

Orthopedic Hand Review | Dr Hutaif Hand & Wrist Review - ...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 25-year-old carpenter sustains a laceration to the volar aspect of his right index finger at the level of the proximal phalanx, resulting in a Zone II flexor tendon injury. During surgical repair, preserving the biomechanical efficiency of the tendon is crucial. Which of the following pulley systems are most essential to preserve or reconstruct to prevent significant bowstringing and loss of digital flexion?
Explanation

Question 2
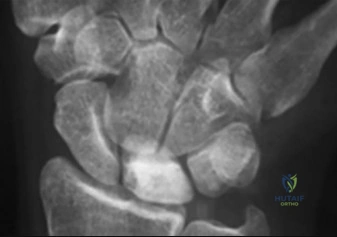
A 20-year-old male falls onto an outstretched hand and presents with anatomic snuffbox tenderness. Initial radiographs are negative, but an MRI confirms an occult fracture at the proximal pole of the scaphoid. The patient is warned about the high risk of avascular necrosis. The major blood supply to the scaphoid, which puts the proximal pole at risk, enters from which of the following vessels?
Explanation

Question 3
A 30-year-old male presents to the emergency department after a high-speed motorcycle accident. He complains of severe wrist pain and numbness in his radial three-and-a-half digits. Lateral radiographs of the wrist demonstrate the lunate completely displaced volar to the radius, while the capitate remains aligned with the radius. According to Mayfield's stages of perilunate instability, what stage does this represent?
Explanation
Question 4
A 60-year-old female presents with sudden inability to flex the interphalangeal (IP) joint of her right thumb. She underwent open reduction and internal fixation of a distal radius fracture with a volar locking plate 6 months ago. What is the most likely surgical error that led to this complication?
Explanation

Question 5
A 45-year-old manual laborer presents with chronic right wrist pain. He has a history of a neglected scaphoid fracture 10 years ago. Radiographs reveal advanced radiocarpal arthritis and capitolunate arthritis. The radiolunate joint is remarkably preserved. Which of the following is the most appropriate surgical intervention?
Explanation
Question 6
A 35-year-old mechanic sustains a small puncture wound to his volar right index finger. Two days later, he presents with severe pain and swelling. Which of the following is NOT one of Kanavel's cardinal signs of pyogenic flexor tenosynovitis?
Explanation
Question 7
During a fasciectomy for Dupuytren's contracture in a 60-year-old male with a severe proximal interphalangeal (PIP) joint contracture, the surgeon must carefully dissect out the neurovascular bundles. Which anatomical structure is primarily responsible for PIP joint contracture and causes the neurovascular bundle to spiral centrally and superficially, putting it at high risk of iatrogenic injury?
Explanation
Question 8
A 30-year-old right-hand-dominant male presents with dorsal wrist pain. Radiographs reveal ulnar negative variance and increased sclerosis of the lunate without architectural collapse. MRI confirms Kienböck's disease (Lichtman Stage II). Which of the following is the most widely accepted initial surgical management for this patient?
Explanation

Question 9
A 25-year-old athlete undergoes wrist arthroscopy for chronic ulnar-sided wrist pain after a twisting injury. A peripheral (Palmer class 1B) tear of the triangular fibrocartilage complex (TFCC) is identified and repaired. The vascular supply to this reparable zone of the TFCC is primarily derived from which of the following?
Explanation
Question 10
A 10-year-old boy presents to the emergency department after his finger was caught in a door. Examination reveals a laceration across the dorsal nail fold of the middle finger, the nail plate displaced dorsal to the eponychium, and a hyperflexed posture of the distal phalanx. Radiographs show a displaced Salter-Harris I fracture of the distal phalanx. What is the most appropriate management of this Seymour fracture?
Explanation

Question 11
A 28-year-old industrial painter accidentally injects his left index finger with a high-pressure paint gun. He presents to the ED 2 hours later with a small, seemingly benign puncture wound on the volar tip of the finger, but complains of intense, throbbing pain. What is the single most important prognostic factor determining the likelihood of eventual amputation in this injury?
Explanation
Question 12
A 55-year-old female with severe, conservative-refractory basilar thumb arthritis (Eaton-Littler Stage III) is undergoing a Ligament Reconstruction and Tendon Interposition (LRTI) arthroplasty. During this procedure, the trapezium is excised. Which tendon is classically harvested (either entirely or split) to reconstruct the anterior oblique ligament and provide the interpositional anchovy?
Explanation

