Masterclass in Tendon Transfers for Thumb Intrinsic Dysfunction: Modified Royle-Thompson and EIP Techniques
Key Takeaway
The modified Royle-Thompson transfer utilizes the ring finger flexor digitorum superficialis to restore thumb adduction and opposition in intrinsic paralysis. By splitting the tendon and routing it to the extensor pollicis longus and adductor pollicis, surgeons can recreate a dynamic pinch. This guide details the biomechanics, step-by-step surgical technique, and postoperative rehabilitation for the Royle-Thompson, extensor indicis proprius, and abductor pollicis longus tendon transfers.
Comprehensive Introduction and Patho-Epidemiology
The human thumb represents the evolutionary pinnacle of prehensile function, relying on a delicate, highly coordinated balance between extrinsic and intrinsic musculature to achieve circumduction, opposition, and powerful key pinch. In the setting of peripheral nerve injuries—specifically ulnar nerve palsy, low median nerve palsy, or combined lesions—the loss of intrinsic muscle function results in profound and debilitating functional impairment. The adductor pollicis, the first dorsal interosseous (FDI), and the opponens pollicis are the primary intrinsic effectors that stabilize the first ray during power grip and precision handling. When these muscles are paralyzed, the complex biomechanical vectors required for a stable pinch are obliterated, leading to characteristic compensatory deformities that orthopedic surgeons must meticulously diagnose and reconstruct.
Patients with intrinsic paralysis typically present with a dramatically weakened key pinch and grip strength, often reduced by up to 70% compared to the contralateral uninjured extremity. Clinically, this manifests as compensatory interphalangeal (IP) joint hyperflexion driven by the unopposed flexor pollicis longus (Froment’s sign), and metacarpophalangeal (MCP) joint hyperextension (Jeanne’s sign). Furthermore, the loss of the first dorsal interosseous allows the index finger to drift ulnarly under the pressure of the thumb during pinch maneuvers, a phenomenon that severely compromises the rigid post required for effective prehension. The patho-epidemiology of these deficits spans traumatic lacerations, severe traction neuropathies, advanced compressive syndromes (such as severe cubital tunnel syndrome), and neurodegenerative disorders. Regardless of the etiology, once the window for primary nerve repair or nerve transfer has closed—typically after 12 to 18 months of denervation—the motor endplates undergo irreversible fibrosis, necessitating structural tendon transfers.
To restore the complex biomechanical vectors required for a stable pinch, orthopedic surgeons employ highly specific tendon transfers designed to replicate the lost moment arms. The modified Royle-Thompson transfer and the Extensor Indicis Proprius (EIP) transfer remain the cornerstone procedures for re-establishing the adduction moment arm of the thumb and stabilizing the index finger against the thumb. Originally described in the early 20th century, the Royle-Thompson procedure has undergone significant evolution. The modern modified technique, heavily influenced by the work of Riordan and Brand, utilizes the flexor digitorum superficialis (FDS) of the ring finger to simultaneously address adduction loss and MCP hyperextension.
It is a fundamental axiom of orthopedic reconstructive surgery that tendon transfers do not create new strength; rather, they redistribute existing power at a mechanical cost. A transferred muscle will typically lose at least one grade of motor strength on the Medical Research Council (MRC) scale following transposition due to alterations in its native length-tension relationship and the friction of new anatomical routing. Therefore, only muscles with a robust preoperative strength of Grade 4 or 5 should be selected as donors. The ultimate goal of this masterclass is to provide the practicing orthopedic surgeon with an exhaustive, biomechanically sound framework for executing these complex transfers, ensuring optimal restoration of pinch kinematics and patient independence.
