Endoscopic Carpal Tunnel Release: Single-Incision Agee Technique
Key Takeaway
Endoscopic carpal tunnel release (ECTR) via a single-incision approach offers reliable median nerve decompression with minimized palmar morbidity. The Agee technique utilizes a proximal incision, specialized blade assembly, and precise trajectory aligned with the ring finger to divide the transverse carpal ligament from within. By releasing the distal half first, surgeons prevent palmar fat herniation from obscuring the endoscopic view, ensuring a safe, complete release and accelerated postoperative rehabilitation.
Comprehensive Introduction and Patho-Epidemiology
Carpal tunnel syndrome (CTS) stands as the most ubiquitous compressive neuropathy of the upper extremity, affecting approximately one to three percent of the general population and representing a significant source of occupational disability and healthcare expenditure. The pathophysiology of CTS is fundamentally driven by a mismatch between the volume of the carpal tunnel and its contents, leading to elevated interstitial pressures. Normal resting carpal tunnel pressures range from 2 to 10 mmHg; however, in patients with CTS, these pressures routinely exceed 30 mmHg, a threshold known to impede epineural venous return. This venous congestion initiates a deleterious cascade of endoneurial edema, localized ischemia, and eventual fibrosis of the median nerve. Prolonged compression ultimately results in axonal degeneration, manifesting clinically as progressive sensory deficits, debilitating nocturnal pain, and eventual thenar motor atrophy.
While open carpal tunnel release (OCTR) has historically served as the gold standard for surgical decompression, Endoscopic Carpal Tunnel Release (ECTR) has revolutionized the operative management of this condition since its inception in the late 1980s and early 1990s. The conceptual framework underpinning ECTR relies on the precise division of the transverse carpal ligament (TCL) from within the carpal vault, thereby preserving the overlying anatomical structures. This includes the palmar skin, subcutaneous adipose tissue, the palmar aponeurosis, and the intricate superficial neural network. By circumventing a direct palmar incision, ECTR fundamentally alters the postoperative recovery trajectory.
The clinical advantages of this minimally invasive approach are profound and well-documented in the orthopedic literature. Preservation of the superficial palmar structures significantly mitigates the incidence and severity of postoperative pillar pain—a common and notoriously recalcitrant complication following OCTR. Furthermore, the absence of a palmar scar eliminates scar tenderness and hyperesthesia during grip activities. Consequently, patients undergoing ECTR consistently demonstrate a statistically significant acceleration in the return to activities of daily living and occupational duties, particularly those involving heavy manual labor or repetitive hand use.
The single-incision technique, pioneered and popularized by John M. Agee, represents a pinnacle of this endoscopic evolution. Utilizing a proprietary pistol-grip blade assembly introduced through a single proximal portal, the Agee technique allows for safe, retrograde division of the TCL under direct video-endoscopic visualization. However, this approach is technically demanding and possesses a steep learning curve. It necessitates an uncompromising, three-dimensional spatial awareness of the carpal vault, a rigorous understanding of anatomical variants, and strict adherence to sequential, protocolized surgical steps to avert catastrophic iatrogenic injuries to the median nerve, the ulnar nerve, and the superficial palmar arch.