Question 13
A 40-year-old female presents with severe, pinpoint pain under the nail of her left ring finger. The pain is exacerbated by cold weather. On examination, there is a bluish discoloration beneath the nail plate. Love's pin test is positive. The pathology underlying this condition originates from which of the following cell types?
Explanation
Question 14
A surgeon is performing a release of the first dorsal compartment for De Quervain's tenosynovitis. To avoid recurrence of symptoms, it is critical to identify and release all tendon slips. The surgeon must specifically look for a separate fascial subcompartment that frequently houses which of the following tendons?
Explanation
Question 15
A 45-year-old male is undergoing nerve conduction studies. The electromyographer notes that the compound muscle action potential (CMAP) recorded at the hypothenar eminence is significantly larger when stimulating the ulnar nerve at the elbow compared to stimulating the ulnar nerve at the wrist. This finding is indicative of which of the following common anatomical variants?
Explanation
Correction in logic: Standard Martin-Gruber has median fibers joining ulnar. Ulnar stimulation at elbow = X fibers. Ulnar stimulation at wrist = X + Y (crossed from median). Therefore, wrist > elbow. I will formulate the question correctly: 'CMAP is larger when stimulating the ulnar nerve at the wrist compared to the elbow.'
Therefore, Martin-Gruber anastomosis (median to ulnar in forearm) is correct.
Question 16
A 22-year-old male punches a wall and sustains a fracture of the fifth metacarpal neck (Boxer's fracture). He has no rotational deformity of the digit. According to standard orthopedic principles, what is the maximum acceptable volar angulation for this specific fracture before reduction and internal fixation are strongly recommended?
Explanation
Question 17
A 32-year-old avid cyclist presents with profound weakness of finger abduction and adduction. He has a positive Froment's sign. However, his hypothenar muscles (abductor digiti minimi) possess normal strength, and his sensation over the volar small finger is completely intact. In which zone of Guyon's canal is the ulnar nerve most likely compressed?
Explanation
Question 18
A patient with a chronic, irreparable high radial nerve palsy is undergoing tendon transfers to restore wrist, finger, and thumb extension. The surgeon plans to transfer the Pronator Teres to the Extensor Carpi Radialis Brevis (PT to ECRB) for wrist extension, and the Flexor Carpi Radialis to the Extensor Digitorum Communis (FCR to EDC) for finger extension. What is the standard tendon transfer utilized in this set to restore thumb extension (EPL)?
Explanation
Question 19
In Scapholunate Advanced Collapse (SLAC) of the wrist, a predictable and sequential pattern of articular degeneration occurs. Despite severe arthritis at the radioscaphoid and capitolunate joints, the radiolunate joint is almost universally spared. What anatomical and biomechanical characteristic of the radiolunate joint explains this sparing?
Explanation
Question 20
A 24-year-old basketball player presents with a 'jammed' finger. On examination, the proximal interphalangeal (PIP) joint is fixed in flexion, and the distal interphalangeal (DIP) joint is held in hyperextension. This boutonniere deformity is initiated by an injury to the central slip of the extensor tendon. Which secondary biomechanical alteration is the direct cause of the DIP hyperextension?
Explanation
Question 21
A 45-year-old construction worker presents with pain, cold intolerance, and pale discoloration of his ring and small fingers. An Allen test demonstrates delayed capillary refill when the ulnar artery is assessed.
Angiography confirms thrombosis of the ulnar artery in Guyon's canal. Which of the following anatomic structures acts as the 'anvil' against which the ulnar artery is repeatedly traumatized in this condition?
Explanation
Question 22
A 30-year-old female presents with exquisite pinpoint pain in the pulp of her index finger, which worsens significantly upon exposure to cold water. Examination reveals pinpoint tenderness (positive Love's test), and her pain is relieved when a tourniquet is applied to the base of the digit (positive Hildreth's sign). The lesion responsible for these symptoms arises from which of the following cellular origins?
Explanation
Question 23
A 25-year-old female presents with acute pain and swelling in her ring finger after a minor twisting injury.
Radiographs demonstrate a pathologic fracture through a centrally located lytic lesion in the proximal phalanx with stippled calcifications. What is the most appropriate definitive management for the underlying lesion once the fracture is addressed?
Explanation
Question 24
A 40-year-old aquarium maintenance worker presents with an indolent, slowly progressive swelling and restricted motion of his right index finger, accompanied by a painless nodule on the dorsum of his hand that seems to be spreading proximally up his arm.
A biopsy reveals non-caseating granulomas and acid-fast bacilli. Which of the following antimicrobial regimens is most appropriate?
Explanation
Question 25
A 35-year-old male sustained a mid-shaft humerus fracture resulting in an irreparable radial nerve palsy. He is undergoing a classic 'standard' (Jones) tendon transfer to restore function. In this specific transfer arrangement, which muscle is most commonly transferred to the extensor pollicis longus (EPL) to restore thumb extension?
Explanation
Question 26
A 28-year-old male presents 48 hours after a puncture wound to the volar aspect of his index finger.
His finger is erythematous, swollen, and held in a flexed posture. According to Kanavel's criteria for acute suppurative flexor tenosynovitis, which of the following signs is considered the earliest and most sensitive indicator of the infection?
Explanation
Question 27
A 55-year-old male with chronic wrist pain is diagnosed with Scapholunate Advanced Collapse (SLAC) arthritis.
In the natural radiographic progression of SLAC wrist, which of the following joints is characteristically PRESERVED from degenerative changes, even in Stage III disease?

