Proximal Interphalangeal Joint Capsulotomy: Comprehensive Surgical Guide
Key Takeaway
Proximal interphalangeal (PIP) joint capsulotomy is a precise surgical intervention indicated for severe, refractory joint stiffness where articular cartilage remains intact. This procedure addresses yielding surrounding tissues, extensor tendon adhesions, and collateral ligament contractures. Success relies on meticulous stepwise release of the collateral ligaments, volar plate checkreins, and contracted soft tissues, ideally performed under regional anesthesia to allow intraoperative assessment of active motion.
Comprehensive Introduction and Patho-Epidemiology
The proximal interphalangeal (PIP) joint is universally recognized as the functional epicenter of the digital ray, accounting for approximately 85% of the total flexion arc of the finger. Because of its complex capsuloligamentous anatomy and its intimate, unforgiving relationship with both the flexor and extensor mechanisms, the PIP joint is notoriously prone to severe, refractory stiffness following trauma, infection, or prolonged immobilization. The functional impairment resulting from a stiff PIP joint cannot be overstated; a loss of PIP flexion severely diminishes power grip, while a lack of extension critically impairs the ability to open the hand to grasp large objects.
The patho-epidemiology of PIP joint stiffness is rooted in the unique biological and biomechanical responses of the digital soft tissues to injury. Following trauma—whether a direct crush injury, a periarticular fracture, or a simple sprain—the joint undergoes an intense inflammatory phase characterized by profound edema. This protein-rich exudate rapidly organizes into a fibrinous network, which serves as a scaffold for fibroblastic proliferation. If the joint is immobilized during this critical window, myofibroblasts deposit dense, cross-linked type I collagen, obliterating the delicate gliding planes of the joint capsule, collateral ligaments, and adjacent tendinous structures.
Proximal interphalangeal joint capsulotomy is a highly specialized, salvage-level soft-tissue reconstruction designed to meticulously dismantle this pathological scar tissue. It is indicated strictly when the surrounding tissues are yielding, the articular surface integrity has been radiographically and clinically maintained, and the primary offenders to motion limitation are isolated to extensor tendon adhesions, dorsal capsular tightness, and collateral ligament contractures. The procedure demands profound anatomical knowledge, as the surgeon must navigate a labyrinth of contracted tissues without destabilizing the joint or devascularizing the critical structures.
It is imperative for the operating surgeon to understand that capsulotomy is not a panacea for all stiff digits. The procedure is fundamentally contraindicated in the presence of severe articular destruction, advanced osteoarthritis, or unyielding bony ankylosis. In such cases, the biological limits of soft tissue release have been surpassed, and salvage procedures such as silicone or pyrocarbon arthroplasty, or formal arthrodesis, must be considered. The decision to proceed with a capsulotomy must therefore be predicated on a rigorous, exhaustive preoperative assessment of the joint's biological and mechanical potential.
Detailed Surgical Anatomy and Biomechanics
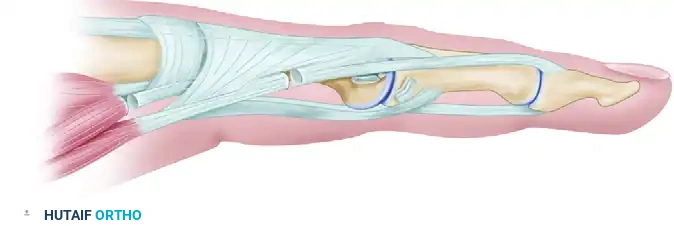
Understanding the intricate kinematics and microanatomy of the PIP joint is paramount before undertaking a capsular release. The PIP joint is a true ginglymus (hinge) joint, characterized by a bicondylar proximal phalangeal head articulating with the dual biconcave facets of the base of the middle phalanx. This specific osteology confers inherent osseous stability in the coronal plane, while allowing a massive arc of motion in the sagittal plane, typically ranging from 0 degrees of extension to 110 degrees of flexion. The condyles of the proximal phalanx are asymmetrical, and their cam-shaped geometry dictates the tensioning of the collateral ligaments throughout the arc of motion.
