Benign Tumors of the Hand: Diagnosis, Staging, and Surgical Management

Key Takeaway
Benign tumors of the hand require meticulous clinical evaluation, appropriate imaging, and precise surgical execution to minimize recurrence and preserve hand function. While history and plain radiographs often suffice for diagnosis, aggressive lesions necessitate advanced MRI or CT staging. Treatment predominantly involves marginal or intralesional excision, with careful adherence to oncologic principles and preservation of critical neurovascular structures.
Comprehensive Introduction and Patho-Epidemiology
The evaluation, diagnosis, and surgical management of benign tumors in the hand and wrist demand an exceptionally profound understanding of complex regional anatomy, highly specialized biomechanics, and rigorous orthopedic oncologic principles. The human hand is composed of tightly packed, functionally critical structures constrained within small, unyielding anatomical compartments. Consequently, even histologically benign and slow-growing lesions can precipitate significant clinical morbidity. This morbidity manifests primarily through mechanical compression of adjacent structures, structural weakening of the osseous architecture leading to pathologic fractures, or direct neurovascular compromise resulting in sensory deficits and motor dysfunction.
Epidemiologically, while ganglion cysts represent the most common tumor-like lesions of the hand and wrist, true neoplastic benign tumors exhibit a diverse histopathological spectrum. Giant Cell Tumor of Tendon Sheath (GCTTS) represents the most common primary solid soft-tissue tumor of the hand, frequently presenting on the volar aspect of the digits. Adipocytic tumors, particularly lipomas, are also exceedingly common, though their deep palmar variants often present unique diagnostic and surgical challenges due to their propensity to track along fascial planes. Peripheral nerve sheath tumors, notably schwannomas and neurofibromas, constitute another significant subset, requiring meticulous microsurgical techniques for extirpation without inducing iatrogenic neurologic deficits. Within the osseous domain, enchondromas overwhelmingly dominate the epidemiological landscape, representing the most common primary bone tumor of the hand, classically presenting in the proximal phalanges or metacarpals, often heralded by a pathologic fracture following trivial trauma.
The patho-epidemiology of these lesions dictates that while malignant transformation is exceedingly rare in the majority of solitary benign hand tumors, specific syndromic associations warrant heightened clinical vigilance. For instance, multiple enchondromatosis (Ollier disease) or its association with soft tissue hemangiomas (Maffucci syndrome) dramatically increases the lifetime risk of chondrosarcoma. Similarly, the presence of multiple neurofibromas in the context of Neurofibromatosis Type 1 (NF1) carries a well-documented 8% to 15% lifetime risk of malignant peripheral nerve sheath tumor (MPNST) degeneration. Therefore, the orthopedic surgeon must approach every hand mass with a high index of suspicion, ensuring that a comprehensive diagnostic pathway is strictly adhered to before any surgical intervention is contemplated.
Usually, a thorough history, meticulous physical examination, and high-quality plain radiographs are sufficient to adequately determine the diagnosis and formulate an appropriate treatment plan for classically benign-appearing tumors. However, if a more aggressive process is suspected—evidenced by intractable rest pain, rapid exponential growth, severe perilesional inflammation, a soft tissue mass greater than 5 cm, or radiographic evidence of permeative bony destruction—further diagnostic and systemic staging studies are strictly warranted before proceeding with any biopsy or definitive surgical excision.
Detailed Surgical Anatomy and Biomechanics
The surgical extirpation of hand tumors requires an intimate, three-dimensional spatial awareness of the hand's intricate anatomy. The palmar aponeurosis, a robust, triangular fascial condensation in the central palm, plays a pivotal role in the clinical presentation of deep space tumors. Because this fascial layer is essentially unyielding, deep palmar space lesions, such as complex lipomas or hemangiomas, are forced to project through the paths of least resistance. They frequently track distally through the lumbrical canals, presenting as asymmetrical masses between the fingers and thumb, or they may project dorsally, driven by the unyielding overlying palmar aponeurosis. This dorsal projection can cause web space widening and a palpable dorsal mass, a phenomenon that can clinically mislead the unwary surgeon regarding the tumor's true epicenter.