Detailed Surgical Anatomy and Biomechanics
Mastery of tendon transfer surgery requires an intimate, three-dimensional understanding of hand biomechanics and the specific anatomical vectors of both the paralyzed muscles and the proposed donor units. The adductor pollicis is a massive, bipennate intrinsic muscle comprising an oblique head (originating from the capitate and the bases of the second and third metacarpals) and a transverse head (originating from the palmar shaft of the third metacarpal). These heads converge to insert on the ulnar base of the thumb proximal phalanx and the ulnar sesamoid, effectively pulling the first metacarpal toward the palm while flexing the MCP joint. This dual action—adduction and MCP flexion—is critical for stabilizing the first ray against the counter-pressure of the index finger during key pinch.
The first dorsal interosseous (FDI) is equally critical to the pinch mechanism. Originating from the adjacent shafts of the first and second metacarpals, the FDI inserts into the radial base of the index proximal phalanx and the extensor expansion. Its primary biomechanical role is to powerfully abduct the index finger and flex its MCP joint, providing an unyielding, rigid post against which the thumb can exert force. When the ulnar nerve is compromised, the FDI is paralyzed, and the index finger succumbs to the ulnar-directed force of the thumb. The extrinsic flexors (FDP and FDS) attempt to compensate, but without the intrinsic stabilization of the MCP joint, the digit collapses into an ineffective, unstable posture.
Understanding the Blix length-tension curve is paramount when selecting and tensioning donor muscles. A muscle generates its maximum active tension at its resting physiological length. If a transferred tendon is sutured with excessive tension, the sarcomeres are stretched beyond their optimal cross-bridge overlap, resulting in a weak, contracted transfer. Conversely, if sutured too loosely, the muscle expends its entire excursion merely taking up the slack, failing to transmit force to the skeletal insertion. The flexor digitorum superficialis (FDS) of the ring finger is an ideal donor for the modified Royle-Thompson transfer because its native excursion (approximately 50 mm) far exceeds the 30 mm required for thumb adduction, and its robust cross-sectional area provides excellent force generation.
The Extensor Indicis Proprius (EIP) is the gold standard donor for restoring FDI function. The EIP possesses an excursion of approximately 40 to 50 mm and an appropriate line of pull when routed volarly to the transverse metacarpal ligament. Its harvest leaves the index finger with independent extension via the extensor digitorum communis (EDC), provided the extensor hood is meticulously repaired. Biomechanically, routing the EIP across the first web space to the radial aspect of the index finger perfectly replicates the vector of the paralyzed FDI. When the EIP is unavailable, the Abductor Pollicis Longus (APL) offers a powerful alternative. The APL frequently possesses multiple accessory slips inserting into the trapezium or thenar fascia. Utilizing these slips, combined with a palmaris longus graft, provides a robust, synergistic vector that does not compromise primary thumb abduction, facilitating rapid cortical re-education since the APL is already a native thumb motor.
Exhaustive Indications and Contraindications
The decision to proceed with a tendon transfer for thumb intrinsic dysfunction is complex and must be strictly governed by established physiological and biomechanical prerequisites. Tendon transfers are indicated only when irreversible intrinsic paralysis has been confirmed, typically after a minimum of 12 to 18 months following a severe peripheral nerve injury, or immediately in cases where primary nerve repair or grafting is deemed anatomically impossible. The patient must present with a profound loss of key pinch strength, severe fatigue with manual tasks, and the classic compensatory deformities (Froment’s and Jeanne’s signs) that interfere with activities of daily living. Furthermore, the patient must have a clear understanding of the surgical goals, acknowledging that the procedure is designed to restore functional stability and pinch strength, not normal anatomical perfection.
Before any surgical intervention is considered, the recipient joints must be completely supple. The principle of "soft tissue equilibrium" dictates that a tendon transfer cannot overcome a fixed joint contracture. If the thumb web space is contracted, or if the thumb MCP or IP joints lack full passive range of motion, a preliminary soft tissue release or serial casting protocol must be executed prior to the transfer. Additionally, the selected donor muscle must possess a minimum MRC grade of 4 (preferably 5), as the transfer process inherently diminishes the muscle's contractile force by at least one grade. The donor must also have adequate excursion to replicate the lost function and, ideally, act synergistically with the intended movement to facilitate postoperative cortical re-education.
