Operative Management of Malignant Soft-Tissue Tumors: A Comprehensive Guide

Key Takeaway
Malignant soft-tissue sarcomas require meticulous surgical planning, wide resection margins, and often multimodal adjuvant therapy. This comprehensive guide details the operative management, biomechanical considerations, and step-by-step surgical approaches for various histological subtypes, including undifferentiated pleomorphic sarcoma, liposarcoma, and synovial sarcoma. Designed for orthopedic oncologists and residents, it emphasizes evidence-based protocols to minimize local recurrence and optimize patient survival.
Comprehensive Introduction and Patho-Epidemiology
The operative management of malignant soft-tissue tumors, collectively known as soft-tissue sarcomas (STS), represents one of the most formidable and complex challenges within the realm of orthopedic oncology. These highly heterogeneous neoplasms originate from embryonic mesoderm and can differentiate into various mesenchymal cell lines, including adipose, fibrous, muscular, and vascular tissues. Representing less than 1% of all adult malignancies, their rarity belies their aggressive clinical behavior and the profound morbidity associated with both the disease process and its surgical extirpation. A rigorous, multidisciplinary approach—integrating orthopedic oncology, medical oncology, radiation oncology, musculoskeletal radiology, and reconstructive microsurgery—is an absolute prerequisite to optimize both oncological survival and functional limb salvage.
Historically, the standard of care for extremity soft-tissue sarcomas was radical amputation, driven by the unacceptably high rates of local recurrence associated with simple excision. However, the modern era of orthopedic oncology has witnessed a paradigm shift toward limb-sparing surgery, primarily facilitated by advancements in multimodal therapy. The synergistic application of wide surgical resection combined with neoadjuvant or adjuvant radiotherapy, and in selected high-risk cases, systemic chemotherapy, has elevated limb salvage rates to over 90% at specialized high-volume sarcoma centers. This evolution underscores the necessity for surgeons to possess an intimate understanding of tumor biology, as the biological grade and histological subtype dictate the aggressiveness of the local resection and the necessity for adjuvant modalities.
Pathologically, soft-tissue sarcomas are stratified using the Fédération Nationale des Centres de Lutte Contre le Cancer (FNCLCC) grading system, which evaluates tumor differentiation, mitotic index, and the extent of tumor necrosis. This three-tiered grading system is the single most critical determinant of metastatic potential and overall survival. High-grade lesions exhibit a profound propensity for hematogenous dissemination, with the pulmonary parenchyma being the primary site of metastasis in over 80% of cases. Conversely, lymphatic spread is classically rare in sarcomas, occurring in fewer than 5% of cases overall, though specific subtypes—namely synovial sarcoma, epithelioid sarcoma, clear cell sarcoma, rhabdomyosarcoma, and angiosarcoma—exhibit a significantly higher predilection for regional lymph node involvement, necessitating meticulous clinical and radiographic nodal staging.
Understanding the specific patho-epidemiology of distinct sarcoma subtypes is vital for tailoring the surgical approach. Undifferentiated Pleomorphic Sarcoma (UPS), formerly classified as Malignant Fibrous Histiocytoma (MFH), remains the most common high-grade soft-tissue sarcoma in adults, typically presenting as a rapidly expanding, deep-seated mass in the proximal lower extremity. Liposarcoma, the second most common variant, presents a spectrum of biological behaviors ranging from the locally aggressive but non-metastasizing atypical lipomatous tumor to the highly lethal pleomorphic liposarcoma. Synovial sarcoma, despite its historical misnomer, rarely arises from intra-articular synovium but rather from periarticular soft tissues in young adults, carrying a pathognomonic t(X;18) chromosomal translocation. Even locally aggressive intermediate tumors, such as desmoid fibromatosis, demand immense surgical respect due to their infiltrative growth patterns and high local recurrence rates, despite lacking metastatic capacity.
Pathological Characteristics of Specific Tumor Subtypes
The literature regarding Malignant Fibrous Histiocytoma (MFH) has undergone a significant paradigm shift over the past two decades. Formerly regarded as the most commonly diagnosed soft-tissue sarcoma in adults, modern immunohistochemistry and molecular diagnostics have led authorities to reclassify it. Today, "MFH" is largely considered a descriptive term for a heterogeneous group of tumors with no distinct line of differentiation, now more accurately termed Undifferentiated Pleomorphic Sarcoma (UPS). Conventionally, this tumor describes a pleomorphic soft-tissue sarcoma exhibiting a storiform histological pattern of growth. It predominantly affects patients aged 50 to 70 years, typically presenting as a large (>5 cm), painless, deep-seated mass, most frequently located in the thigh musculature.
