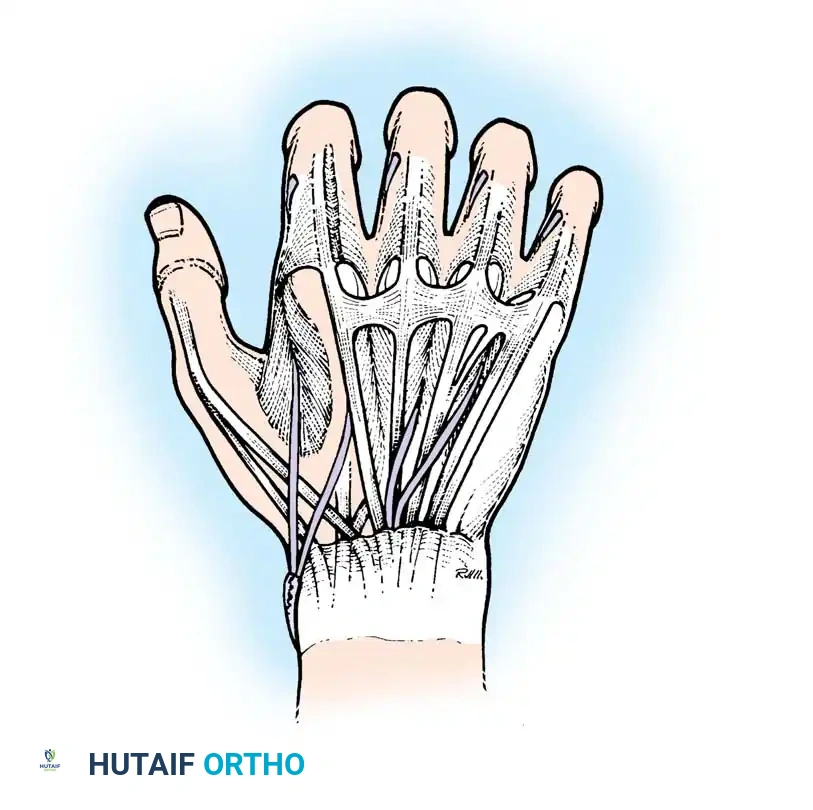
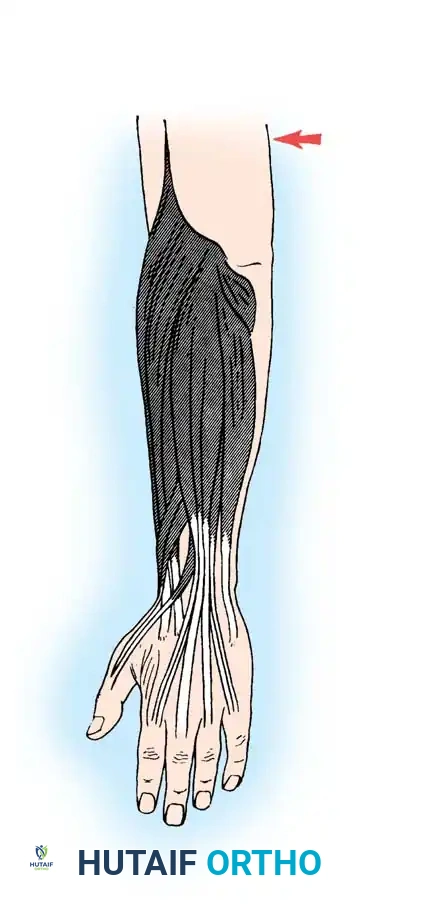
Paul Brand, drawing from his unparalleled experience treating thousands of Hansen's disease patients in India, developed highly reliable, standardized transfers using the wrist extensors. His preferred technique utilizes the extensor carpi radialis brevis (ECRB), which is detached from its insertion on the third metacarpal, withdrawn proximally, and lengthened by a free plantaris graft.
The free graft is split into four tails. Each tail is passed through the interosseous spaces, volar to the deep transverse metacarpal ligament. For the middle, ring, and little fingers, the slips are attached to the radial side of the extensor aponeurosis. However, for the index finger, Brand made a critical biomechanical observation: he advocated attaching the slip to the ulnar side of the index finger. Attaching the transfer to the ulnar lateral band places the index digit in adduction during pinch. This provides a much firmer and more stable platform against the thumb compared to radial attachment, which would promote unwanted abduction and pinch collapse.