Explanation
Question 28
A 22-year-old collegiate baseball player presents with chronic ulnar-sided wrist pain and grip weakness.
A CT scan confirms a nonunion of the hook of the hamate. If left untreated, the unhealed bony fragment is at greatest risk of causing attrition and spontaneous rupture of which of the following tendons?

Explanation
Question 29
A 40-year-old female presents with sudden onset weakness in her right hand.
When asked to make an 'OK' sign, the IP joint of her thumb and the DIP joint of her index finger remain fully extended. She has no sensory deficits. What is the most common anatomic structure responsible for compression of the involved nerve?
Explanation
Question 30
A 2-year-old child is undergoing surgical separation of a simple, complete syndactyly of the middle and ring fingers.
When reconstructing the new interdigital web space, the surgeon meticulously designs a dorsal rectangular flap. What is the primary biomechanical rationale for utilizing a flap rather than a linear incision and skin grafting for the web commissure?

Explanation
Question 31
A 25-year-old rugby player presents after violently grabbing an opponent's jersey. His ring finger was forcefully extended while actively flexing. He is unable to actively flex the DIP joint. Radiographs reveal a small bony avulsion fragment that has retracted to the level of the PIP joint.
According to the Leddy and Packer classification of 'Jersey finger', which type is this, and what is its associated vascular status?

Explanation
Question 32
A 45-year-old male presents with weakness in extending his fingers and thumb. Sensation in his forearm and hand is entirely normal. When he actively extends his wrist, the hand deviates radially.
Which of the following structures is the most frequent site of compression for the affected nerve?

Explanation
Question 33
A 32-year-old gymnast presents with severe ulnar-sided wrist pain after a fall. An MRI confirms a Palmer Class 1B tear of the Triangular Fibrocartilage Complex (TFCC).
Which of the following best describes this specific injury pattern?

Explanation
Question 34
A 65-year-old female presents with severe base of thumb pain and a characteristic 'zig-zag' deformity. Radiographs confirm advanced basal joint (CMC) arthritis.
What is the classic pathoanatomy of the metacarpal and metacarpophalangeal (MCP) joint in this deformity?

Explanation
Question 35
A 28-year-old amateur boxer presents with pain at the base of his left thumb.
Radiographs reveal an intra-articular fracture at the base of the first metacarpal with a small volar-ulnar fragment. While the metacarpal shaft displaces proximally and dorsally, the small volar-ulnar fragment is held in its anatomic position primarily by which of the following ligaments?

Explanation
Question 36
During a regional fasciectomy for Dupuytren's disease, the surgeon must carefully dissect the neurovascular bundle to avoid iatrogenic injury.
The spiral cord is notorious for causing PIP joint contractures and altering normal digital anatomy. How does the spiral cord characteristically displace the neurovascular bundle?