Liposarcoma represents a complex family of adipocytic neoplasms with vastly different clinical trajectories. Well-Differentiated Liposarcoma (Atypical Lipomatous Tumor) is a low-grade, locally aggressive lesion with minimal metastatic potential, often managed with wide excision alone. In stark contrast, Dedifferentiated Liposarcoma represents a high-grade progression from well-differentiated lesions, requiring aggressive multimodal therapy. Myxoid Liposarcoma is unique due to its intermediate-to-high-grade behavior and its highly unusual propensity for extrapulmonary metastases, specifically to the retroperitoneum, contralateral extremity, and osseous spine, mandating whole-spine MRI and abdominal CT during initial staging. Pleomorphic Liposarcoma represents the most aggressive variant, characterized by rapid growth, high metastatic rates, and a generally poor prognosis despite optimal surgical intervention.
Synovial Sarcoma presents unique clinical features compared to other adult soft-tissue sarcomas. It frequently affects young adults (15-40 years) and has a strong predilection for the distal extremities, particularly around the knee, foot, and hand. Clinically, they often present as slow-growing, deceptively small (<5 cm) masses that may be painful, leading to frequent misdiagnosis as benign cysts, neuromas, or tendinopathy. Plain radiographs show amorphous, stippled calcifications within the soft-tissue mass in up to 30% of cases. Genetically, they are characterized by the pathognomonic t(X;18)(p11;q11) chromosomal translocation, resulting in the SYT-SSX fusion transcript.

While technically classified as intermediate (locally aggressive) rather than frankly malignant, desmoid tumors (aggressive fibromatosis) are critical to discuss due to their infiltrative growth and high propensity for local recurrence. They do not metastasize but can cause severe morbidity through local destruction of neurovascular structures and joints. Histologically characterized by a monoclonal proliferation of well-differentiated fibroblasts in a dense collagenous background, they often harbor mutations in the CTNNB1 gene (beta-catenin) or the APC gene (in the context of familial adenomatous polyposis). Surgical resection must be meticulously planned, as positive microscopic margins significantly elevate the risk of aggressive local failure.

Detailed Surgical Anatomy and Biomechanics
A profound mastery of cross-sectional and longitudinal compartmental anatomy is the bedrock upon which successful oncological surgery is built. Soft-tissue sarcomas respect anatomical boundaries in their early and intermediate stages of growth, expanding centrifugally and compressing surrounding normal tissue. This compression creates a "pseudocapsule," a deceptive layer composed of compressed normal cells, inflammatory tissue, and neovascularity. Crucially, this pseudocapsule is not a true anatomical barrier; it is highly permeable and invariably contains microscopic satellite tumor cells. Surgical dissection that violates this reactive zone or the pseudocapsule itself (a marginal or intralesional margin) guarantees microscopic residual disease and a near-certainty of local recurrence.
The concept of anatomical barriers is central to planning a wide resection. Fascia, periosteum, epineurium, and adventitia are dense, collagenous structures that act as robust natural barriers to tumor micro-invasion. A tumor abutting a thick fascial layer can often be safely resected by taking the fascia as the deep margin. Conversely, loose areolar tissue, fat, and skeletal muscle are permissive tissues that offer no resistance to tumor spread. Within a muscular compartment, the tumor can track longitudinally along the muscle fibers far beyond its palpable or radiographically obvious borders. Therefore, when a tumor arises within a muscle belly, the entire muscle from origin to insertion—or at least a substantial longitudinal cuff of normal muscle (typically 3-5 cm)—must be resected to achieve a truly wide margin.


The biomechanical implications of wide soft-tissue resection are significant and must be anticipated during preoperative planning. Excision of an entire muscular compartment, such as the anterior compartment of the thigh (quadriceps) or the posterior compartment of the leg (gastrocnemius-soleus complex), results in profound and predictable functional deficits. The surgeon must evaluate the remaining synergistic muscles and plan for potential tendon transfers or dynamic orthoses. For example, resection of the femoral nerve or the entire quadriceps mechanism will severely compromise knee extension, requiring the patient to lock the knee in hyperextension during the stance phase of gait or utilize a knee-ankle-foot orthosis (KAFO).