Stability and motion are dictated by a delicate, highly interdependent balance of capsuloligamentous structures. The Proper Collateral Ligaments (PCL) are robust, cord-like bands originating from the dorsal-lateral condylar recesses of the proximal phalanx and inserting into the volar-lateral base of the middle phalanx. Due to the cam effect of the proximal phalangeal head, the PCLs are maximally taut in deep flexion and relatively lax in full extension. Conversely, the Accessory Collateral Ligaments (ACL) are situated volar to the PCL, fanning out to insert extensively into the margins of the volar plate. The ACLs are taut in extension and lax in flexion, working in concert with the volar plate to resist hyperextension forces.
The volar plate itself is a thick, structurally complex fibrocartilaginous structure that forms the floor of the PIP joint. Distally, it has a rigid osseous insertion into the base of the middle phalanx, while proximally it transitions into a membranous structure that must fold upon itself like an accordion during joint flexion. The proximal lateral extensions of the volar plate are tethered by the checkrein ligaments. As classically described by Watson, Light, and Johnson, these robust ligamentous structures consist of fibers originating from the dorsal portion of the flexor sheath and reflections of the accessory ligament. They extend from thick attachments along the proximal edge of the volar plate and diverge to insert separately along the volar-lateral periosteum of the proximal phalanx.
When the PIP joint is immobilized in flexion, a predictable cascade of contractures occurs. The proper collateral ligaments shorten in their lax state, the volar plate proximal recess becomes obliterated by scar tissue, and the checkrein ligaments undergo severe fibrotic contraction, leading to a rigid, fixed flexion deformity. Conversely, immobilization in extension leads to shortening of the proper collateral ligaments in their relaxed, extended position, effectively tethering the joint and preventing subsequent flexion. Understanding this specific pathoanatomy is the foundation of the Curtis classification and dictates the exact sequence of surgical release required to restore physiological kinematics.
Exhaustive Indications and Contraindications
The decision to perform a PIP joint capsulotomy requires a highly nuanced clinical judgment, balancing the patient's functional deficit against the inherent risks of surgical intervention. The primary indication is severe, refractory PIP joint stiffness that has failed to improve after a minimum of 3 to 6 months of rigorous, specialized hand therapy, including static progressive and dynamic splinting. The stiffness must be significantly impairing the patient's activities of daily living or occupational duties. Furthermore, the surgeon must confirm that the articular cartilage is preserved; a joint with a congruent, well-maintained radiographic joint space is the ideal candidate for soft tissue release.
Before proceeding to surgery, the exact anatomical structures restricting motion must be systematically identified using the Curtis classification. For flexion deficits, the surgeon must evaluate for dorsal skin contracture, extensor mechanism adherence, intrinsic muscle tightness (via a positive Bunnell test), and proper collateral ligament contracture. For extension deficits, the evaluation must rule out volar skin scarring, Dupuytren's fascial cords, flexor tendon sheath contracture, flexor tendon adherence, and volar plate/checkrein ligament fibrosis. The capsulotomy is indicated when the primary block to motion is capsuloligamentous in nature.
Contraindications to PIP joint capsulotomy are strict and must be respected to avoid catastrophic outcomes. Absolute contraindications include advanced degenerative joint disease, post-traumatic articular step-off or incongruity, active periarticular infection, and untreated Complex Regional Pain Syndrome (CRPS). Attempting a capsulotomy in a joint with denuded cartilage will only result in exacerbated pain, recurrent stiffness, and accelerated joint destruction. Additionally, patients with severe, unyielding soft tissue deficits (such as a severely crushed digit with global scarring) or those who are psychologically incapable of complying with the grueling postoperative rehabilitation protocol are considered poor candidates.
Relative contraindications include the presence of concomitant, severe flexor tendon adhesions that require a massive tenolysis. While a staged approach is possible, attempting a simultaneous aggressive capsulotomy and a complex flexor tenolysis in a single setting is fraught with complications. The resulting inflammatory response, hematoma formation, and global scar tissue proliferation will almost certainly lead to recurrent, intractable stiffness. In such scenarios, the surgeon must carefully stage the reconstruction, prioritizing passive motion restoration first, followed by active motion restoration at a later date.