Brand also described a variation where the ECRL or ECRB is transferred to the volar aspect of the forearm, extended by a four-tailed graft passed through the carpal tunnel, and routed through the lumbrical canals.
While this volar routing provides an excellent, direct line of pull for MCP flexion, it crowds the carpal tunnel. It carries a distinct risk of iatrogenic median nerve compression and should be used with extreme caution, or avoided entirely, if the median nerve is still functioning.
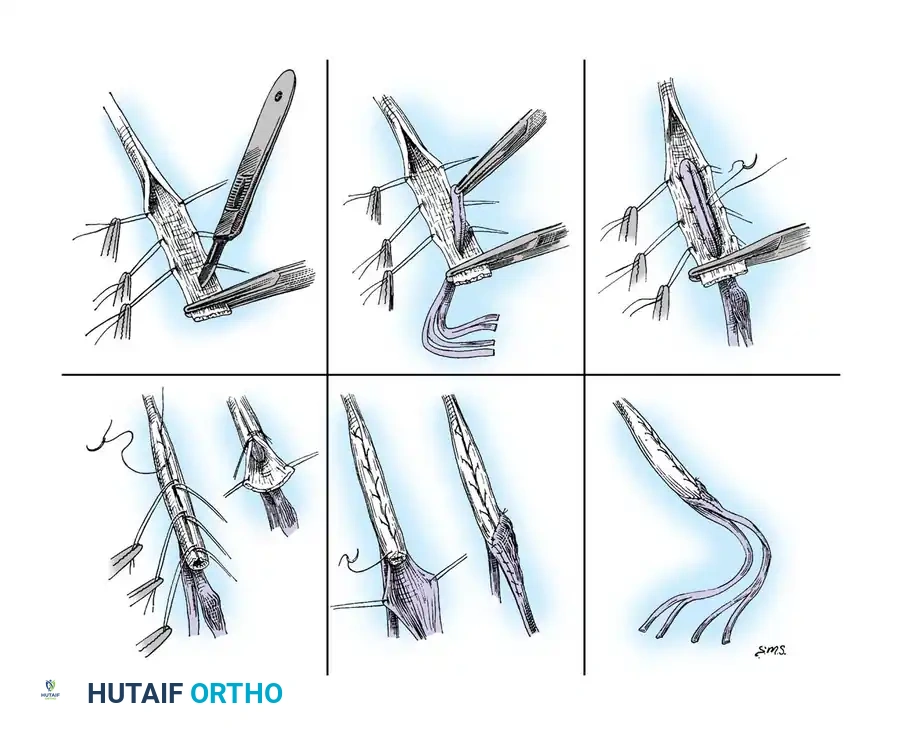
Advanced Tendon Routing and Graft Preparation
The ultimate success of any intrinsic tendon transfer relies heavily on the meticulous preparation of the tendon grafts and the precise anatomical routing of the slips. Tendon grafts must be handled with atraumatic technique to preserve the epitenon. The junctions between the donor motor and the free grafts must be woven smoothly, typically employing a Pulvertaft weave with 3-0 or 4-0 braided non-absorbable sutures, to prevent bulky adhesions and ensure seamless gliding.