Contraindications to these tendon transfers are absolute and must be respected to prevent catastrophic surgical failures. Severe, unyielding joint stiffness or fixed contractures of the first web space are absolute contraindications; transferring a tendon into a stiff joint will only result in a tethered, non-functional digit. Advanced degenerative joint disease (DJD) of the thumb MCP or carpometacarpal (CMC) joints precludes isolated soft tissue transfers, as the skeletal foundation is inherently unstable and painful; such cases require primary arthrodesis. Cognitive impairment, severe psychiatric illness, or a documented history of non-compliance with rehabilitation protocols are also strict contraindications, as the success of a tendon transfer is entirely dependent on meticulous, phased postoperative hand therapy.
| Parameter | Indications for Tendon Transfer | Absolute Contraindications |
|---|---|---|
| Neurologic Status | Irreversible ulnar/median nerve palsy (>12-18 months) | Recovering nerve lesion; progressive untreatable neuropathy |
| Joint Mobility | Full, supple passive range of motion in all involved joints | Fixed contractures; severe first web space adduction contracture |
| Donor Muscle | MRC Grade 4 or 5 strength; adequate excursion; synergistic | MRC Grade < 4; previously traumatized or denervated donor |
| Skeletal Stability | Stable thumb MCP and CMC joints without severe arthritis | Advanced degenerative joint disease; global skeletal instability |
| Patient Factors | Compliant, motivated, cognitively intact, realistic expectations | Non-compliant, severe cognitive deficits, active local infection |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for the modified Royle-Thompson and EIP tendon transfers begins with an exhaustive clinical examination. The surgeon must meticulously document the active and passive range of motion of the thumb and index finger, utilizing a goniometer to quantify any deficits. The MRC grading of all potential donor muscles—specifically the FDS of the ring finger, the EIP, and the APL—must be recorded. A thorough assessment of the first web space is critical; if the angle of maximum passive radial abduction is less than 40 degrees, a preliminary Z-plasty or first dorsal interosseous fascia release may be required either prior to or concomitantly with the tendon transfer. Radiographic evaluation, including AP, lateral, and Robert's views of the thumb, is mandatory to rule out underlying degenerative joint disease or occult skeletal instability that would necessitate an arthrodesis.
Templating the surgical vectors is a critical cognitive exercise for the operating surgeon. For the modified Royle-Thompson transfer, the surgeon must visualize the pathway from the distal palmar crease, deep to the palmar fascia, and across the palm to the adductor insertion and the EPL tendon. The tunnel must be perfectly straight to avoid the "pulley effect," which diminishes the effective tension and excursion of the transfer. Similarly, for the EIP transfer, the surgeon must plan the subcutaneous routing over the dorsum of the hand to ensure a sweeping, frictionless curve that avoids acute angles. Patient education regarding the anticipated postoperative immobilization and the rigorous rehabilitation timeline is also a mandatory component of the preoperative phase.
On the day of surgery, anesthesia is typically achieved via a regional block—such as an axillary or supraclavicular brachial plexus block—combined with intravenous sedation. This approach provides excellent intraoperative muscle relaxation and profound postoperative analgesia, minimizing the need for systemic opioids. General anesthesia is reserved for patients with contraindications to regional blockade or extreme anxiety. The patient is positioned supine with the operative arm extended onto a radiolucent hand table. A well-padded pneumatic upper arm tourniquet is applied to the proximal brachium.
Following standard surgical preparation and draping from the fingertips to the mid-arm, the limb is exsanguinated using an Esmarch bandage, and the tourniquet is inflated to 250 mm Hg (or exactly 100 mm Hg above the patient's documented systolic blood pressure). The surgeon must note the exact time of tourniquet inflation, as the maximum safe ischemic time is generally considered to be 120 minutes. If the procedure extends beyond this limit, the tourniquet must be deflated for 15 to 20 minutes to allow for reperfusion before re-inflation. Prior to the first incision, a surgical time-out is performed to confirm patient identity, the correct operative extremity, and the specific tendon transfers to be executed.