The neurovascular topography is of paramount importance during tumor resection. The common digital nerves, terminal branches of the median and ulnar nerves, travel volar to the superficial palmar arch and divide into proper digital nerves proximal to the metacarpophalangeal (MCP) flexion creases. Benign peripheral nerve sheath tumors, such as schwannomas (neurilemmomas), typically grow eccentrically from the nerve fascicles, displacing the functional neural tissue to the periphery of the epineurium. This eccentric growth allows for meticulous microsurgical enucleation. Conversely, neurofibromas exhibit a central, infiltrative growth pattern, intimately intertwining with the nerve fascicles, making complete excision without creating a profound neurological deficit virtually impossible. Understanding this anatomical and histopathological distinction is critical for preoperative patient counseling and intraoperative decision-making.
The flexor tendon sheath mechanism, comprising the annular (A1-A5) and cruciate (C1-C3) pulleys, intimately surrounds the flexor digitorum superficialis (FDS) and profundus (FDP) tendons. Giant Cell Tumors of the Tendon Sheath (GCTTS) arise directly from the synovial lining of these sheaths or adjacent interphalangeal joints. These tumors frequently exhibit a lobulated, multinodular growth pattern that wraps around the collateral ligaments, digital neurovascular bundles, and occasionally extends intra-articularly or causes pressure erosions on the underlying phalangeal cortex. Complete marginal excision requires a meticulous, bloodless field to identify and resect all microscopic satellite nodules, as failure to do so directly correlates with the historically high local recurrence rates associated with GCTTS.
From an osseous perspective, the metacarpals and phalanges possess a thin cortical shell surrounding a relatively voluminous medullary canal, particularly in the metaphyseal regions. This anatomical configuration makes them highly susceptible to structural compromise from expansile intramedullary lesions such as enchondromas or aneurysmal bone cysts (ABCs). The biomechanical forces exerted on the hand during power grip and pinch are substantial; thus, when an intramedullary tumor erodes more than 50% of the cortical diameter, the structural integrity of the ray is critically compromised, leading to the classic presentation of a pathologic fracture. Surgical management of these osseous lesions must therefore balance thorough oncologic curettage with the immediate biomechanical restoration of the digit using structural bone grafts or biocompatible cements.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for a benign tumor of the hand must be carefully weighed against the natural history of the specific lesion, the patient's functional demands, and the inherent risks of hand surgery, including stiffness, nerve injury, and complex regional pain syndrome (CRPS). Surgical excision is not universally mandated for all benign lesions; a period of watchful waiting is often appropriate for asymptomatic, static masses.
Strict indications for surgical intervention include impending or actual pathologic fractures secondary to expansile bone tumors, progressive neurological deficits caused by compressive neuropathies (e.g., a lipofibroma in the carpal tunnel), intractable pain (classically seen with glomus tumors or osteoid osteomas), and functional impairment due to mechanical block of joint excursion or tendon glide. Furthermore, any lesion exhibiting rapid growth, skin changes, or atypical imaging features mandates a diagnostic biopsy or excisional biopsy to definitively rule out a malignant sarcoma.
Conversely, absolute contraindications to surgical excision include the presence of an undiagnosed, potentially malignant mass without prior staging and biopsy planning. Injudicious "shelling out" of an unrecognized sarcoma (the "whoops" procedure) severely compromises subsequent limb-salvage options and drastically increases the risk of local recurrence and systemic metastasis. Relative contraindications include asymptomatic, static lesions in patients with severe medical comorbidities, or multiple neurofibromas in NF1 patients where excision would result in unacceptable, widespread neurological morbidity.