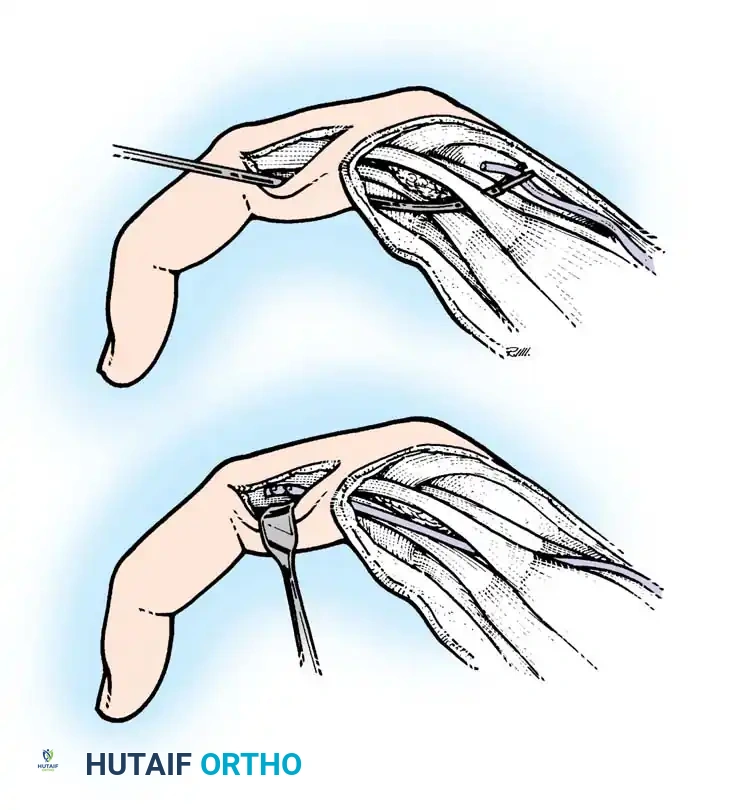
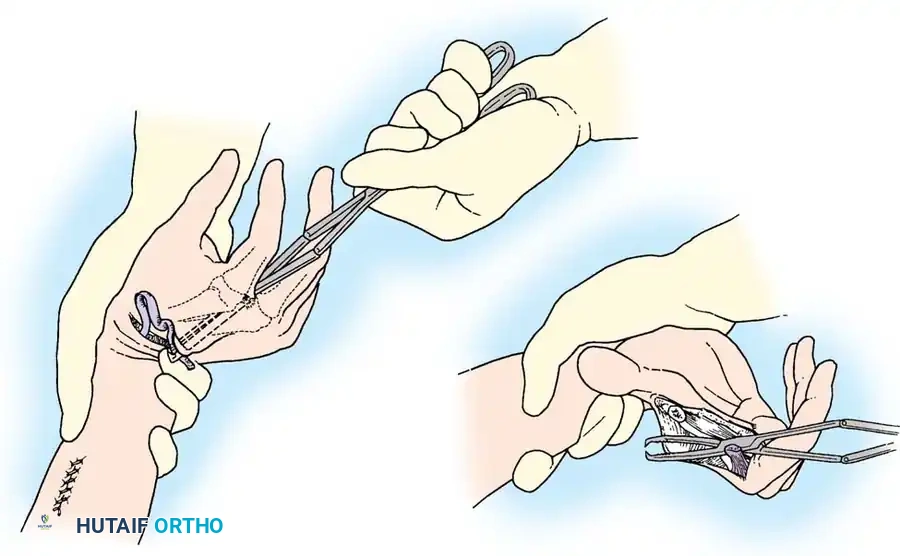
The routing pathways must strictly adhere to the volar aspect of the transverse metacarpal ligament. The surgeon uses a tendon passer or curved hemostat, introduced from the dorsal digital incision, passing volar to the ligament, to retrieve the graft slip from the palm.
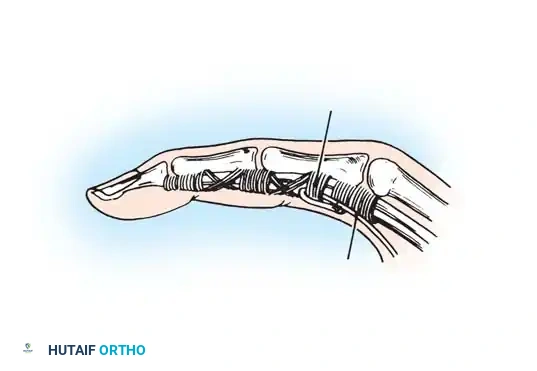
Tensioning the slips is the most artistic and critical phase of the operation. The wrist is placed in neutral, and the slips are tensioned such that the MCP joints are held in approximately 60 to 70 degrees of flexion, with the IP joints fully extended. The tension must recreate the normal resting cascade of the hand, where the index finger has the least flexion and the little finger has the most.