| Clinical Parameter | Indications for Capsulotomy | Contraindications for Capsulotomy |
|---|---|---|
| Duration of Stiffness | > 3-6 months of failed conservative therapy | < 3 months (continue therapy/splinting) |
| Articular Status | Intact cartilage, congruent joint space | Advanced OA, articular destruction, bony ankylosis |
| Primary Pathology | Isolated capsuloligamentous contracture (PCL, Volar Plate, Checkreins) | Severe global crush injury, active infection |
| Soft Tissue Envelope | Pliable, well-vascularized skin | Severe scarring requiring flap coverage, active CRPS |
| Patient Factors | Highly compliant, understands rehab demands | Non-compliant, unable to participate in daily therapy |
| Concomitant Issues | Isolated stiffness, or planned staged tenolysis | Simultaneous need for complex flexor tenolysis (relative) |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for a PIP joint capsulotomy begins with a meticulous, highly structured physical examination. The surgeon must precisely document the active and passive arcs of motion of the metacarpophalangeal (MCP), PIP, and distal interphalangeal (DIP) joints. A critical component of the examination is the intrinsic tightness test (Bunnell test). By holding the MCP joint in full extension and passively flexing the PIP joint, the surgeon assesses the tension of the interosseous and lumbrical muscles. If PIP flexion is significantly more restricted when the MCP is extended compared to when it is flexed, intrinsic tightness is confirmed, and an intrinsic release must be incorporated into the surgical plan.
Radiographic templating is equally critical, albeit less focused on hardware sizing and more focused on joint space analysis. True anteroposterior, lateral, and oblique radiographs of the individual digit must be obtained. The surgeon must scrutinize the joint space for symmetrical preservation of the cartilage interval, the presence of marginal osteophytes, or hidden dorsal/volar osseous blocks (exostoses) that could impinge during motion. If there is any doubt regarding the articular integrity or the presence of subtle intra-articular fractures, a high-resolution computed tomography (CT) scan of the digit should be strongly considered to definitively map the osseous architecture.
The choice of anesthesia has undergone a paradigm shift in modern hand surgery. The "Awake Patient Concept," utilizing the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique, is now considered the gold standard for PIP joint capsulotomy. By injecting a buffered solution of 1% lidocaine with 1:100,000 epinephrine into the subcutaneous tissues of the digit and palm, the surgeon achieves profound local anesthesia and a bloodless surgical field without the need for a pneumatic tourniquet. Crucially, because the extrinsic flexor and extensor muscles remain unparalyzed, the awake patient can actively move the digit upon command intraoperatively. This provides the surgeon with real-time, dynamic feedback regarding the adequacy of the capsular release and the presence of any residual tendon adhesions.
Patient positioning is straightforward but requires attention to ergonomic detail. The patient is positioned supine with the operative arm extended onto a radiolucent hand table. If WALANT is not utilized, a well-padded upper arm tourniquet is applied, and the limb is exsanguinated with an Esmarch bandage. The surgeon sits seated, utilizing loupe magnification (typically 2.5x to 3.5x) and a focused surgical headlight to ensure pristine visualization of the microanatomy. The surgical field is prepped and draped in a standard sterile fashion, ensuring the entire hand and wrist are exposed to allow for full kinematic assessment of the extrinsic tendons during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Midlateral Surgical Approach and Exposure
The surgical approach to the PIP joint must provide wide, unhindered access to both the dorsal and volar capsular structures while minimizing the risk of postoperative scar contracture. The midlateral incision is universally preferred over dorsal or volar approaches. By placing the incision exactly along the midaxial line—connecting the apices of the flexion creases of the digit—the resulting scar remains in the neutral axis of motion, thereby preventing irogenic flexion or extension contractures. The incision is carried sharply through the dermis, and delicate blunt dissection is utilized to navigate the subcutaneous tissues.
Upon deepening the incision, the surgeon must carefully identify and mobilize the neurovascular bundle, which lies volar to the midaxial line. Cleland's cutaneous ligaments, which are dorsal to the neurovascular bundle, are sharply divided to allow volar retraction of the digital artery and nerve. Grayson's ligaments, located volar to the bundle, may also require partial release. Retracting the neurovascular bundle safely out of the surgical field is paramount to preventing devastating iatrogenic injury during the deep capsular dissection.