| Clinical Scenario / Pathology | Surgical Indications | Surgical Contraindications |
|---|---|---|
| Enchondroma (Intramedullary) | Pathologic fracture (post-healing), cortical thinning >50%, symptomatic pain. | Asymptomatic, incidental finding with thick intact cortices (Observation preferred). |
| Giant Cell Tumor of Tendon Sheath | Progressive enlargement, mechanical block to finger flexion, neurovascular compression. | Active local infection, medically unstable patient. |
| Schwannoma / Neurilemmoma | Symptomatic pain, Tinel's sign, progressive sensory/motor deficit, mass effect. | Asymptomatic small lesions (relative contraindication due to risk of iatrogenic nerve injury). |
| Neurofibroma (Solitary or NF1) | Severe intractable pain, rapid growth suggestive of MPNST degeneration. | Routine excision of asymptomatic lesions (inevitable permanent nerve deficit). |
| Suspected Sarcoma (>5cm, deep) | Strictly Contraindicated for Primary Excision. Requires longitudinal incisional biopsy and staging first. | Primary marginal excision ("shelling out") without prior biopsy and systemic staging. |
| Osteoid Osteoma | Severe nocturnal pain relieved by NSAIDs, functional limitation. | Pain easily controlled with minimal NSAID use (lesions may spontaneously resolve over years). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful hand oncology surgery. Local imaging studies are paramount for surgical planning, defining the anatomical extent of the lesion, and assessing compartmental boundaries. Plain radiographs are the mandatory first step in all hand tumors. They evaluate for osseous involvement, cortical scalloping, matrix calcification (e.g., the classic "rings and arcs" or stippled calcification seen in cartilaginous tumors), and pathologic fractures.
Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the undisputed gold standard for evaluating soft tissue tumors of the hand. MRI delineates the tumor's relationship to critical tendons, neurovascular bundles, and joint capsules. It is highly sensitive for identifying the fluid-fluid levels characteristic of an aneurysmal bone cyst (ABC), the specific signal characteristics of a lipoma (isointense to subcutaneous fat on all sequences, suppressing on STIR), or the hemosiderin deposition seen in GCTTS (blooming artifact on gradient-echo sequences). Computed Tomography (CT) is superior for evaluating cortical integrity, subtle matrix mineralization, and pinpointing the central radiolucent nidus of an osteoid osteoma, which is critical for planning precise surgical excision or radiofrequency ablation.
Orthopedic oncology relies heavily on the Enneking staging systems to guide surgical margins. For benign tumors, the Enneking Classification categorizes lesions into Stage 1 (Latent: static or healing, well-marginated, e.g., non-ossifying fibroma), Stage 2 (Active: growing, symptomatic, bounded by natural barriers, e.g., ABC), and Stage 3 (Aggressive: rapidly growing, breaching natural barriers, high recurrence rate, e.g., Giant Cell Tumor of Bone). The planned surgical margin—whether intracapsular (curettage), marginal (shelling out through the reactive zone), wide (intracompartmental en bloc), or radical (extracompartmental)—must be explicitly defined preoperatively based on the Enneking stage.
Patient positioning and anesthesia are critical components of the preoperative setup. The patient is typically positioned supine with the operative arm extended on a radiolucent hand table, allowing for unhindered fluoroscopic access. A well-padded pneumatic tourniquet is applied to the proximal arm to ensure a bloodless surgical field, which is absolutely vital for identifying microscopic satellite tumor nodules and preserving delicate digital nerves. Anesthesia is typically achieved via a regional block, such as an ultrasound-guided axillary brachial plexus block or an intravenous regional anesthesia (Bier block), supplemented with intravenous sedation. General anesthesia is reserved for pediatric patients, prolonged complex reconstructions, or when harvesting autologous bone graft from the iliac crest is anticipated.
Step-by-Step Surgical Approach and Fixation Technique
Extirpation of a Complex Palmar Lipoma
The following section details the step-by-step surgical extirpation of a complex, deep palmar lipoma that has tracked distally along the path of least resistance, presenting with significant dorsal prominence.
The patient presents with a substantial mass at the base of the middle finger. Due to the unyielding palmar aponeurosis, deep palmar lipomas often project dorsally, causing interference with grasp and finger adduction.

A thorough clinical examination often reveals a palpable mass on the palmar aspect that dramatically translates dorsally when the hand is clenched into a fist. The dorsal view with fingers extended highlights the asymmetric mass effect and web space widening caused by the palmar tumor projecting dorsally.