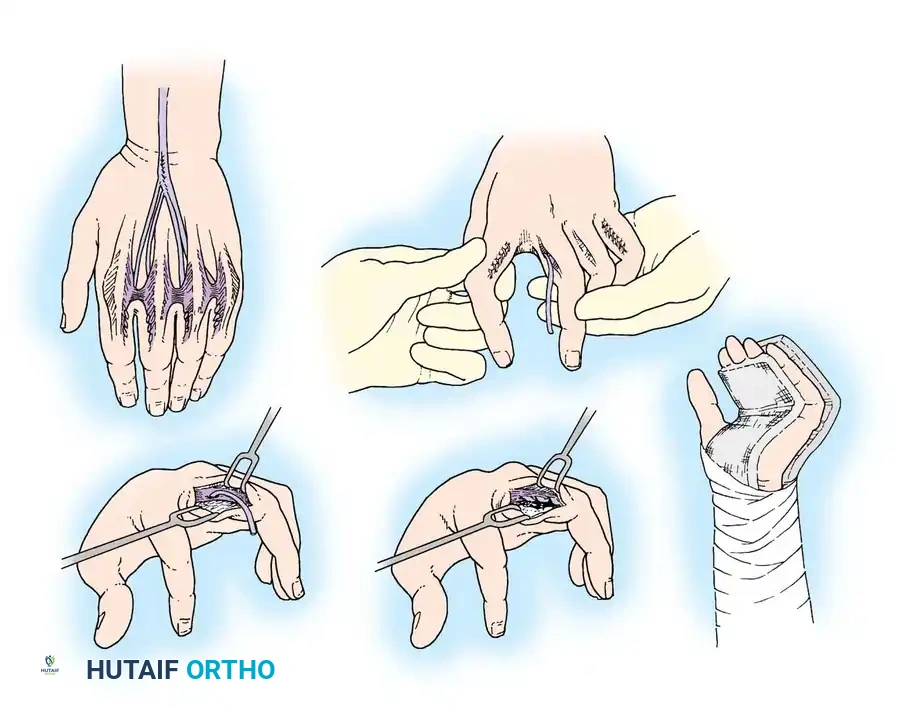
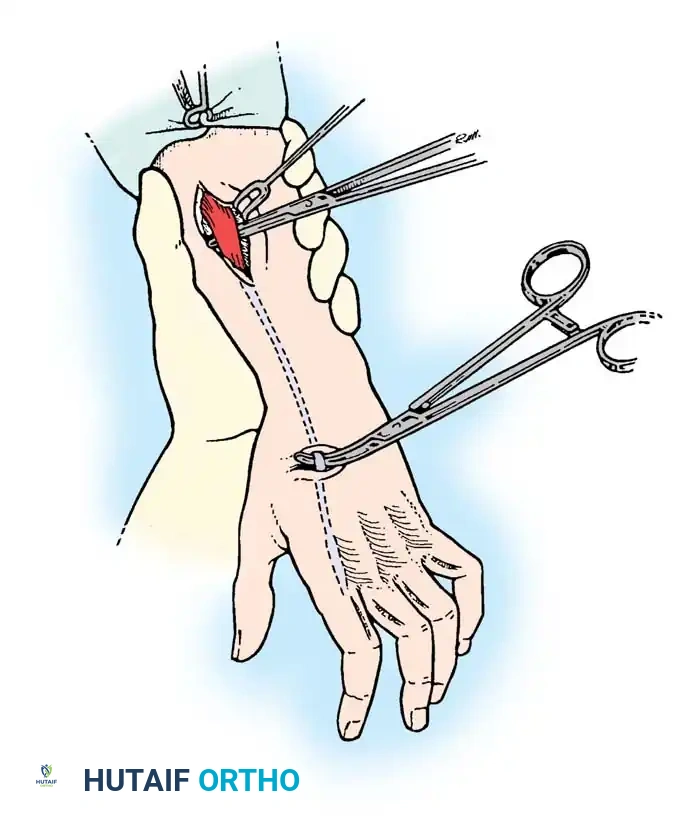
Associated Surgical & Radiographic Imaging
To further elucidate the complex spatial relationships and routing vectors, the following intraoperative diagrams and radiographic correlates are provided. These illustrate the critical passage of tendon slips through the interosseous spaces, ensuring they glide without impingement against the metacarpal heads or the transverse metacarpal ligament.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications in intrinsic tendon transfers can occur, largely due to the highly sensitive biomechanical balance of the extensor mechanism. The most dreaded complication is the iatrogenic intrinsic-plus deformity (swan-neck deformity), which occurs when the transfer is tensioned too tightly or a donor motor that is too powerful (such as an un-split FDS) is utilized. Conversely, under-tensioning or graft stretching leads to recurrent clawing.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Intrinsic-Plus Deformity | 5% - 15% | Avoid classic Bunnell in supple hands; precise intraoperative tensioning (wrist neutral, MCP 70° flex); use split grafts. | Lateral band mobilization; tenolysis; step-cut lengthening of the transfer |