Furthermore, the preservation of major neurovascular bundles is a delicate biomechanical and oncological balance. When a tumor is intimately associated with a major nerve (e.g., the sciatic nerve in posterior thigh sarcomas), the surgeon must decide whether the nerve can be safely dissected free by resecting its epineurium (an epineurial dissection) or if it must be sacrificed to achieve a negative margin. Sacrificing the sciatic nerve results in a flail foot and loss of plantar sensation, leading to a high risk of neuropathic ulceration and chronic pain. In such scenarios, the biomechanical reality of a insensate, non-functional limb must be weighed against the oncological necessity, and occasionally, an amputation may provide a superior functional outcome compared to a highly morbid limb-salvage procedure.

Exhaustive Indications and Contraindications
The decision-making process regarding the surgical management of soft-tissue sarcomas is governed by the primary objective of achieving local tumor control while maximizing patient survival and functional capacity. The absolute indication for surgical intervention is the presence of a localized, resectable soft-tissue sarcoma where a wide or radical margin can be achieved without causing unacceptable systemic or local morbidity. Limb-sparing surgery is indicated for the vast majority (>90%) of extremity sarcomas, provided that the tumor can be excised with a continuous cuff of normal tissue and that the resulting limb will possess adequate vascular supply, protective sensation, and useful motor function.
Neoadjuvant and adjuvant therapies are critical adjuncts that modify surgical indications. Preoperative (neoadjuvant) external beam radiation therapy (EBRT) is strongly indicated for large (>5 cm), deep-seated, high-grade sarcomas. Neoadjuvant radiation serves to sterilize the reactive zone, potentially downstage the tumor, and thicken the pseudocapsule, thereby facilitating a safer wide resection and allowing for closer surgical margins near critical neurovascular structures. Adjuvant radiation is indicated when preoperative radiation was not administered and the final pathological margins are close (<1 cm) or microscopically positive (R1 resection). Chemotherapy indications remain controversial in adult STS but are generally considered for young patients with large, high-grade, deep tumors at high risk for systemic micrometastatic disease.
Contraindications to limb salvage surgery, while increasingly rare, are absolute when oncological principles cannot be met. The most definitive contraindication is the inability to achieve negative surgical margins without sacrificing essential neurovascular structures that cannot be reconstructed, rendering the limb non-functional, insensate, and a source of chronic morbidity. Extensive involvement of the major neurovascular bundle (e.g., encasement of the sciatic nerve and superficial femoral artery over a long segment) often necessitates amputation. Other contraindications include massive fungating tumors complicated by intractable secondary infection, severe baseline peripheral vascular disease precluding flap reconstruction or wound healing, and local recurrence following prior maximal radiation therapy where further limb-sparing surgery would result in catastrophic wound failure.
| Clinical Scenario | Indication / Approach | Contraindication to Limb Salvage |
|---|---|---|
| Small (<5cm), Superficial, Low-Grade | Wide surgical excision alone. Adjuvant RT rarely needed if margins are >1cm. | None. Limb salvage is standard of care. |
| Large (>5cm), Deep, High-Grade | Neoadjuvant RT followed by Wide Resection. Consider systemic chemotherapy. | Encasement of major neurovascular bundle precluding R0 resection. |
| Tumor abutting major bone/joint | Wide resection with extra-articular or periosteal/cortical resection. Bone reconstruction. | Extensive intra-articular invasion or massive bone destruction. |
| Involvement of Major Nerve | Epineurial dissection if not encased. Sacrifice nerve if encased, followed by tendon transfers. | Complete loss of protective sensation in weight-bearing surface (e.g., sole of foot) without reconstructive options. |
| Recurrent Tumor Post-EBRT | Radical resection or Amputation. Free tissue transfer mandatory if limb salvage attempted. | Inability to achieve negative margins; severe radiation fibrosis precluding wound healing. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the vanguard of successful sarcoma surgery. The process invariably begins with the initial biopsy, which is arguably the most critical step in the entire management pathway. A poorly executed biopsy can contaminate distinct anatomical compartments or major neurovascular bundles, catastrophically converting a highly resectable tumor into one that mandates amputation. The biopsy must be performed via a small longitudinal incision placed meticulously within the planned definitive surgical excision tract. Transverse incisions are strictly contraindicated, as they require massive sacrifice of normal skin and soft tissue during the definitive resection to clear the contaminated tract. Furthermore, absolute hemostasis must be achieved during the biopsy to prevent the tracking of tumor-laden hematoma into adjacent fascial planes.