Detailed Surgical Anatomy and Biomechanics
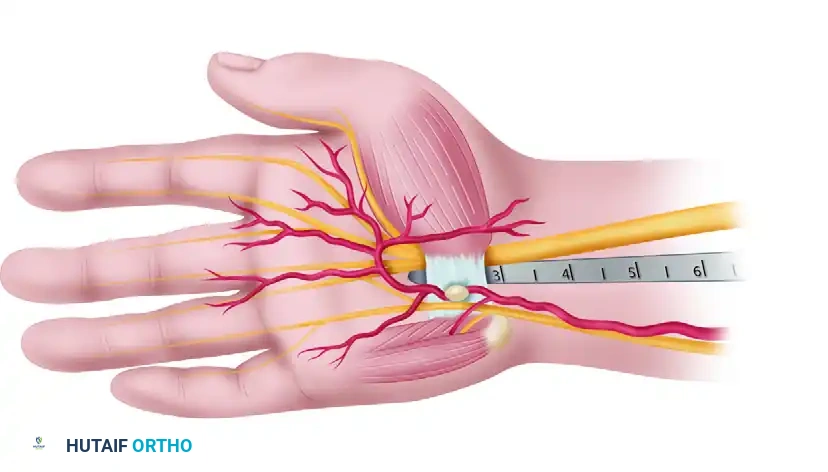
A profound, masterful understanding of the carpal tunnel's three-dimensional osteofibrous anatomy is an absolute prerequisite for the safe and efficacious execution of an endoscopic release. The carpal tunnel is a rigid, non-expansile canal bounded dorsally by the concave arch of the carpal bones and volarly by the unyielding transverse carpal ligament. The radial border is defined by the scaphoid tuberosity and the crest of the trapezium, while the ulnar border is anchored by the pisiform and the hook of the hamate. The TCL itself is a robust, fibrous structure, typically measuring 1 to 2 millimeters in thickness and 2 to 3 centimeters in width, serving as a critical retinacular pulley for the extrinsic flexor tendons.
Within this confined space reside ten critical structures: the four tendons of the flexor digitorum superficialis (FDS), the four tendons of the flexor digitorum profundus (FDP), the flexor pollicis longus (FPL) tendon, and the median nerve. The median nerve typically courses superficially and radially within the tunnel, situated immediately deep to the TCL. However, the surgeon must remain acutely vigilant regarding anatomical variations, most notably detailed by the Lanz classification. These variations include a high bifurcation of the median nerve, an accessory distal branch, and most critically, a transligamentous or subligamentous trajectory of the recurrent motor branch. Failure to recognize these variants during endoscopic instrumentation can result in devastating motor deficits.
The foundational tenet of safe endoscopic carpal tunnel release is strict adherence to the anatomical "safe zone." This safe zone for blade elevation and ligament division is a highly specific, three-dimensional triangular corridor. Its boundaries are defined radially by the ulnar border of the median nerve (specifically, its common digital branch to the long and ring finger web space), ulnarly by the hook of the hamate and Guyon’s canal, and distally by the superficial palmar arch. By maintaining the endoscopic trajectory strictly within the ulnar half of the carpal tunnel, the surgeon effectively isolates the instrumentation from the median nerve and its recurrent motor branch, which typically arborizes radially.
Biomechanically, the transverse carpal ligament is not merely a passive constraint; it contributes to the structural integrity of the carpal arch and prevents volar bowstringing of the flexor tendons during forceful wrist flexion. While division of the TCL inevitably alters these biomechanics—often resulting in a slight widening of the carpal arch—the preservation of the overlying palmar fascia in ECTR provides a secondary restraint. This preserved fascial layer helps to limit postoperative tendon bowstringing and maintains a more physiological transmission of forces across the wrist joint compared to the complete disruption inherent in an open release.
Exhaustive Indications and Contraindications
The decision to proceed with Endoscopic Carpal Tunnel Release must be predicated on a meticulous clinical evaluation, corroborated by objective electrodiagnostic testing, and tempered by a thorough assessment of the patient's specific anatomical and medical profile. The primary indication for ECTR is symptomatic carpal tunnel syndrome that has proven refractory to a comprehensive regimen of conservative management. This typically includes a minimum of six to twelve weeks of nocturnal splinting, nonsteroidal anti-inflammatory drugs (NSAIDs), activity modification, and potentially corticosteroid injections.
Patients presenting with severe clinical manifestations—such as profound thenar atrophy, fixed sensory deficits (two-point discrimination greater than 5mm), or severe, unrelenting nocturnal pain that disrupts sleep architecture—are candidates for expedited surgical intervention. Electrodiagnostic studies (EMG/NCS) are paramount in confirming the diagnosis and stratifying disease severity. Prolonged distal sensory latencies (typically > 3.5 ms) and distal motor latencies (> 4.5 ms), coupled with decreased conduction velocities across the wrist, provide objective justification for surgical decompression. ECTR is particularly advantageous for patients requiring bilateral simultaneous releases, as the minimized morbidity allows for a significantly more manageable early postoperative recovery phase.