Elevation of the Transverse Retinacular Ligament
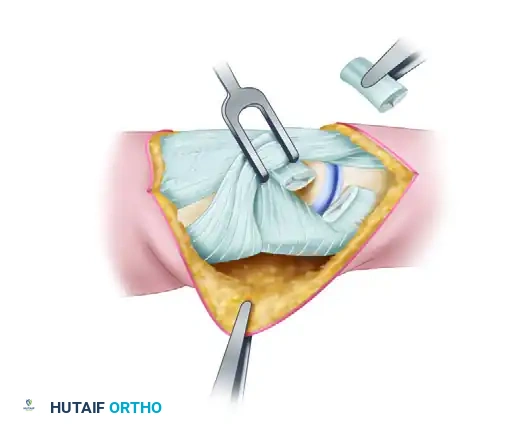
With the neurovascular bundle protected, the surgeon's attention turns to the extensor mechanism. The transverse retinacular ligament (TRL) is a critical stabilizing structure that originates from the volar capsule and the edge of the flexor tendon sheath, sweeping dorsally to insert onto the lateral border of the lateral band of the extensor mechanism. The TRL prevents dorsal subluxation of the lateral bands during PIP joint extension. To access the underlying collateral ligaments, the TRL must be meticulously identified and elevated.

Using fine tenotomy scissors or a scalpel, the TRL is incised parallel to the lateral band, leaving a sufficient cuff of tissue on the lateral band to facilitate robust repair at the conclusion of the procedure. The TRL is then reflected volarly, exposing the underlying proper and accessory collateral ligaments. Failure to preserve and subsequently repair the TRL is a catastrophic technical error; without an intact TRL, the lateral bands will subluxate dorsally during the postoperative rehabilitation phase, inevitably leading to a rigid, iatrogenic swan-neck deformity.
Excision of the Collateral Ligaments
Once the collateral ligament complex is fully visualized, the surgeon must identify the thick, cord-like proper collateral ligament (PCL). In a stiff PIP joint, the PCL is typically profoundly contracted, thickened, and fibrotic. The standard technique, as pioneered by Curtis, dictates that the PCL must be excised en bloc, not merely transected. A simple transverse release of the ligament is insufficient, as the raw edges will rapidly bridge with scar tissue during the inflammatory phase of healing, leading to immediate recurrence of stiffness.
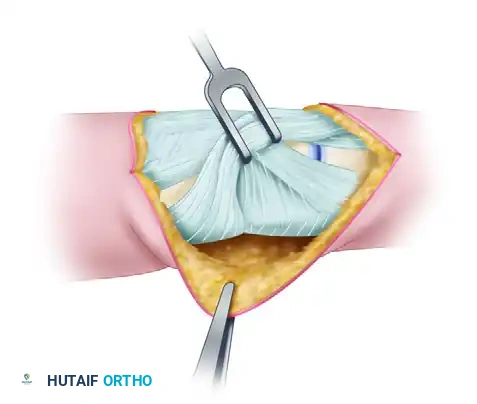
Starting at its distal attachment on the volar-lateral base of the middle phalanx, the PCL is sharply elevated off the bone. The dissection is carried proximally to its origin on the dorsal-lateral condylar recess of the proximal phalanx. The entire cord portion of the ligament is resected. This precise maneuver must be repeated on the contralateral side of the joint, requiring a second midlateral incision. Bilateral excision of the PCLs is mandatory to restore symmetrical, unimpeded glide of the proximal phalangeal condyles.
Volar Pouch Restoration and Checkrein Release
Following collateral ligament excision, the surgeon must address the volar pathology, particularly in cases with a severe flexion contracture. The volar synovial pouch—the critical gliding recess between the volar plate and the volar neck of the proximal phalanx—is frequently obliterated by dense, unyielding synechiae. To restore this pouch, a small, curved elevator (such as a Freer elevator) is gently introduced into the recess. The surgeon carefully sweeps away the adhesions, taking extreme care not to perforate the volar plate or injure the delicate vincula brevis and longa, which supply critical blood flow to the flexor tendons.