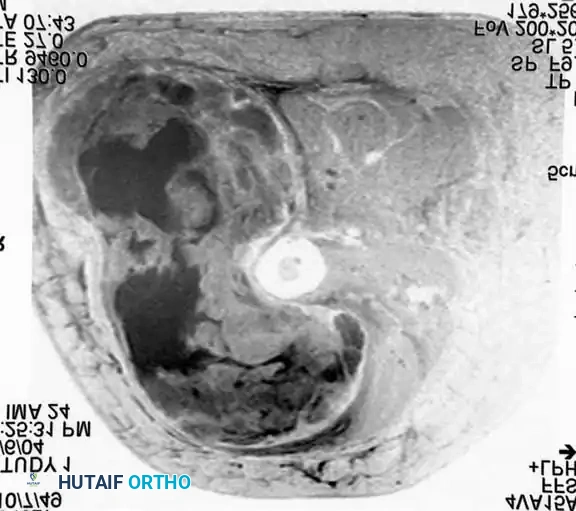
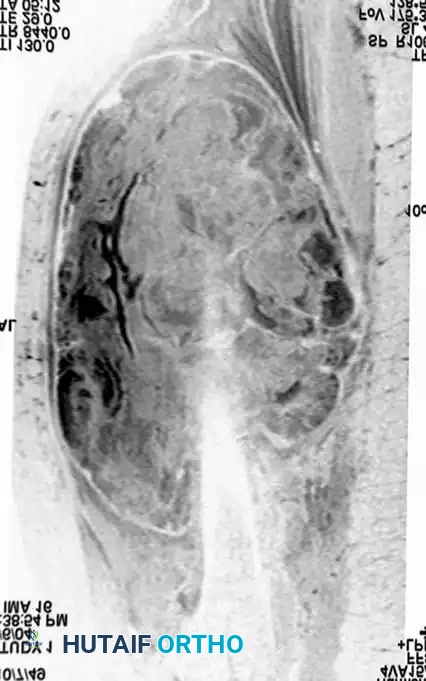
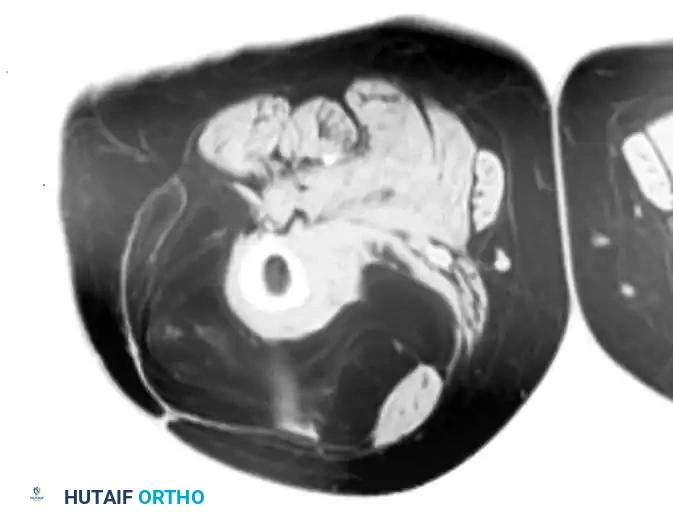
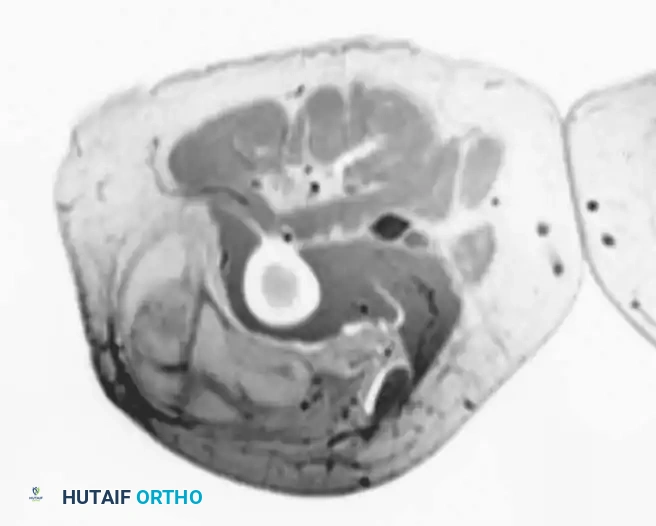
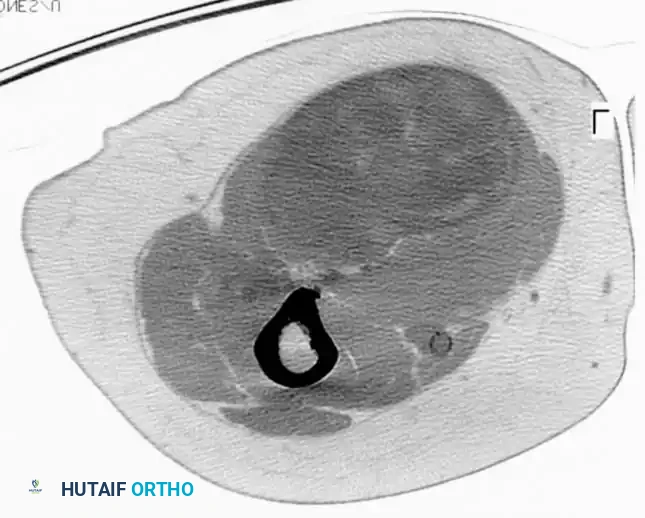
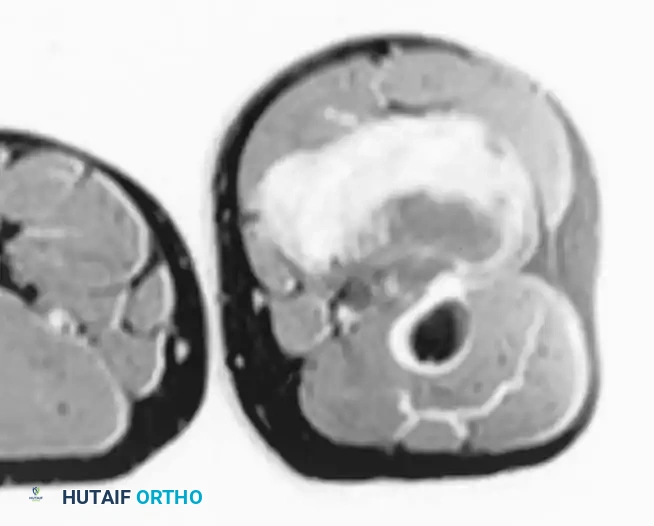
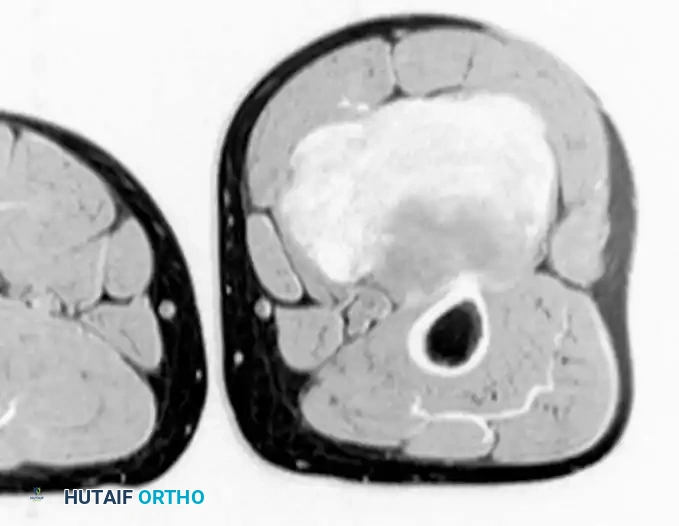
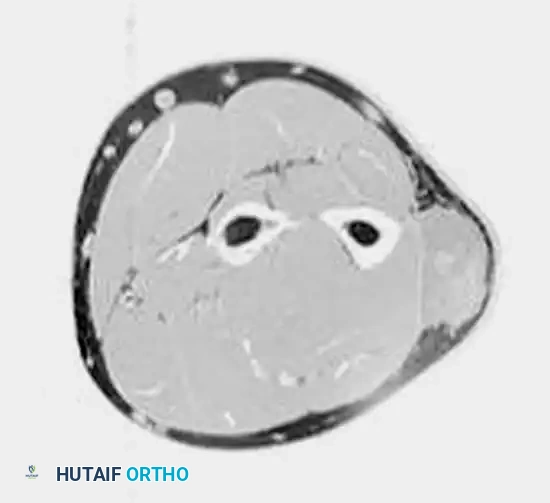
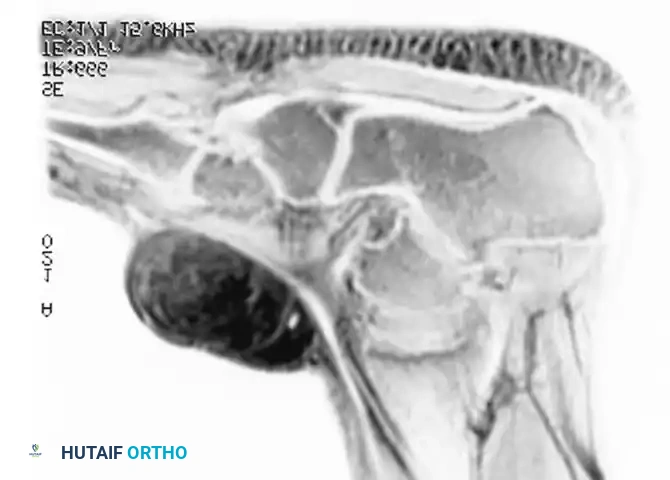
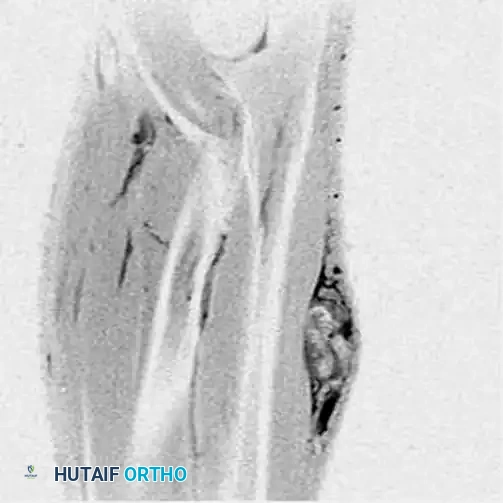
Advanced imaging is the cornerstone of surgical templating. Contrast-enhanced Magnetic Resonance Imaging (MRI) of the entire anatomical compartment (from the joint above to the joint below) is the gold standard. T1-weighted images provide excellent anatomical detail and demonstrate fat content (crucial for liposarcoma diagnosis), while T2-weighted and STIR (Short Tau Inversion Recovery) sequences highlight peritumoral edema, necrosis, and the true extent of the reactive zone. The MRI dictates the surgical margins, identifying exactly which muscles, fascial layers, and neurovascular structures must be sacrificed or preserved. Staging for distant metastasis requires a high-resolution Computed Tomography (CT) scan of the chest without contrast, as the pulmonary capillary bed is the primary filter for hematogenous sarcoma emboli.