Step-by-Step Surgical Approach and Fixation Technique
The Modified Royle-Thompson Transfer (FDS Harvest and Routing)
The original Royle-Thompson transfer was designed solely to restore thumb opposition. The modern modified technique, however, utilizes the flexor digitorum superficialis (FDS) of the ring finger to address both the adduction deficit and the MCP hyperextension characteristic of Jeanne's sign. The procedure begins with a midlateral incision over the ulnar aspect of the ring finger. This specific approach is chosen to avoid the volar tactile surface, thereby minimizing the risk of painful neuromas and postoperative flexion contractures. The surgeon carefully dissects through the subcutaneous tissue to expose the flexor tendon sheath. The sheath is incised, with absolute care taken to preserve the critical A2 and A4 pulleys; violation of these pulleys will lead to catastrophic postoperative bowstringing of the remaining flexor digitorum profundus (FDP) tendon.
Once the FDS tendon is identified, its insertion on the middle phalanx is freed. The FDS bifurcates at Camper's chiasm; the surgeon must ensure both slips of the insertion are sharply and cleanly detached. Next, a short transverse incision is made in the mid-palm, precisely following the distal palmar crease to ensure a cosmetically acceptable scar and avoid crossing flexion creases at a right angle. The FDS tendon of the ring finger is identified within the palmar wound. Gentle traction is applied to the distal stump in the finger, and the tendon is withdrawn proximally out of the palm. Using a fresh #15 scalpel blade, the harvested FDS tendon is meticulously split longitudinally into two equal slips along its entire length.
A curved incision is then made on the dorsoradial aspect of the thumb, similar to the approach described for a Riordan transfer. This incision must allow adequate, unimpeded exposure of the extensor pollicis longus (EPL) tendon and the tendinous insertion of the adductor pollicis. The surgeon creates a wide, generous subcutaneous tunnel from the palmar incision to the dorsoradial thumb incision using blunt dissection. It is a critical surgical warning that this tunnel must be strictly subcutaneous and wide enough to allow frictionless gliding of the transferred tendon. Constriction within the tunnel is a primary cause of transfer failure. Both slips of the split FDS tendon are passed radially through this tunnel. Slip 1 is sutured to the EPL tendon distal to the MCP joint to act as a dynamic tenodesis, preventing hyperextension. Slip 2 is tunneled dorsally over the first metacarpal and sutured securely to the adductor pollicis insertion. Tension is set with the wrist in neutral, the thumb in full adduction, and the MCP joint in slight flexion, utilizing a Pulvertaft weave with 3-0 non-absorbable braided suture.
Transfer of the Extensor Indicis Proprius (EIP) Tendon
Restoring thumb adduction is insufficient if the index finger cannot provide a stable, rigid post against which the thumb can pinch. The EIP transfer is the gold standard for restoring the function of the paralyzed first dorsal interosseous (FDI). The procedure begins with a curved incision starting at the midlateral point on the radial side of the index finger proximal phalanx, carrying proximally over the radial aspect of the MCP joint, and curving dorsally to end at the middle of the second metacarpal. The EIP tendon is identified over the dorsum of the hand; it is consistently located ulnar and deep to the extensor digitorum communis (EDC) tendon of the index finger.
To add critical length to the EIP tendon, the surgeon elevates a small, rectangular flap of the dorsal extensor expansion over the MCP joint where it attaches to the insertion of the tendon. The tendon is then withdrawn proximally into the dorsal wound. A crucial step at this juncture is the meticulous closure of the resulting defect in the extensor expansion using 4-0 absorbable sutures. Failure to perform this repair will inevitably result in a postoperative extensor lag or ulnar subluxation of the remaining EDC tendon. The EIP tendon is then freed throughout the proximal wound to ensure completely unrestricted excursion.