However, ECTR is not universally applicable, and recognizing its contraindications is critical to avoiding devastating surgical misadventures. Absolute contraindications include the presence of space-occupying lesions within the carpal tunnel (e.g., ganglion cysts, lipomas, schwannomas, or anomalous muscle bellies), which require direct open visualization for safe extirpation. Previous operative interventions in the carpal tunnel or significant traumatic scarring of the volar wrist represent absolute contraindications due to the obliteration of normal tissue planes and the high risk of iatrogenic nerve laceration. Relative contraindications encompass severe inflammatory tenosynovitis (such as in rheumatoid arthritis), which may necessitate an open concomitant tenosynovectomy, and profound wrist stiffness that precludes the necessary extension required for safe trocar insertion.
| Classification | Condition/Factor | Rationale for Contraindication/Consideration |
|---|---|---|
| Absolute Contraindication | Prior Carpal Tunnel Surgery | Obliterated tissue planes; severe risk of median nerve laceration. |
| Absolute Contraindication | Space-Occupying Lesions (Tumor/Cyst) | Requires open excision; blind endoscopic passage risks incomplete removal or neurovascular injury. |
| Absolute Contraindication | Anatomical Deformity (e.g., severe distal radius malunion) | Distorted carpal vault anatomy prevents safe, linear passage of the endoscopic trocar. |
| Relative Contraindication | Rheumatoid Arthritis / Severe Tenosynovitis | May require open flexor tenosynovectomy; severe synovium obscures endoscopic visualization ("snowstorm effect"). |
| Relative Contraindication | Advanced Thenar Atrophy | Open release may be preferred to directly inspect the motor branch or perform a simultaneous opponensplasty. |
| Relative Contraindication | Inability to Extend the Wrist | Limits the necessary trajectory angle for the Agee device, forcing the blade too close to the median nerve. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative preparation is the vanguard against intraoperative complications in endoscopic surgery. The clinical evaluation must include a detailed assessment of the cervical spine to rule out double-crush syndrome, as well as a precise mapping of the patient's sensory deficits and motor function. While routine advanced imaging is not mandatory for classic CTS, high-resolution ultrasonography or magnetic resonance imaging (MRI) is increasingly utilized in complex cases to template the cross-sectional area of the median nerve, identify anomalous vessels (such as a persistent median artery), or detect subclinical space-occupying lesions.
Operating room ergonomics and the spatial arrangement of the surgical team are critical determinants of a successful ECTR. The surgeon must ascertain that the setup provides an unobstructed, direct line of sight to the high-definition television monitor. The monitor should be positioned directly across the operating table, aligning the surgeon’s visual axis with their hands. This collinear arrangement eliminates cervical strain and optimizes the fine hand-eye coordination required to manipulate the endoscopic blade assembly within a confined space. The endoscopic tower must be tested for white balance, focus, and light intensity prior to the induction of anesthesia.
The choice of anesthesia warrants careful consideration and carries specific implications for the endoscopic technique. General anesthesia or regional anesthesia (such as an axillary or supraclavicular brachial plexus block) are the preferred modalities, providing profound analgesia and complete muscle relaxation. While the Wide Awake Local Anesthesia No Tourniquet (WALANT) technique has gained immense popularity for many hand procedures, it presents a distinct hazard in ECTR. The localized infiltration of tumescent fluid alters the delicate tissue planes within the carpal tunnel and frequently leaks into the endoscopic field, severely clouding the lens and compromising the pristine visualization required for a safe release.