Multidisciplinary tumor board discussion is a mandatory component of preoperative planning. The integration of the orthopedic oncologist, musculoskeletal radiologist, and pathologist ensures diagnostic accuracy, while the medical and radiation oncologists coordinate the timing of neoadjuvant therapies. If plastic surgery is required for complex soft-tissue reconstruction (e.g., rotational muscle flaps, pedicled flaps, or microvascular free tissue transfer), their involvement must be secured preoperatively. The surgical template should explicitly define the planned skin incision, the specific muscles to be resected en bloc with the tumor, the anticipated handling of the neurovascular bundle, and the reconstructive strategy.
Patient positioning and intraoperative setup must facilitate access to the entire anatomical compartment and potential flap donor sites. The patient is positioned securely, often utilizing a beanbag or pegboard, to allow for dynamic limb manipulation during the resection. A pneumatic tourniquet is routinely applied proximal to the surgical field to minimize blood loss and enhance visualization of critical structures. However, under no circumstances should the limb be exsanguinated using an Esmarch bandage, as the mechanical compression can force tumor emboli into the systemic circulation. Instead, the limb should be elevated for 3 to 5 minutes to allow for gravity exsanguination prior to tourniquet inflation. The entire limb must be prepped and draped free to allow for intraoperative assessment of distal perfusion and tension-free manipulation.

Step-by-Step Surgical Approach and Fixation Technique
The surgical approach for wide resection of a soft-tissue sarcoma is a meticulously choreographed procedure that prioritizes oncological margins above all else. The skin incision must be carefully designed to incorporate the entire previous biopsy tract, including the skin entry point and the deep fascial violation, within an elliptical island of skin. A minimum margin of 2 to 3 cm of normal, healthy skin is typically maintained around the biopsy site and any superficial tumor extension. Once the skin is incised, full-thickness fasciocutaneous flaps are elevated. It is imperative that these flaps are developed within pristine, normal tissue planes, well away from the tumor's reactive zone. The surgeon must constantly orient themselves relative to the tumor's location as defined by the preoperative MRI, ensuring that the dissection never inadvertently violates the pseudocapsule.