If restoring the volar pouch does not yield full passive extension, the checkrein ligaments must be addressed. As emphasized by Watson, Light, and Johnson, the checkreins are the primary tethering structures in persistent flexion deformities. These thick, fibrotic bands extend from the proximal edge of the volar plate and diverge to insert into the volar-lateral periosteum of the proximal phalanx. The surgeon must isolate these checkreins bilaterally and resect them sharply. Once the checkreins are divided, the volar plate is freed from its proximal tethers, allowing it to glide distally and permitting full, unhindered extension of the PIP joint.
Addressing Intrinsic Contractures and Fixation Technique
If preoperative assessment or intraoperative testing reveals intrinsic muscle tightness, an intrinsic release must be performed to allow full PIP flexion. The lateral band, which carries the terminal fibers of the interosseous muscles, is identified through the existing midlateral approach.

A step-cut tenotomy is meticulously executed on the lateral band/interosseous tendon complex. The tendon is incised longitudinally, and transverse cuts are made at opposite ends of the longitudinal incision.
The digit is then passively flexed, allowing the step-cut ends to slide apart and elongate the tendinous unit. The elongated ends are then repaired with fine, non-absorbable suture (e.g., 4-0 or 5-0 Prolene).
Regarding "fixation technique" in the context of a capsulotomy, internal osseous fixation is generally not required unless severe, unexpected instability is encountered. However, soft tissue fixation is paramount. The TRL must be meticulously repaired with 5-0 absorbable sutures to prevent swan-neck deformity. In extremely rare cases where the joint is hopelessly unstable post-release, temporary transarticular K-wire fixation (0.035 or 0.045 inch) holding the joint in extension for 3 to 5 days may be utilized, though this heavily compromises the goal of early mobilization and is generally discouraged unless absolutely necessary to protect a tenuous vascular or nerve repair.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, PIP joint capsulotomy is an inherently high-risk procedure with a significant complication profile. The most common and frustrating complication is recurrent stiffness. The biological drive for the digit to form scar tissue is immense, and any lapse in immediate, aggressive postoperative rehabilitation will result in the rapid reformation of capsular contractures. Hematoma formation within the joint space further exacerbates this risk by providing a rich, fibrinous scaffold for accelerated fibroblastic proliferation. Meticulous hemostasis, often facilitated by the epinephrine in WALANT, is critical to mitigating this risk.
A devastating biomechanical complication is the development of an iatrogenic swan-neck deformity. This occurs almost exclusively due to failure to properly identify, preserve, and robustly repair the transverse retinacular ligament during the surgical exposure. Without the tethering effect of the TRL, the lateral bands subluxate dorsal to the axis of rotation of the PIP joint during extension, creating a massive hyperextension moment. Correction of this deformity requires a complex secondary operation, such as a superficialis tenodesis or a lateral band rerouting procedure, significantly compromising the final functional outcome.
Infection and neurovascular injury are less common but potentially catastrophic complications. The midlateral approach places the digital neurovascular bundle at immediate risk. Iatrogenic transection of the digital nerve results in painful neuroma formation and sensory loss, while injury to the digital artery can threaten the viability of the digit, especially in patients with preexisting vascular compromise. Furthermore, aggressive dissection within the volar pouch can disrupt the vincula, leading to avascular necrosis of the flexor tendons and subsequent spontaneous rupture.
When a capsulotomy fails and the joint returns to a rigid, non-functional state, salvage procedures must be employed. The choice of salvage depends heavily on the specific digit involved and the patient's occupational demands. For the index and middle fingers, where lateral pinch stability is paramount, a formal PIP joint arthrodesis positioned in 40 to 50 degrees of flexion is often the most reliable and durable solution. For the ring and small fingers, where a mobile flexion arc is critical for power grip, implant arthroplasty (utilizing silicone elastomers or modern pyrocarbon implants) may be considered, provided the bone stock and collateral ligaments are sufficient to support the prosthesis.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Recurrent Stiffness | 20% - 40% | Poor therapy compliance, hematoma, prolonged immobilization | Serial casting, static progressive splinting; rarely revision surgery |
| Swan-Neck Deformity | 5% - 10% | Failure to repair Transverse Retinacular Ligament (TRL) | TRL reconstruction, FDS tenodesis, lateral band rerouting |
| Joint Instability | 2% - 5% | Over-resection of collateral ligaments, unrecognized bone loss | Prolonged splinting, ligament reconstruction, Arthrodesis |
| Infection | 1% - 3% | Poor sterile technique, compromised soft tissue envelope | Aggressive I&D, targeted IV antibiotics, hardware removal (if any) |
| CRPS | 2% - 5% | Undiagnosed pre-op CRPS, severe post-op pain cycle | Stellate ganglion blocks, aggressive pain management, desensitization |
| Flexor Tendon Rupture | < 1% | Iatrogenic injury to vincula causing avascular necrosis | Tendon grafting, staged reconstruction, or Arthrodesis |
Phased Post-Operative Rehabilitation Protocols
The ultimate success of a PIP joint capsulotomy is inextricably linked to the rigorous, relentless execution of the postoperative rehabilitation protocol. The surgical release merely creates the potential for motion; it is the immediate, sustained mechanical loading provided by hand therapy that dictates the final functional outcome. The protocol is divided into distinct, aggressive phases, requiring a highly motivated patient and a specialized, certified hand therapist.