Patient positioning must facilitate unhindered manipulation of the upper extremity. The patient is placed supine with the operative arm extended on a radiolucent hand table. A pneumatic tourniquet is applied over adequate cast padding on the proximal arm. Prior to inflation, the limb is meticulously exsanguinated using an Esmarch bandage to ensure a bloodless surgical field, which is an absolute necessity for endoscopic clarity. The arm is prepped and draped in a standard sterile fashion, leaving the extremity exposed distal to the tourniquet. A rolled towel or specialized wrist positioner is placed under the dorsal wrist to maintain slight extension, optimizing the trajectory for the introduction of the endoscopic instruments.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Superficial Dissection
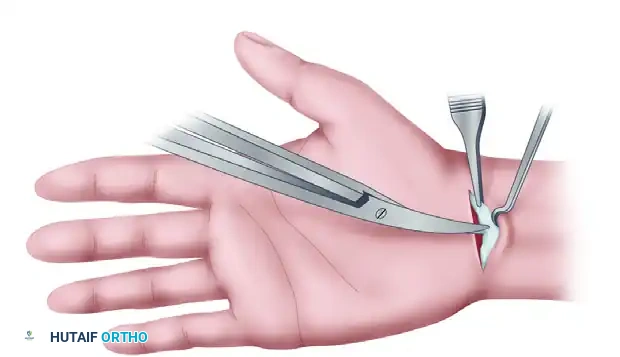
The Agee single-incision technique begins with precise anatomical landmarking. In a patient with two or more volar wrist flexion creases, the most proximal crease is identified as the primary landmark. A transverse incision, measuring approximately 1.5 to 2.0 centimeters, is placed exactly within this crease, centered over the interval between the flexor carpi radialis (FCR) and the flexor carpi ulnaris (FCU) tendons. This specific placement is designed to minimize postoperative scarring and avoid the critical superficial nerves.
Following the skin incision, dissection proceeds through the subcutaneous adipose tissue. It is imperative that all dissection at this level is performed longitudinally using blunt instruments, such as tenotomy scissors or a small hemostat. Longitudinal spreading parallel to the axis of the forearm prevents inadvertent transection of the palmar cutaneous branch of the median nerve (PCBMN)—which typically lies radial to the axis of the ring finger—and the medial antebrachial cutaneous nerve branches. Dissection is carried down until the glistening, transverse fibers of the antebrachial (forearm) fascia are clearly exposed.
Fascial Flap Preparation and Synovial Clearance
Once the antebrachial fascia is exposed, a U-shaped, distally based fascial flap is designed and incised. This flap is carefully elevated and retracted distally (palmarward) using a fine stay suture or a small skin hook. The creation of this flap is a pivotal step; it not only facilitates the smooth introduction of the blunt obturator and the endoscopic blade assembly but also prevents the proximal fascia from rolling inward and obstructing the optical cavity.
Retraction of the fascial flap reveals the proximal entrance to the carpal tunnel, appearing as a "mouthlike" opening. Before introducing the optics, the surgeon must address the tenosynovium lining the deep surface of the transverse carpal ligament. A specialized, blunt-tipped synovium elevator is introduced through the portal. By applying firm, upward pressure against the deep surface of the TCL, the surgeon scrapes the hypertrophied synovium distally. Failure to adequately clear this synovial tissue will result in a "snowstorm" effect on the monitor—a chaotic swirl of tissue fragments and fluid that critically obscures the ligamentous fibers and renders the release unsafe.
Endoscopic Trajectory and Insertion
With the synovial bed cleared, the patient's wrist is positioned in slight extension over the rolled towel. The endoscopic blade assembly, with the blade fully retracted, is introduced into the carpal tunnel. The trajectory of insertion is the most critical safeguard against iatrogenic nerve injury.