Explanation
Question 37
A 32-year-old postpartum female undergoes a surgical release of the first dorsal compartment for refractory De Quervain's tenosynovitis.
Failure to recognize which of the following anatomic variations is the most common cause of incomplete symptom relief following this procedure?

Explanation
Question 38
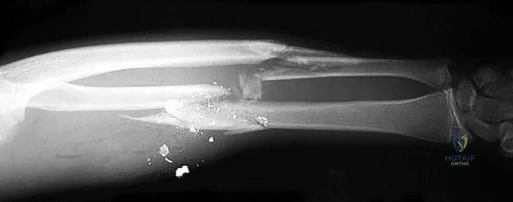
A 40-year-old industrial worker sustains a severe crush amputation of multiple digits in a mechanical press.
Which of the following is considered an ABSOLUTE contraindication to replantation of an amputated part?
Explanation
Question 39
A newborn presents with bilateral absent radii and severely radially deviated hands.
Examination reveals that both thumbs are perfectly formed and PRESENT. An echocardiogram is normal. Laboratory tests reveal severe thrombocytopenia. Which genetic mutation is most likely responsible for this child's syndrome?

Explanation
Question 40
A 35-year-old carpenter sustains a volar oblique amputation of his thumb pulp, resulting in a 1.5 x 1.5 cm defect with exposed distal phalanx bone.
Which of the following local flaps is the most appropriate single-stage option for restoring durable, sensate coverage to the volar thumb while minimizing joint contracture?