A volar zig-zag (Bruner) incision is meticulously designed over the palmar aspect of the affected digit, extending proximally into the palm. This classic approach prevents linear flexion contractures across the joint creases and provides wide, extensile exposure of the flexor tendon sheath and neurovascular bundles. The skin flaps are elevated full-thickness, ensuring the preservation of the delicate subdermal vascular plexus to prevent flap necrosis. Upon incising the palmar fascia, the tumor is frequently revealed to be much larger than clinically apparent, exhibiting extensive lobulation and insinuating itself between vital structures.
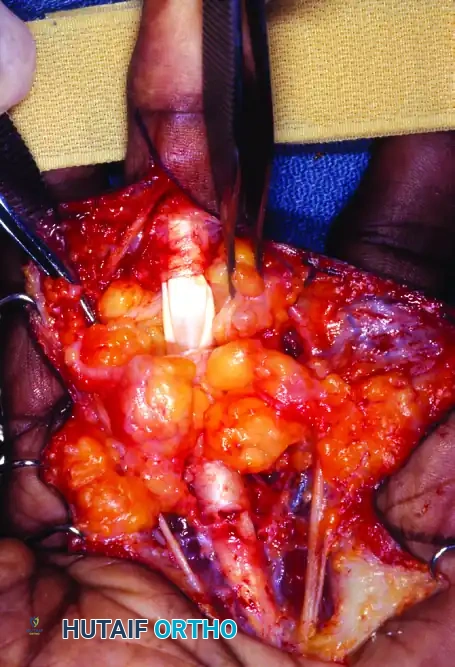
Careful, blunt dissection using tenotomy scissors or a blunt elevator is mandatory. The lipoma often intimately surrounds the common and proper digital nerves. The neurovascular bundles must be definitively identified proximally in normal, unscarred tissue. Once identified, they are gently mobilized and traced distally through the tumor mass using vessel loops for atraumatic retraction. The tumor is then marginally excised. Because true lipomas are encapsulated by a thin pseudocapsule, they can typically be "shelled out" once the neurovascular structures are safely mobilized. The flexor tendon sheath (A1 and A2 pulleys) should be strictly preserved unless directly infiltrated by a different, more aggressive pathology.

Following complete extirpation, the surgical bed must demonstrate pristine sparing of the glistening white flexor tendons and the intact digital nerves. The pneumatic tourniquet is routinely deflated prior to skin closure to ensure meticulous hemostasis. Bipolar electrocautery is utilized to control any bleeding vessels, thereby preventing postoperative hematoma formation, which can lead to severe fibrosis, stiffness, and delayed wound healing. The wound is irrigated copiously with sterile saline. The skin is closed using non-absorbable monofilament sutures (e.g., 4-0 or 5-0 Nylon) in an interrupted fashion.
Management of Benign Bone Tumors (Enchondroma)
For intramedullary benign bone tumors such as enchondromas, the surgical approach varies based on the anatomical location. For a proximal phalanx lesion, a mid-lateral or dorsal longitudinal approach is utilized, carefully retracting the lateral band or splitting the extensor tendon longitudinally. The periosteum is incised and elevated. A cortical window is created using a high-speed burr or osteotome, ensuring the window is large enough to access the entire extent of the intramedullary lesion.
Aggressive intralesional curettage is the cornerstone of treatment. Angled curettes are used to meticulously scrape the tumor from the endosteal surface of the medullary canal. Following macroscopic tumor removal, the cavity is expanded using a high-speed burr to remove any microscopic disease residing in the bony interstices—a technique known as extended curettage. Chemical adjuvants, such as 88% phenol followed by alcohol neutralization, or physical adjuvants like liquid nitrogen cryotherapy or argon beam coagulation, may be employed to further reduce the local recurrence rate.
Once the cavity is thoroughly debrided and sterilized, the resulting osseous defect must be managed. For small defects with robust remaining cortices, the cavity may be left to fill with hematoma. However, for larger defects that compromise biomechanical stability, the cavity is packed with autologous cancellous bone graft (harvested from the distal radius or iliac crest), allograft chips, or injectable calcium phosphate (CaPhos) bone cement. CaPhos cement provides immediate structural stability, allowing for earlier postoperative mobilization, and undergoes slow osteoclastic resorption and creeping substitution over time. The cortical window may be replaced, and the soft tissues are closed in layers. If the cortical destruction is massive, prophylactic internal fixation using a miniature plate and screw construct may be indicated to prevent postoperative fracture.