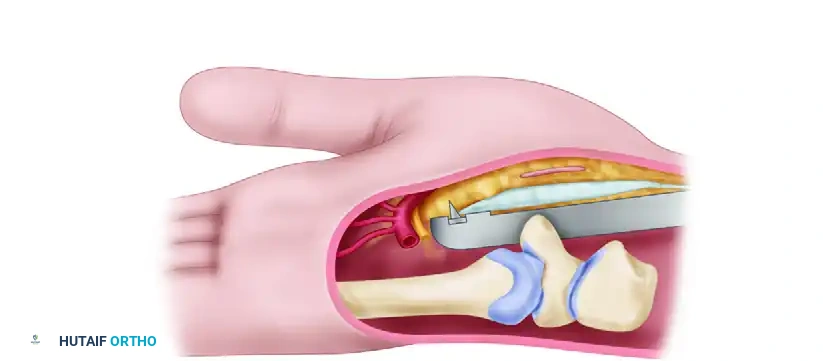
The surgeon must adhere to the "Critical Trajectory Rule": the instrument must be aligned with the longitudinal axis of the ring finger. As the device is advanced, the surgeon must actively "hug" the hook of the hamate, maintaining the instrument strictly on the ulnar side of the carpal vault. Simultaneously, the viewing window must be pressed snugly against the deep surface of the TCL. This ulnar-biased, dorsally elevated trajectory ensures the instrument remains within the safe zone, far removed from the median nerve and its recurrent motor branch. Several proximal-to-distal passes are made to clearly define the transverse fibers of the ligament and identify the distal edge where the fat of the superficial palmar arch begins.
Division of the Transverse Carpal Ligament
The precise identification of the distal margin of the TCL is mandatory before any cutting occurs. The surgeon must utilize a triad of verification methods to confirm this landmark. First, the Video Picture must clearly show the transition from the stark, white, transverse fibers of the ligament to the yellow, lobulated fat of the palm. Second, Ballottement is performed by palpating the tip of the instrument through the palmar skin; the tip should be felt just proximal to the superficial palmar arch. Third, Transillumination of the endoscopic light through the palmar skin provides a visual map of the instrument's distal extent.
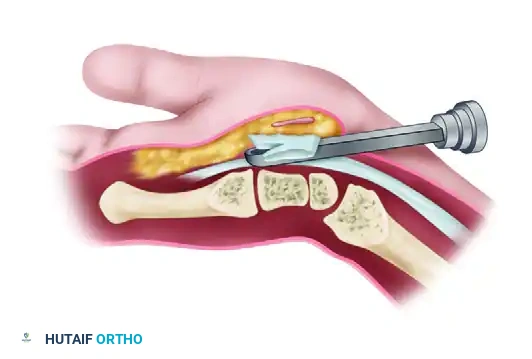
Once the distal edge is unequivocally identified, the blade assembly is positioned appropriately. The blade is partially elevated to touch the distal end of the ligament, judging the precise entry point. The blade is then fully elevated, and the device is smoothly withdrawn proximally, incising the ligament from inside out.
To avoid a common technical pitfall, the release should be performed in two stages. If the proximal half of the ligament is divided first, adipose tissue from the proximal palm and subcutaneous layers will prolapse into the tunnel, coating the endoscopic lens with an impenetrable oil layer. Therefore, the surgeon must first release only the distal one-half to two-thirds of the ligament.
After this initial distal cut, the instrument is reinserted through the now-unobstructed path. The distal division is verified, and the proximal remainder of the ligament is subsequently divided with a final, controlled proximal pass of the elevated blade.
Verification of Complete Decompression
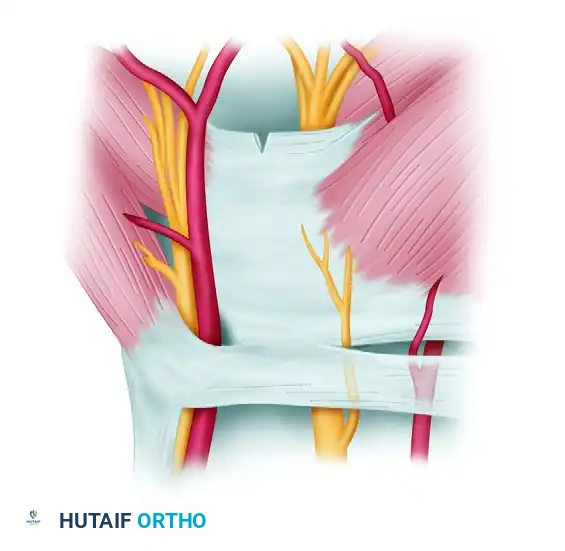
A partial release is the most frequent cause of persistent postoperative symptoms; thus, rigorous endoscopic verification of complete division is imperative. Through the endoscope, a partially divided ligament will present as a V-shaped defect, indicating that the superficial fibers remain intact.