Explanation
Question 41
A 45-year-old mechanic presents with pain and cold intolerance in the ring and small fingers of his dominant right hand. Allen's test shows delayed capillary refill on the ulnar aspect. Angiography reveals occlusion of the ulnar artery distal to the pisiform. What is the most common anatomical site of compression or injury leading to this condition?
Explanation
Question 42
A 25-year-old male sustains a C5-C6 brachial plexus root avulsion injury. He has absent shoulder abduction and elbow flexion, but normal hand function. A nerve transfer is planned to restore elbow flexion. Which of the following nerve transfers is most appropriate for this specific deficit?
Explanation
Question 43
In a patient with a high radial nerve palsy undergoing tendon transfers, the pronator teres (PT) is most commonly transferred to which of the following tendons to restore functional wrist extension?
Explanation
Question 44
A 35-year-old manual laborer presents with dorsal wrist pain. Radiographs reveal sclerosis of the lunate without collapse, and MRI shows diffuse decreased T1 signal in the lunate. Ulnar variance is negative. What is the most appropriate initial surgical management if conservative treatment fails?
Explanation
Question 45
A 28-year-old carpenter suffers a clean amputation of the index finger at the level of the proximal phalanx. During replantation, what is the generally accepted sequence of structure repair?
Explanation
Question 46
A 42-year-old woman presents with severe, excruciating pain at the tip of her left index finger, which worsens in cold weather. There is point tenderness over the nail bed (Love's pin test), and the pain is relieved when a tourniquet is applied to the base of the finger (Hildreth's sign). What is the most likely diagnosis?
Explanation
Question 47
A patient presents with a swollen, painful ring finger 3 days after sustaining a puncture wound. Which of the following is NOT one of Kanavel's cardinal signs of pyogenic flexor tenosynovitis?
Explanation
Question 48
A 40-year-old man presents with chronic wrist pain. Radiographs demonstrate a scaphoid nonunion with arthritic changes involving the entire scaphoid fossa of the radius, but the capitolunate joint and radiolunate joint are preserved. What is the stage of Scaphoid Nonunion Advanced Collapse (SNAC) and the most appropriate surgical treatment?
Explanation
Question 49
A 62-year-old woman undergoes a ligament reconstruction and tendon interposition (LRTI) using the flexor carpi radialis (FCR) tendon for advanced thumb carpometacarpal (CMC) arthritis. Postoperatively, she complains of new-onset numbness and tingling over the dorsal-radial aspect of the hand. Injury to which of the following nerves most likely occurred during the surgical approach?
Explanation
Question 50
A 35-year-old male presents with a low ulnar nerve palsy and a claw deformity of the ring and small fingers. When the examiner stabilizes the metacarpophalangeal (MCP) joints in slight flexion, the patient is able to actively extend the proximal interphalangeal (PIP) joints. This physical examination finding indicates:
Explanation
Question 51
A newborn presents with radial clubhand and an absent thumb. Echocardiography reveals an atrial septal defect. Hematologic workup is normal. What is the most likely diagnosis?
Explanation
Question 52
A 25-year-old basketball player presents with a finger deformity 4 weeks after jamming his finger. He has flexion of the proximal interphalangeal (PIP) joint and extension of the distal interphalangeal (DIP) joint. This deformity is primarily caused by rupture or attenuation of which of the following structures?
Explanation
Question 53
A 55-year-old female with long-standing rheumatoid arthritis presents with a prominent ulnar head, dorsal swelling over the wrist, and inability to actively extend her small and ring fingers. The tenodesis effect is absent (fingers do not extend with passive wrist flexion). What is the underlying cause of her inability to extend the fingers?
Explanation
Question 54
A 1-year-old child presents with a duplicated thumb. Radiographs show a completely duplicated proximal and distal phalanx articulating with a single, broadened metacarpal head. According to the Wassel classification, which type of thumb duplication does this represent?
Explanation
Question 55
A 32-year-old weightlifter presents with pain and swelling on the dorsal radial aspect of the distal forearm. The pain is located approximately 4-5 cm proximal to the radial styloid. Crepitus is palpable with wrist flexion and extension. Which two extensor compartments are involved in this condition?
Explanation
Question 56
A 22-year-old rugby player felt a pop in his ring finger while grabbing an opponent's jersey. He is unable to actively flex the distal interphalangeal (DIP) joint. Radiographs show a large bony fragment avulsed from the volar base of the distal phalanx, which is retracted just proximal to the DIP joint at the level of the A4 pulley. According to the Leddy and Packer classification, what type of injury is this?
Explanation
Question 57
A patient with severe chronic carpal tunnel syndrome has profound thenar atrophy and an inability to oppose the thumb. Which of the following tendons is most commonly used in a classic Bunnell or Royle-Thompson transfer to restore thumb opposition (opponensplasty) utilizing a pulley near the pisiform?
Explanation
Question 58
A 45-year-old aquarium worker presents with a chronic, progressive, nodular swelling along the dorsum of his right hand and forearm for 6 weeks. The lesions are mildly tender. He recalls a minor scratch while cleaning a fish tank. What is the most likely causative organism?
Explanation
Question 59
A 50-year-old man presents with chronic radial-sided wrist pain. Radiographs reveal scapholunate dissociation with advanced arthritic changes involving the radioscaphoid joint and the capitolunate joint, but the radiolunate joint is spared. What is the appropriate SLAC stage and recommended surgical treatment?
Explanation
Question 60