Complications, Incidence Rates, and Salvage Management
Surgical intervention for benign tumors of the hand, while generally highly successful, carries inherent risks that must be thoroughly discussed with the patient preoperatively. The complex, densely packed anatomy of the hand makes iatrogenic injury a constant threat, and the biological behavior of certain tumors predisposes them to local recurrence despite seemingly adequate surgical margins.
Local recurrence is a primary concern, particularly for specific histologies. Giant Cell Tumor of Tendon Sheath (GCTTS) carries a historical recurrence rate ranging from 10% to 20%. This is primarily attributed to the tumor's multinodular nature and the failure to resect microscopic satellite lesions during the index procedure. Infiltrating lipomas, which grow between and within muscle fibers without a true capsule, exhibit an exceptionally high recurrence rate (up to 60%) following marginal excision. Aneurysmal Bone Cysts (ABCs) and Giant Cell Tumors of Bone (GCT) also have notable recurrence rates if intralesional curettage is not aggressively supplemented with high-speed burring and adjuvant therapy.
Neurological complications range from transient neuropraxia due to traction, to permanent sensory or motor deficits resulting from direct nerve transection or aggressive intraneural dissection. Enucleation of a schwannoma carries a low risk of permanent deficit, but excision of a neurofibroma almost invariably results in loss of function of the involved nerve fascicles. Postoperative stiffness, secondary to tendon adhesions, prolonged immobilization, or excessive surgical trauma, is a ubiquitous risk in hand surgery. Complex Regional Pain Syndrome (CRPS) is a devastating, though relatively rare, complication characterized by disproportionate pain, autonomic dysfunction, and severe stiffness.
| Complication | Estimated Incidence | Prevention Strategies and Salvage Management |
|---|---|---|
| Local Tumor Recurrence (GCTTS) | 10% - 20% | Prevention: Meticulous marginal excision under tourniquet control and loupe magnification; aggressive search for satellite nodules. Salvage: Re-excision with wider margins; consider postoperative radiation therapy for multiple recurrences. |
| Digital Nerve Injury / Neuroma | 1% - 5% | Prevention: Proximal identification of nerves; use of vessel loops; avoidance of blind clamping. Salvage: Immediate microsurgical primary repair or nerve grafting; if delayed, neuroma excision and nerve reconstruction or targeted muscle reinnervation (TMR). |
| Postoperative Joint Stiffness | 15% - 30% | Prevention: Atraumatic tissue handling; meticulous hemostasis; early initiation of active range of motion (AROM). Salvage: Aggressive hand therapy; dynamic splinting; surgical tenolysis or capsulotomy for refractory cases >6 months. |
| Pathologic Fracture (Post-Curettage) | 2% - 8% | Prevention: Adequate filling of large osseous defects with structural bone graft or CaPhos cement; prophylactic internal fixation for cortical loss >50%. Salvage: Open reduction and internal fixation (ORIF) with supplemental bone grafting. |
| Complex Regional Pain Syndrome (CRPS) | 1% - 3% | Prevention: Preoperative Vitamin C (500mg daily); adequate postoperative pain control; early mobilization. Salvage: Multidisciplinary pain management; sympathetic nerve blocks; intensive desensitization therapy. |
Salvage management for local recurrence typically involves a more aggressive re-excision. In cases of recurrent GCT of bone with massive joint destruction, en bloc resection and complex reconstruction (e.g., osteoarticular allograft, custom arthroplasty, or arthrodesis) may be required. For iatrogenic nerve injuries, prompt recognition is critical. If a nerve is inadvertently transected, immediate primary epineurial repair using 8-0 or 9-0 nylon under an operating microscope yields the best functional results.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is as critical to the final functional outcome as the surgical extirpation itself. The hand is exceptionally prone to rapid, debilitating stiffness if immobilized for prolonged periods. Therefore, the overarching goal of rehabilitation is to protect the surgical repair or bone graft while initiating the earliest possible safe motion to prevent tendon adhesions and joint contractures.
