Skier's Thumb Case Study: Diagnosing Ulnar Collateral Ligament Rupture & Stener Lesion
Key Takeaway
Diagnosis of Skier's Thumb (UCL rupture) involves a detailed clinical examination, including valgus stress testing that reveals significant instability. A palpable firm mass near the MCP joint strongly suggests a Stener lesion. MRI imaging is crucial for confirming a complete UCL tear and identifying the Stener lesion's displacement, guiding appropriate surgical intervention.
A 35-year-old software engineer presents following a skiing injury. He has significant tenderness over the ulnar aspect of the thumb MCP joint and a palpable mass. You suspect a Stener lesion. What is the clinical significance of this lesion, and how does it dictate your management plan?
Candidate: A Stener lesion is where the distal UCL is torn and becomes trapped outside the adductor aponeurosis. This acts as a mechanical block to healing, so it requires surgery. If you don't operate, the ligament won't heal to the bone, leading to chronic instability and arthritis.
Candidates often focus only on the "trap" mechanism without mentioning the crucial biomechanical implications for the patient's occupation. They also frequently fail to describe the specific physical examination findings (palpable mass) that correlate with the diagnosis.
A Stener lesion occurs when the distally avulsed UCL is displaced superficial to the adductor pollicis aponeurosis. The aponeurosis interposes between the ligament stump and its anatomic footprint at the base of the proximal phalanx, creating a permanent mechanical barrier to healing. Given this patient's high-demand occupation requiring fine motor control and pinch stability, surgical exploration is mandatory to anatomically reduce the ligament. Non-operative treatment in the presence of a Stener lesion is doomed to failure, resulting in chronic joint instability, pinch weakness, and secondary osteoarthritis.
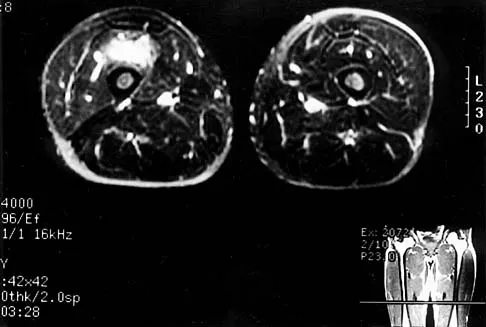
You have decided to proceed to surgery. This image represents a classic diagnostic finding associated with the injury. Describe the imaging finding and explain why you would not perform stress radiography in this case.
Candidate: This image shows the "yo-yo on a string" sign. The "yo-yo" is the retracted UCL stump and the "string" is the adductor aponeurosis. I wouldn't do stress radiographs because I suspect a Stener lesion, and the stress test could potentially convert a partial or non-displaced tear into a complete or displaced one.
Failing to emphasize the *iatrogenic* risk. Examiners want to hear that you recognize the clinical diagnosis (palpable mass + laxity) is sufficient to make the diagnosis, rendering further stress imaging redundant and potentially harmful.
The image illustrates the 'yo-yo on a string' sign—the pathognomonic MRI finding for a Stener lesion. The 'yo-yo' represents the retracted distal ligamentous stump, and the 'string' is the adductor aponeurosis. Stress radiography is contraindicated here because the patient has a clear clinical diagnosis of complete rupture with an associated Stener lesion. Applying further valgus stress creates an unacceptable risk of iatrogenically displacing a non-displaced ligament or extending a partial injury into a complete, displaced rupture.
Describe your surgical approach, specifically highlighting how you avoid injury to critical surrounding structures.
Candidate: I use a lazy-S incision on the ulnar aspect of the thumb. I perform blunt dissection to find the dorsal sensory branch of the radial nerve. I protect it with a vessel loop. Then I incise the adductor aponeurosis longitudinally to reach the joint.
Candidates often forget to mention the design of the skin incision (avoiding a longitudinal line to prevent scar contracture) or fail to specify the importance of keeping a 'cuff' of aponeurosis for later repair.
I utilize a lazy-S or chevron incision to avoid a straight line across the flexion crease, preventing contracture. After skin incision, the primary priority is identifying and protecting the terminal branches of the dorsal sensory branch of the radial nerve (Wartenberg's nerve) using blunt dissection and gentle retraction. Upon reaching the adductor aponeurosis, I perform a longitudinal incision, taking care to leave a 2–3 mm cuff attached to the extensor mechanism. This cuff is vital for ensuring a robust, anatomic closure of the aponeurosis at the end of the procedure, restoring dynamic stability.