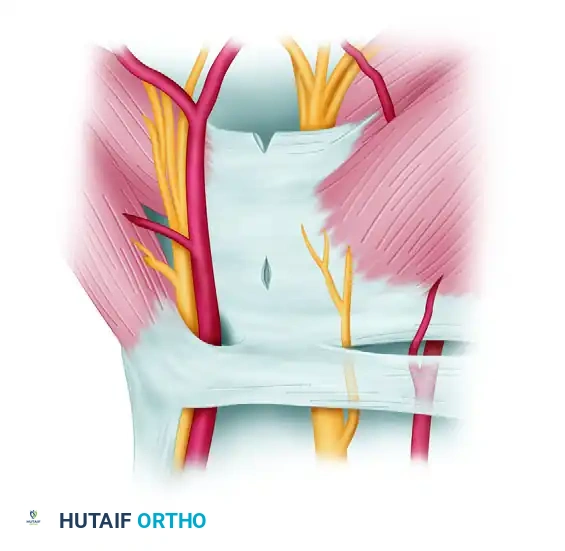
As subsequent passes complete the division, this V-shaped cleft will abruptly transition into a wide, trapezoidal defect. This widening occurs as the two halves of the completely severed ligament spring apart under the resting tension of the carpal arch.

Through this trapezoidal window, the surgeon should directly visualize the longitudinal fibers of the palmar fascia, intermingled with subcutaneous fat and occasionally palmaris brevis muscle fibers. By pressing firmly on the palmar skin, these superficial structures can be forced to protrude into the tunnel, confirming the absence of intervening ligamentous tissue. Furthermore, rotating the blade assembly approximately 20 degrees radially and ulnarly should cause the cut edges of the ligament to abruptly "flop" into the viewing window.

Finally, manual palpation over the palmar skin while moving the blade assembly should reveal independent motion between the divided TCL and the superficial palmar fascia, definitively confirming a complete structural release.
Proximal Fascial Release and Closure
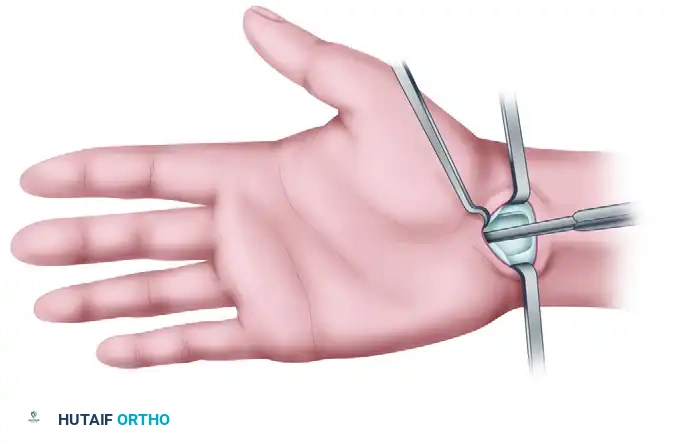
To ensure absolutely complete decompression of the median nerve, the proximal antebrachial fascia must also be released. This step is not performed endoscopically but rather under direct, open vision through the proximal incision. Tenotomy scissors are carefully inserted into the proximal wound, directing the tips proximally and superficially.

Small right-angle retractors (such as Senn retractors) are utilized to elevate the skin and subcutaneous tissues, providing direct visual access to the fascia. The fascia is divided for several centimeters proximally, taking extreme care to avoid the median nerve, which lies immediately deep to this layer.

