Distal Thigh Schwannoma: A Comprehensive Clinical and MRI Diagnosis Case Study
Key Takeaway
Schwannomas are typically diagnosed through a combination of patient history (progressive mass, neurological symptoms), clinical examination (Tinel's sign, diminished sensation), and characteristic MRI findings. MRI often reveals a well-circumscribed, enhancing mass with specific 'target sign' and 'split fat sign,' differentiating it from other soft tissue tumors and confirming its nerve sheath origin.
A 48-year-old male presents with a two-year history of a slow-growing, painful mass in the posteromedial thigh. On examination, the mass has specific mechanical properties regarding its mobility. How would you describe the physical examination findings, and what do they imply regarding the nature of the lesion?
Candidate: The mass is mobile side-to-side but restricted longitudinally. This suggests it is attached to a nerve. A positive Tinel's sign confirms it's a peripheral nerve sheath tumor, likely a schwannoma or neurofibroma.
Failure to link the biomechanical findings to the anatomy. A candidate who simply states "it's a nerve tumor" without articulating the specific "transverse mobility vs. longitudinal tethering" sign misses the core diagnostic marker that separates nerve sheath tumors from other soft tissue masses (like lipomas or sarcomas).
I would perform a focused examination looking for the pathognomonic sign: the mass will be mobile perpendicular to the limb's long axis but restricted longitudinally, due to tethering by the parent nerve. Combined with a positive Tinel's sign (radiating paresthesias), this clinically localizes the lesion to a major peripheral nerve. I would then check the distal neurovascular status—specifically mapping the sensory deficit—and ensure there are no signs of NF1, such as café-au-lait spots, to help differentiate between a solitary schwannoma and a neurofibroma.
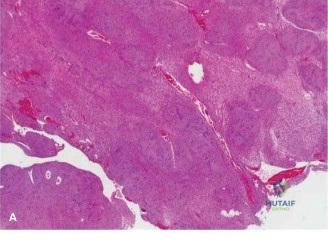
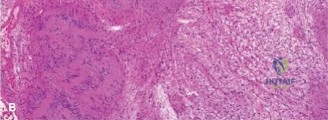
You have reviewed the MRI. It shows a T2 hyperintense mass with a 'target sign' and a 'split fat sign'. What is the significance of these findings, and how do they influence your decision-making regarding surgery?
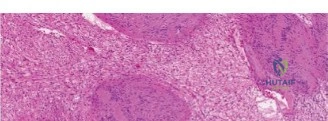
Candidate: These signs are classic for a benign schwannoma. The target sign reflects Antoni A and B tissue distribution. The split fat sign shows it's well-encapsulated. This means I can offer marginal excision or enucleation, which is safer than attempting a radical resection.
Focusing only on the MRI signs without mentioning the surgical implication. Examiners look for the candidate to distinguish between schwannoma (which can be enucleated because it is eccentric/encapsulated) and neurofibroma (which is often interstitial and may require sacrifice of nerve fascicles).
The 'target sign' and 'split fat sign' are highly suggestive of a benign peripheral nerve sheath tumor (BPNST), specifically a schwannoma. Surgically, the distinction is vital: schwannomas are encapsulated and arise eccentrically, allowing for microsurgical enucleation while sparing functional fascicles. In contrast, neurofibromas grow interstitially and often necessitate segmental resection of the nerve. Given these imaging findings, I would counsel the patient on a planned microsurgical enucleation under neuromonitoring, while consenting for potential transient or permanent sensory/motor deficits.
During the procedure, you have exposed the mass. How do you technically ensure the safety of the nerve during excision, and what is the role of intraoperative neuromonitoring (IONM) in this specific case?
Candidate: I would use magnifying loupes or a microscope. I'd identify the functional fascicles, stimulate them with a handheld nerve stimulator, and perform an epineurotomy in the 'safe zone'. IONM is essential to confirm I haven't damaged the nerve.
Neglecting the anesthesia requirements. A candidate who forgets to mention that muscle relaxants must be avoided or reversed before neuromonitoring will fail the practical/technical safety component of the viva.
Safety is paramount: I would ensure total avoidance of long-acting neuromuscular blockers by the anaesthetist. Intraoperatively, I would utilize a handheld stimulator (e.g., 0.5-1.0 mA) to map the fascicles draped over the mass. Once the 'safe zone' is identified, I would perform a longitudinal epineurotomy, use micro-dissection to separate the tumor capsule, and achieve enucleation. IONM provides real-time feedback—specifically somatosensory evoked potentials and triggered EMG—to confirm functional continuity throughout the procedure and immediately post-enucleation.