Phase 1 encompasses the first 14 days postoperatively and is defined by immediate, controlled mobilization. The bulky intraoperative compressive dressing is removed within 24 to 48 hours. Edema control is paramount and is achieved through Coban wrapping, elevation, and retrograde massage. Active and active-assisted range of motion exercises are initiated immediately. If WALANT was utilized, the patient already understands the expected arc of motion. During rest periods, the digit is managed with dynamic or static progressive splinting. If the primary preoperative deficit was a flexion contracture, an extension orthosis (such as a Capener splint or a static progressive extension splint) is worn almost continuously, removed only for active flexion exercises.
Phase 2 spans from week 2 to week 6 and focuses on scar remodeling and maximizing the end-range of motion. Suture removal occurs at approximately 14 days. Scar massage with silicone gel sheeting is initiated to prevent dermal adherence to the underlying extensor mechanism. The splinting regimen is aggressively titrated based on the joint's tendency to stiffen. A "wear-and-tear" approach is often adopted: dynamic flexion strapping is utilized during the day to force the joint into deep flexion, while rigid static extension splinting is mandated at night to prevent the insidious recurrence of a flexion contracture. The therapist must constantly balance the forces, ensuring neither flexion nor extension is gained at the expense of the other.
Phase 3 begins at 6 weeks and extends for several months. The focus shifts towards functional strengthening, work conditioning, and weaning from the rigid splinting protocols. Grip and pinch strengthening exercises are introduced using putty, hand dynamometers, and functional tasks. Patients must be heavily counseled preoperatively that splinting may be necessary at least part of the time for 3 to 6 months postoperatively. Long-term outcomes literature suggests that while the functional arc of motion is vastly improved, a completely "normal" joint is rarely achieved. A residual lack of terminal extension (10 to 15 degrees) is common, biologically expected, and generally well-tolerated functionally, provided the digit can flex sufficiently to participate in power grip.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the PIP joint capsulotomy is chronicled through several landmark publications that have fundamentally shaped modern orthopedic hand surgery. The foundational principles were established by Raymond M. Curtis in his seminal 1954 paper, "Capsulectomy of the Interphalangeal Joints of the Fingers." Curtis was the first to systematically categorize the anatomical structures responsible for limited motion and advocated for the radical, en bloc excision of the proper collateral ligaments, rather than simple transection. His classification system remains the gold standard for preoperative evaluation and intraoperative decision-making to this day.
A critical advancement in the understanding of volar pathology was published by Watson, Light, and Johnson in 1979 in their paper, "Checkrein Resection for Flexion Contracture of the Middle Joint." Prior to their work, many surgeons struggled to achieve full extension despite aggressive collateral ligament excision and volar plate release. Watson and his colleagues elegantly described the microanatomy of the checkrein ligaments, proving that these dense, fibrotic bands tethering the proximal volar plate were the primary culprits in refractory flexion contractures. Their mandate that checkrein resection be considered an obligatory part of all PIP joint releases revolutionized the surgical technique and drastically improved extension outcomes.
In recent decades, the literature has heavily focused on the optimization of anesthesia and the mitigation of intraoperative complications. The widespread adoption of the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique, championed by Donald Lalonde and others, has transformed the procedure. Numerous prospective cohort studies have demonstrated that