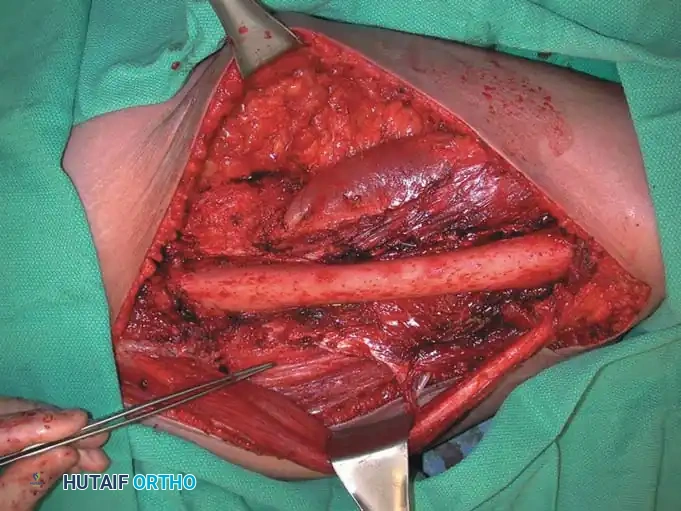
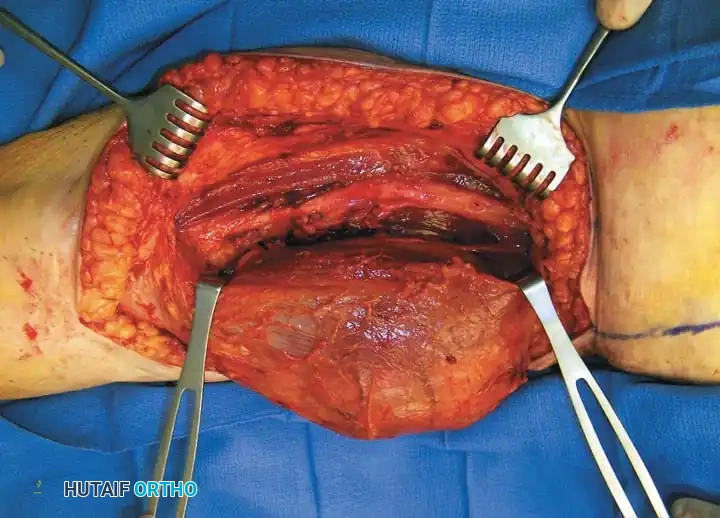
The identification and protection of the major neurovascular bundles constitute the most perilous phase of the dissection. The neurovascular structures must be identified in normal, unadulterated anatomical planes both proximal and distal to the tumor mass. Once identified, they are gently tagged with vessel loops and traced systematically into the zone of resection. If the tumor abuts the neurovascular bundle without encasing it, the surgeon must perform a meticulous epineurial and adventitial dissection. This involves incising the normal epineurium and adventitia proximal to the tumor and peeling these layers away from the nerve and vessels, leaving them attached to the tumor specimen. This technique provides a marginal but anatomically robust barrier, allowing for nerve preservation without compromising oncological safety.



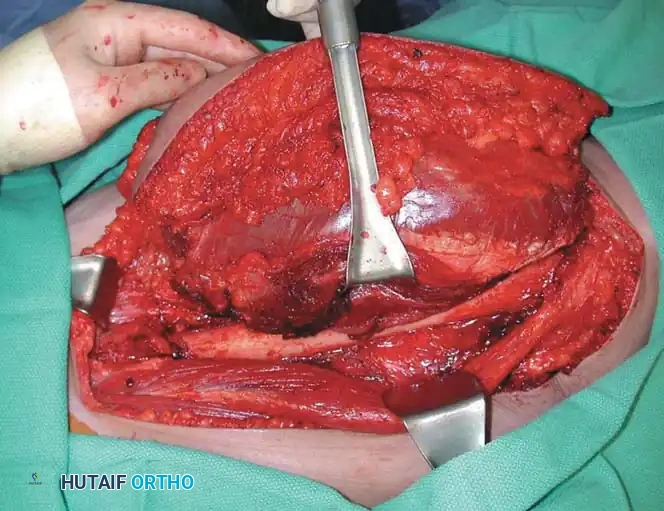
The actual extirpation of the tumor is performed en bloc, meaning the tumor, its pseudocapsule, the reactive zone, and the planned cuff of normal surrounding tissue (muscle, fascia, and fat) are removed as a single, intact specimen. The surgeon must utilize sharp dissection through normal muscle bellies, avoiding the temptation to follow the path of least resistance along the tumor capsule. For tumors like Undifferentiated Pleomorphic Sarcoma (UPS) or high-grade Liposarcoma, the deep margin often necessitates the resection of the underlying muscular fascia or even the outer cortex of adjacent bone if the tumor is deeply seated. Throughout the resection, the surgeon must maintain rigorous hemostasis, as bleeding can obscure tissue planes and increase the risk of microscopic tumor seeding.