Upon completion of the release, the tourniquet is deflated, and meticulous hemostasis is achieved. The wound is copiously irrigated with sterile saline to remove any debris or blood clots. The skin incision is closed using either a running subcuticular suture or simple interrupted non-absorbable sutures (e.g., 4-0 nylon). A sterile, nonadhering dressing is applied, followed by a soft, bulky compressive wrap.
Alternative Approach: Two-Portal (Chow) Technique
While the Agee single-incision technique is highly favored for its minimization of palmar scarring, the Chow two-portal technique remains a historically significant and viable alternative. This method establishes a working slotted trocar through the carpal tunnel, utilizing both a proximal entry portal and a distal exit portal.
The proximal entry portal is established in a manner nearly identical to the single-incision technique, located just proximal to the distal wrist flexion crease.
The distal exit portal requires meticulous anatomical mapping. It is typically located in the mid-palm, positioned carefully at the intersection of the cardinal line (drawn from the apex of the first web space across the palm) and a longitudinal line extending from the radial border of the ring finger. This placement is designed to safely bypass the superficial palmar arch.
A blunt, slotted trocar is passed blindly but carefully from the proximal portal to the distal portal, exiting through the palmar incision. The endoscope is then introduced into the trocar. By rotating the trocar, the transverse fibers of the carpal ligament are identified through the open slot in the trocar wall.
The ligament division in the Chow technique is performed using specialized, interchangeable knives introduced alongside the endoscope. Initially, a probe knife is utilized to cut from distal to proximal, releasing the most distal aspect of the carpal ligament.

Subsequently, a retrograde triangle knife is inserted to complete the division of the midsection and the proximal portion of the ligament.
While the Chow technique provides excellent visualization through the slotted trocar, the requirement of a palmar incision inherently increases the risk of postoperative palmar scar tenderness compared to the Agee single-incision approach.
Complications, Incidence Rates, and Salvage Management
Despite the high success rates and rapid recovery associated with ECTR, the procedure is unforgiving of technical errors. The learning curve is notoriously steep, and complications, when they occur, can be functionally devastating for the patient and medicolegally perilous for the surgeon. A comprehensive understanding of potential pitfalls and their immediate salvage management is mandatory.
The most frequently encountered complication following ECTR is an incomplete release of the transverse carpal ligament, with reported incidence rates ranging from 1% to 3% in large series. This typically occurs at the extreme distal margin of the TCL, where the surgeon may prematurely terminate the cut to avoid the superficial palmar arch, or proximally at the antebrachial fascia. Patients present with persistent or rapidly recurrent CTS symptoms. Diagnosis is confirmed clinically and via repeat electrodiagnostic studies. The salvage management for an incomplete release is a definitive open carpal tunnel exploration and completion of the release under direct visualization.
Nerve injuries represent the most catastrophic complications of ECTR. Laceration of the median nerve or its recurrent motor branch occurs in less than 0.5% of cases but results in profound sensory and motor deficits. This typically stems from a failure to maintain the ulnar trajectory (hugging the hamate) or from unrecognized anatomical variants (e.g., a transligamentous motor branch). Ulnar nerve injury, though exceedingly rare, can occur if the blade is advanced too far ulnarly into Guyon's canal. If a nerve laceration is recognized intraoperatively, the endoscopic procedure must be immediately converted to an open approach, and formal microsurgical epineural repair must be performed by a surgeon proficient in peripheral nerve reconstruction.
Vascular injuries, specifically to the superficial palmar arch, occur if the endoscopic blade is advanced excessively distal to the TCL. This is entirely preventable by strict adherence to the triad of distal verification (video, ballottement, transillumination). Intraoperative arterial hemorrhage will immediately obscure the endoscopic field. The surgeon must immediately apply direct, firm palmar pressure, inflate the tourniquet (if deflated), and convert to an open palmar incision to