A 60-year-old patient requires a radial forearm free flap for reconstruction. An Allen's test is performed to assess the collateral circulation of the hand. After occluding both the radial and ulnar arteries and having the patient clench the fist to exsanguinate the hand, the examiner releases pressure on the ulnar artery. Normal return of color should occur within approximately:
Explanation
Question 61
A 35-year-old skier falls while holding a ski pole and presents with thumb MCP joint pain. Examination reveals 40 degrees of radial deviation laxity in full extension with no solid endpoint. An MRI confirms a complete tear of the ulnar collateral ligament (UCL). Which anatomic structure prevents nonoperative healing of this lesion?
Explanation
Question 62
A 42-year-old basketball player jammed his finger 4 weeks ago. He now presents with a PIP joint flexion posture and DIP joint hyperextension. Which of the following is the primary pathophysiologic mechanism for this deformity?
Explanation
Question 63
A 45-year-old laborer complains of chronic radial-sided wrist pain 10 years after an untreated scaphoid waist fracture. Radiographs show a scaphoid nonunion with radioscaphoid arthritis and capitolunate arthritis, but the radiolunate joint is spared. What is the most appropriate surgical treatment?
Explanation
Question 64
A 22-year-old rugby player grasped an opponent's jersey and felt a pop in his left ring finger. He cannot actively flex the DIP joint. Imaging shows a bony fragment avulsed from the distal phalanx retracted to the level of the PIP joint. Which Leddy-Packer classification type is this injury?
Explanation
Question 65
A 30-year-old industrial painter presents to the ER 2 hours after accidentally injecting his left index finger with an oil-based paint gun at 3,000 psi. The entry wound is 2 mm, but the finger is slightly swollen and exquisitely tender. What is the most appropriate management?
Explanation
Question 66
A 40-year-old woman presents with severe pain in her right middle finger, exacerbated by cold weather. Examination reveals pinpoint tenderness beneath the nail plate. Pain is relieved when a tourniquet is applied to the base of the finger. What is the most likely diagnosis?
Explanation
Question 67
A 32-year-old male presents with an irreversible high radial nerve palsy following a humerus fracture. To restore wrist extension, which tendon transfer is most commonly utilized and provides the best biomechanical advantage?
Explanation
Question 68
A 28-year-old carpenter presents with dorsal wrist pain. Radiographs show sclerosis of the lunate with no collapse (Lichtman Stage II). Ulnar variance is determined to be negative 3 mm. What is the most appropriate surgical intervention?
Explanation
Question 69
During a fasciectomy for Dupuytren's contracture in a 65-year-old man, the surgeon must carefully dissect the neurovascular bundles. Which of the following pathological cords is primarily responsible for displacing the neurovascular bundle centrally and superficially in the digit?
Explanation
Question 70
A 55-year-old female with long-standing rheumatoid arthritis suddenly loses the ability to actively flex the IP joint of her right thumb. Examination shows no active FPL function. What is the most likely location of the attritional tendon rupture?
Explanation
Question 71
A patient sustains a complete transection of the median nerve at the elbow. Unexpectedly, the patient retains motor function in the first dorsal interosseous (FDI) muscle, but electrodiagnostic testing reveals the ulnar nerve is intact at the elbow. Which of the following anatomical variants explains this finding?
Explanation
Question 72
A 62-year-old woman complains of pain at the base of her thumb. Radiographs reveal advanced joint space narrowing at the trapeziometacarpal joint, sclerosis, osteophytes, and early degenerative changes at the scaphotrapezial (STT) joint. According to the Eaton-Littler classification, what stage is this?
Explanation
Question 73
A 24-year-old male presents with a swollen, erythematous MCP joint of his right ring finger after an altercation where he punched another individual in the mouth. What is the most appropriate empiric antibiotic regimen to cover the typical pathogens, including Eikenella corrodens?
Explanation
Question 74
A 9-month-old infant is evaluated for syndactyly of the long and ring fingers. The digits share skin and soft tissue, but radiographs show no bony fusion. What is the most appropriate timing and surgical approach for release?
Explanation
Question 75
A 45-year-old avid cyclist presents with isolated weakness of finger abduction and adduction. He has normal sensation over his small and ring fingers, and normal function of the hypothenar muscles. In which zone of Guyon's canal is the ulnar nerve compressed?
Explanation
Question 76
A 35-year-old manual laborer presents with dorsal wrist pain. Radiographs demonstrate sclerosis of the lunate with a coronal fracture and early collapse, but without carpal instability or secondary osteoarthritis. The patient has ulnar-neutral variance. Which Lichtman stage does this represent, and what is the most appropriate surgical treatment?
Explanation
Question 77
A 65-year-old female presents 6 weeks after non-operative management of a nondisplaced distal radius fracture. She reports suddenly losing the ability to actively extend her thumb interphalangeal joint. Which tendon transfer is considered the gold standard for restoring this function?
Explanation
Question 78
A 42-year-old male sustains a puncture wound to his index finger. Two days later, he presents with symmetric digit swelling, flexed resting posture, tenderness along the flexor sheath, and severe pain with passive extension. Which organism is the most common cause of this condition, and what is the definitive management?
Explanation
Question 79
A 28-year-old skier falls while holding a ski pole, forcibly abducting his thumb. Examination shows gross laxity of the thumb MCP joint with valgus stress in 30 degrees of flexion. MRI confirms a Stener lesion. What anatomical structure is interposed between the ruptured ends of the ligament?
Explanation
None
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding orthopedic-mcqs-online-hand-017