Following the removal of the specimen, the tumor bed is thoroughly irrigated with sterile saline or sterile water (which can theoretically cause osmotic lysis of residual tumor cells, though clinical evidence is mixed). The surgeon must then systematically place radiopaque surgical clips (e.g., titanium clips) at the superior, inferior, medial, lateral, superficial, and deep margins of the resection bed. These clips serve as critical fiducial markers for the radiation oncologist, allowing for precise targeting of the postoperative radiation field while minimizing collateral damage to surrounding normal tissues. Finally, the reconstruction phase commences. If primary closure cannot be achieved without excessive tension, or if critical structures (nerves, vessels, bone) are exposed, immediate soft-tissue reconstruction via local rotational flaps (e.g., gastrocnemius or soleus flaps) or microvascular free tissue transfer (e.g., anterolateral thigh or latissimus dorsi flaps) is mandatory to ensure wound healing and allow for timely initiation of adjuvant therapies.

Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and comprehensive preoperative planning, the operative management of soft-tissue sarcomas carries a substantial risk of complications, driven by the extensive nature of the resections and the deleterious effects of neoadjuvant radiation on tissue healing. Wound complications are the most frequent source of postoperative morbidity, particularly in the lower extremity. The incidence of major wound complications—defined as those requiring secondary surgical intervention, prolonged negative pressure wound therapy, or resulting in a delay of adjuvant therapy—ranges from 25% to 35% in patients receiving preoperative radiation. Tissue necrosis, dehiscence, and deep surgical site infections are exacerbated by radiation-induced endarteritis, which severely compromises the microvascular supply to the skin flaps.
Local recurrence is a devastating oncological complication that signifies a failure of local control. The incidence of local recurrence following wide resection and radiation therapy is generally maintained below 10% in modern high-volume centers. However, this rate increases significantly in the presence of positive microscopic margins (R1 resection), high histological grade, and specific histologies such as aggressive fibromatosis (desmoid tumors) or epithelioid sarcoma. Salvage management for local recurrence is highly complex and depends on the patient's prior treatments. If the patient has not received prior radiation, re-excision with adjuvant radiotherapy is the standard approach. If the patient has already received maximal therapeutic doses of radiation, further limb-sparing surgery requires radical re-excision coupled with vascularized free tissue transfer to bring healthy, non-irradiated tissue into the defect. Often, amputation becomes the most reliable salvage option to prevent further fungation and intractable pain.
Systemic metastasis remains the primary cause of mortality in sarcoma patients. High-grade sarcomas, particularly large (>5 cm) and deep lesions, have a 40% to 50% risk of distant metastasis, predominantly to the lungs. Routine postoperative surveillance with high-resolution chest CT is mandatory. The management of pulmonary metastases involves a multidisciplinary approach; isolated, resectable pulmonary nodules in a patient with a controlled primary site may be managed with pulmonary metastasectomy, which can offer a distinct survival advantage. Unresectable metastatic disease is managed palliatively with systemic chemotherapy, targeted therapies, or enrollment in clinical trials, though the overall prognosis in this setting remains grim.
| Complication Category | Specific Complication | Estimated Incidence | Salvage / Management Strategy |
|---|---|---|---|
| Wound / Soft Tissue | Major Wound Dehiscence / Necrosis | 25% - 35% (with neoadjuvant RT) | Surgical debridement, Negative Pressure Wound Therapy (NPWT), Flap coverage (rotational or free flap). Delay adjuvant chemo until healed. |
| Infectious | Deep Surgical Site Infection | 10% - 15% | Aggressive I&D, deep tissue cultures, targeted IV antibiotics, hardware/clip retention if possible, flap coverage if dead space exists. |
| Oncological | Local Recurrence | <10% (with R0 margin + RT) | Restaging MRI/CT. Re-excision with wide margins + free flap. Amputation if neurovascular bundle involved or prior maximal RT precludes healing. |
| Oncological | Pulmonary Metastasis | 40% - 50% (High-grade tumors |