Phase I: Immediate Postoperative Period (Days 0 to 14)
Immediately following surgery, a bulky, soft compressive dressing is applied. For soft tissue tumor excisions, the hand is typically immobilized in the "intrinsic-plus" position: the wrist extended 20 to 30 degrees, the MCP joints flexed 70 to 90 degrees, and the interphalangeal (IP) joints in full extension. This position maintains the collateral ligaments of the MCP joints at their maximal length, preventing extension contractures. The patient is instructed to keep the hand strictly elevated above heart level to minimize edema. Active range of motion (AROM) of the uninvolved digits, elbow, and shoulder is encouraged immediately. For bone tumor curettage with cementation, early protected motion can often begin within 3 to 5 days. Sutures are typically removed between 10 and 14 days postoperatively.
Phase II: Early Mobilization and Tendon Gliding (Weeks 2 to 6)
Once the initial wound healing is secure and sutures are removed, formal hand therapy commences. The bulky dressing is transitioned to a custom-molded thermoplastic splint, which is worn between exercise sessions. The focus shifts to edema control (using compression garments and retrograde massage) and scar management (silicone gel sheets and deep friction massage once the incision is fully closed). A rigorous regimen of tendon gliding exercises is initiated, progressing through straight fist, hook fist, and full fist positions to ensure differential glide between the FDS and FDP tendons. Passive range of motion (PROM) and gentle dynamic splinting may be introduced if active motion plateaus or if early contractures develop.
Phase III: Strengthening and Functional Restoration (Weeks 6 to 12+)
By the sixth postoperative week, soft tissue healing is generally robust, and bone grafts or cements have achieved sufficient integration to tolerate increased loads. The splint is progressively discontinued. Progressive resistance exercises are initiated using therapy putty, hand grippers, and graduated weights. Work-hardening programs and sports-specific training are incorporated as the patient approaches full functional recovery. For patients who underwent bone grafting for large enchondromas, heavy lifting and high-impact activities are typically restricted until radiographic evidence of complete graft incorporation and cortical remodeling is confirmed, which may take 10 to 16 weeks.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of benign hand tumors is heavily influenced by several landmark contributions to orthopedic oncology and hand surgery literature.
The foundational staging system utilized universally in orthopedic oncology was developed by William F. Enneking. His seminal work established the Enneking Staging System for benign musculoskeletal tumors, categorizing them based on clinical, radiographic, and histological characteristics into latent, active, and aggressive stages. This system remains the absolute standard for determining the necessary surgical margins (intracapsular, marginal, wide, or radical) to minimize recurrence while preserving function.
For Giant Cell Tumors of Bone (GCT), the Campanacci Grading System is the definitive clinical guideline. Campanacci's radiographic classification (Grade I: well-marginated, Grade II: expanded but intact cortex, Grade III: cortical destruction with soft tissue extension) directly dictates the aggressiveness of the surgical intervention. Current clinical guidelines strongly advocate for extended intralesional curettage with high-speed burring and the use of chemical adjuvants (like phenol) for Grade I and II lesions, reserving en bloc resection primarily for massive Grade III lesions with unsalvageable joint destruction.
The World Health Organization (WHO) Classification of Soft Tissue and Bone Tumors provides the definitive histological categorization used by pathologists and surgeons worldwide. The WHO guidelines are critical for differentiating locally aggressive benign lesions (like infiltrating lipomas or desmoid-type fibromatosis) from low-grade sarcomas, ensuring appropriate oncologic management.
Regarding Giant Cell Tumor of Tendon Sheath (GCTTS), extensive literature reviews and meta-analyses have consistently demonstrated that the most significant risk factor for local recurrence is the failure to achieve complete marginal excision of all satellite nodules. Clinical guidelines therefore strongly emphasize the absolute necessity of performing these excisions under complete tourniquet ischemia and utilizing surgical loupe magnification to ensure meticulous, complete extirpation of the primary mass and any adjacent synovial disease.