The tendon is passed radially in a gentle, sweeping subcutaneous curve toward the base of the index finger. The tendinous insertion of the paralyzed FDI muscle is identified and its surface is deliberately roughened with a scalpel to promote robust biological healing. The transferred EIP tendon is securely sutured to the FDI tendon using a standard weave technique. Tensioning is performed with the index finger held in full radial abduction and slight MCP flexion. The surgeon must ensure that the tension is tight enough to hold the digit in abduction against gravity, but not so tight as to create a fixed abduction contracture.
Abductor Pollicis Longus (APL) Transfer (Neviaser Technique)
When the EIP is unavailable—due to prior trauma, previous transfer, or anatomical absence—the Abductor Pollicis Longus (APL) transfer serves as an excellent, powerful alternative for restoring FDI function. The APL frequently possesses multiple accessory slips inserting into the trapezium or thenar fascia, making it an ideal donor that does not compromise primary thumb abduction. The biomechanical advantage of the APL transfer is its robust vector that closely mimics the native FDI. Furthermore, because the APL is already a native thumb motor, cortical re-education for pinch is often significantly faster than with an EIP transfer.
Step 1: Harvesting the Accessory Slip
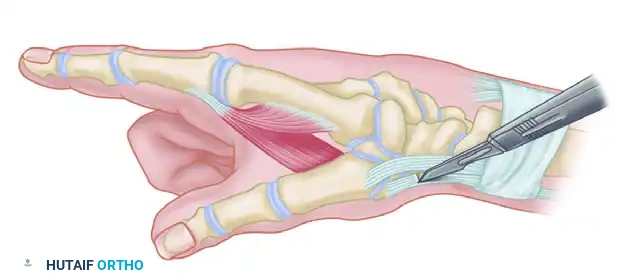
The surgeon identifies the first dorsal compartment over the radial styloid. The compartment is opened, and the multiple slips of the APL are identified. The primary functional slip inserting into the base of the first metacarpal is carefully preserved. The accessory slip inserting into the trapezium is sharply detached distal to the extensor retinaculum.
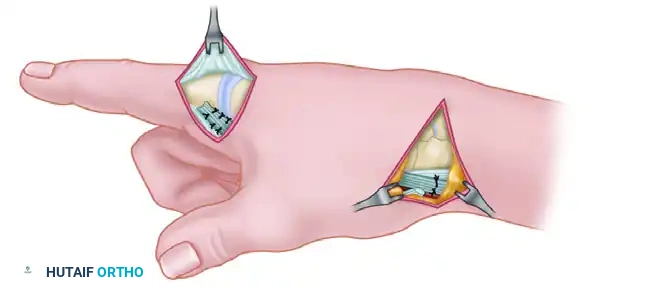
Figure A: The accessory slip inserting into the trapezium is sharply detached distal to the extensor retinaculum. The primary functional slip, inserting into the first metacarpal, is carefully preserved to maintain native thumb abduction.
Step 2: Tunnel Creation
Once the accessory slip is mobilized, a direct pathway must be created to redirect its line of pull toward the index finger. Utilizing blunt dissecting scissors, a wide subcutaneous tunnel is formed.
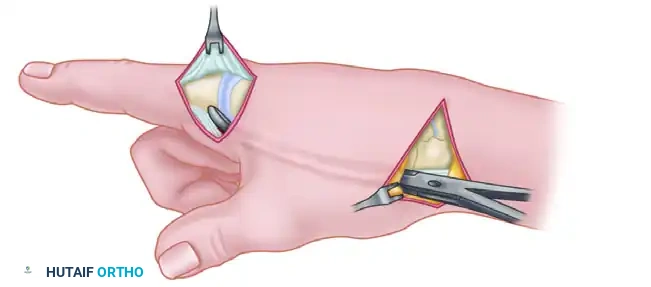
Figure B: A wide subcutaneous tunnel is created using blunt dissection from the radial styloid across the first web space to the tendinous insertion of the first dorsal interosseous on the radial aspect of the index finger.
Step 3: Grafting and Fixation
Because the accessory slip of the APL is almost always too short to reach the FDI insertion directly, a free tendon graft is required to bridge the anatomical defect. The palmaris longus is the standard graft of choice.
Figure C: The free tendon graft is meticulously woven into the native tendon of the first dorsal interosseous distally, passed through the subcutaneous tunnel, and sutured to the mobilized accessory slip of the APL proximally under appropriate tension.
Management of the Unstable Thumb Metacarpophalangeal Joint
Tendon transfers inherently rely on stable skeletal foundations to transmit force effectively. If the thumb metacarpophalangeal joint exhibits global instability, a fixed hyperextension deformity greater than 30 degrees, or advanced degenerative joint disease, soft tissue transfers alone will unequivocally fail to provide a powerful pinch. The transferred forces will simply dissipate through the unstable joint, exacerbating the deformity rather than restoring function. In these specific scenarios, arthrodesis of the thumb MCP joint is strictly indicated and must be performed concomitantly with, or prior to, the tendon transfers.
Fusion of the thumb MCP joint is typically performed utilizing a dorsal approach. The articular cartilage is meticulously denuded using a combination of rongeurs and a high-speed burr, ensuring exposing of healthy, bleeding subchondral bone. The joint is then positioned in the functional posture: 10 to 15 degrees of flexion, slight pronation to face the index finger, and neutral abduction/adduction. Fixation is achieved using crossed K-wires, a tension band construct, or a dedicated low-profile compression plate, depending on surgeon preference and bone quality.
A critical surgical pearl in this scenario involves the extensor pollicis brevis (EPB) tendon. Once the thumb MCP joint is fused, the EPB tendon becomes functionally redundant, as its primary role is MCP extension. Rather than discarding this valuable tissue, the EPB tendon can be harvested at its musculotendinous junction, mobilized, and transferred to the first dorsal interosseous insertion to restore index finger abduction. This elegant salvage maneuver spares the EIP or APL for other necessary reconstructive procedures and utilizes local tissue that is already in the operative field.
Complications, Incidence Rates, and Salvage Management
To achieve true mastery in tendon transfer surgery, the orthopedic surgeon must not only execute the procedure flawlessly but also anticipate, recognize, and mitigate potential complications. The most common and devastating cause of transfer failure is improper tensioning. Based on the Blix curve of muscle length-tension, a transfer set too loose will fail to generate sufficient force, resulting in a weak pinch and persistent deformity. Conversely, a transfer set too tight may cause severe joint contractures, undergo ischemic necrosis at the suture line, or fail entirely due to rupture. Meticulous intraoperative tensioning, verified by the tenodesis effect during passive wrist motion, is the only safeguard against this complication.
Adhesions represent another significant hurdle, occurring in up to 15% of tendon transfers across the hand and wrist. Rough handling of the tendon, inadequate hemostasis leading to hematoma formation, or failure to create a sufficiently wide subcutaneous tunnel will inevitably lead to restrictive scar tissue formation. Surgeons must adhere to strict atraumatic tissue handling principles, utilizing moist sponges to handle tendons and strictly avoiding crushing forceps like Allis or Kocher clamps on any portion of the tendon that will be retained. If severe adhesions develop, a secondary tenolysis may be required, though this is technically demanding and carries its own risks.
Donor site morbidity is a critical consideration, particularly when harvesting the FDS tendon. In approximately 5-10% of cases, removal of the FDS can lead to a secondary swan-neck deformity or proximal interphalangeal (PIP) joint stiffness in the donor digit. This risk is mitigated by strictly preserving the FDP tendon, meticulously repairing the flexor sheath where possible, and initiating early, controlled mobilization. Similarly, when harvesting the EIP, failure to meticulously repair the extensor hood over the index MCP joint will result in a noticeable extensor lag and potential ulnar subluxation of the EDC tendon, a complication that requires prompt surgical revision.
| Complication | Estimated Incidence | Prevention Strategy | Salvage Management |
|---|---|---|---|
| Improper Tensioning | 10 - 15% | Intraoperative verification of tenodesis effect; proper joint positioning | Revision surgery (tightening/loosening); secondary tendon grafting |
| Restrictive Adhesions | 10 - 15% | Atraumatic handling; wide subcutaneous tunnels; meticulous hemostasis | Aggressive hand therapy; surgical tenolysis at 6 months post-op |
| Donor Digit Swan-Neck | 5 - 10% | Preserve FDP; avoid over-resection of FDS insertion; early ROM | FDP tenodesis; PIP joint volar plate advancement |
| Index Extensor Lag | < 5% | Meticulous 4-0 absorbable repair of the extensor expansion hood | Surgical revision and primary repair of the extensor mechanism |
| Transfer Rupture | < 2% | Robust Pulvertaft weave (3-4 passes); compliant post-op splinting | Primary repair if acute; alternative donor transfer if chronic |
Phased Post-Operative Rehabilitation Protocols
The surgical execution of a tendon transfer represents only half of the reconstructive journey; the ultimate success of the procedure is inextricably linked to a rigorous, phased postoperative rehabilitation protocol directed by a certified hand therapist. The rehabilitation timeline is strictly dictated by the biological phases of tendon healing. The initial phase, spanning weeks 0 to 3, is the Immobilization Phase. Immediately postoperatively, the surgical wounds are closed in layers, and a bulky, non-compressive dressing is applied to accommodate anticipated swelling. This is followed by the application of a rigid, custom-molded, forearm-based thumb spica splint. Crucially, the splint must hold the thumb in full palmar adduction, the index finger in radial abduction, and the wrist in moderate flexion (approximately 30 degrees) to completely remove tension from the newly woven transfers.
At exactly 3 weeks postoperatively, the primary biological healing at the tendon weave is sufficient to withstand gentle stress, marking the beginning of the Early Mobilization Phase (Weeks 3-6). The static surgical splint is removed, and active range-of-motion exercises are initiated. The therapist focuses on isolated, gravity-eliminated movements to facilitate tendon gliding and prevent restrictive adhesions. Cortical re-education is paramount during this phase; the patient is taught to fire the donor muscle (e.g., flexing the ring finger to activate the FDS) while visualizing the new biomechanical action (thumb adduction). Between exercise sessions, the patient must wear a removable, protective forearm-based thumb spica splint that specifically prevents thumb hyperextension and index ulnar deviation.
The Strengthening Phase commences at 6 weeks postoperatively, coinciding with the maturation and remodeling of the collagen fibers at the transfer site. Progressive resistance exercises are gradually introduced, utilizing therapy putty, grip dynamometers, and specialized pinch devices. The therapist carefully monitors the patient for any signs of transfer attenuation or joint pain. The protective splint is progressively weaned during the day but may be worn at night or during high-risk activities for an additional 2 to 4 weeks. Full, unrestricted activity, including heavy manual labor and sports, is typically permitted by 10 to 12 weeks postoperatively, provided the patient has achieved functional pinch strength and demonstrates no signs of transfer failure.
Summary of Landmark Literature and Clinical Guidelines
The evolution of tendon transfers for thumb intrinsic dysfunction is deeply rooted in a rich history of orthopedic literature and biomechanical research. The foundational work was laid by Royle in 1938 and subsequently refined by Thompson in 1942, who initially utilized the flexor digitorum superficialis to restore opposition in the setting of median nerve palsy. However, it was the seminal contributions of Riordan in the 1950s and Paul Brand in the 1970s that transformed these early concepts into the highly specific, biomechanically optimized transfers utilized today. Brand’s exhaustive studies on muscle mechanics, specifically his codification of muscle excursion, cross-sectional area, and tension fraction, remain the absolute gold standard for donor selection in modern hand surgery.
The use of the Extensor Indicis Proprius (EIP) for restoring first dorsal interosseous function was extensively popularized by Burkhalter and subsequently validated by numerous long-term outcome studies. Literature demonstrates that when the EIP is properly routed and tensioned, patients can expect a
