Surgical Management of Central Slip Ruptures and Boutonnière Deformity
Key Takeaway
The surgical management of central slip ruptures requires a profound understanding of extensor mechanism biomechanics. This comprehensive guide details the operative techniques for both acute injuries and chronic Boutonnière deformities. Key procedures include primary anatomic repair, Fowler/Dolphin tenotomy for supple deformities, and the Littler dorsal shift reconstruction. Precise surgical execution, combined with meticulous postoperative rehabilitation such as the Evans short-arc motion protocol, is essential for restoring proximal interphalangeal joint kinematics and preventing long-term functional impairment.
Comprehensive Introduction and Patho-Epidemiology
The extensor mechanism of the human digit represents a highly complex, finely balanced kinematic chain that relies on a delicate interplay between intrinsic and extrinsic muscular forces, precise tendinous insertions, and meticulously calibrated retinacular restraints. Disruption of the central slip of the extensor expansion over the proximal interphalangeal (PIP) joint initiates a predictable, progressive, and highly debilitating cascade of biomechanical failures. This structural collapse is clinically recognized as the Boutonnière (or buttonhole) deformity. While acute injuries may present simply as a localized loss of extension, the natural history of an untreated central slip rupture is a relentless progression toward a fixed, rigid deformity that severely compromises the global function of the hand.
Epidemiologically, central slip injuries are frequently encountered in both the acute trauma setting and as a sequela of chronic inflammatory arthropathies. In the traumatic cohort, these injuries most commonly result from forced flexion of an actively extended PIP joint—a mechanism ubiquitous in ball-handling sports such as basketball and volleyball. Volar dislocations of the PIP joint, though less common than their dorsal counterparts, almost universally result in avulsion or rupture of the central slip and must be treated with a high index of suspicion. Open lacerations over the dorsal PIP joint, often resulting from occupational hazards or altercations, represent another significant etiology. Conversely, in the rheumatoid arthritis population, the pathogenesis is driven by chronic synovial proliferation within the PIP joint. This relentless synovitis mechanically distends the joint capsule, enzymatically degrades the central slip insertion, and stretches the secondary stabilizing structures, leading to an insidious, atraumatic onset of the deformity.
The pathogenesis of the true Boutonnière deformity is fundamentally a time-dependent phenomenon. Initially, the loss of central slip continuity results merely in an extensor lag at the PIP joint; the digit may still appear relatively normal at rest. However, if left untreated, the triangular ligament over the dorsum of the middle phalanx—which normally prevents volar migration of the lateral bands—begins to attenuate under the unremitting tension of the intrinsic musculature. Simultaneously, the transverse retinacular ligaments contract, actively pulling the lateral bands volar to the axis of rotation of the PIP joint. Once this critical biomechanical threshold is crossed, the deformity accelerates rapidly.
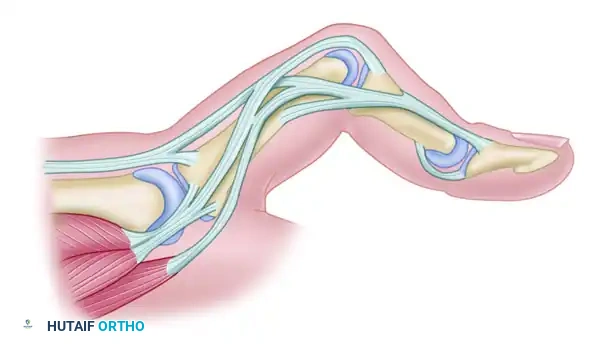
Figure 66-72A: Typical chronic Boutonnière deformity with fixed flexion of the PIP joint and hyperextension of the DIP joint. The lateral bands have subluxated volarward.
Clinically, the classic presentation of a mature Boutonnière deformity is unmistakable: a fixed flexion contracture of the PIP joint combined with a rigid hyperextension of the distal interphalangeal (DIP) joint. However, the orthopedic surgeon must be acutely aware that relying on this classic presentation for diagnosis will result in missed acute injuries. The true Boutonnière deformity is rarely present immediately following an acute central slip rupture. Early diagnosis relies heavily on meticulous clinical examination, specifically the Elson test. In this maneuver, the PIP joint is flexed to 90 degrees over the edge of a table, and the patient is asked to actively extend the PIP joint against resistance. In a normal digit, the DIP joint remains flail because the central slip bears the extensor force. In a central slip rupture, the extensor force is transmitted entirely through the lateral bands, resulting in rigid extension of the DIP joint and an absence of extension force at the PIP joint. Failure to recognize this acute pathology condemns the patient to a chronic, complex reconstruction.
Detailed Surgical Anatomy and Biomechanics
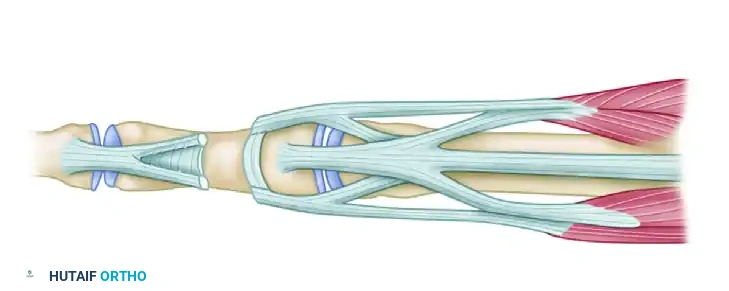
A profound mastery of the extensor mechanism's microanatomy is the absolute prerequisite for any surgeon attempting reconstruction of a Boutonnière deformity. The extrinsic extensor system, originating from the extensor digitorum communis (EDC), bifurcates over the proximal phalanx. The central, most robust portion of this tendon continues distally to insert onto the dorsal base of the middle phalanx, forming the central slip. This structure is the primary active extensor of the PIP joint. The lateral slips of the EDC diverge and are joined by the tendinous contributions of the intrinsic muscles (the lumbricals and interossei) to form the conjoined lateral bands. These lateral bands travel along the dorsolateral aspect of the PIP joint and ultimately converge over the middle phalanx to form the terminal tendon, which inserts onto the dorsal base of the distal phalanx to extend the DIP joint.
The spatial orientation of these tendinous structures is strictly maintained by a complex array of retinacular ligaments. The triangular ligament, a thin but biomechanically critical fascial sheet located over the dorsal middle phalanx, spans the interval between the two lateral bands. Its primary function is to tether the lateral bands dorsally, preventing them from subluxating volarward during PIP joint flexion. Antagonistic to the triangular ligament are the transverse retinacular ligaments, which originate from the volar aspect of the PIP joint capsule and flexor tendon sheath, inserting into the lateral edges of the lateral bands. These ligaments prevent excessive dorsal migration of the lateral bands during active PIP joint extension. The delicate balance between the triangular and transverse retinacular ligaments dictates the precise kinematic tracking of the extensor apparatus.
Biomechanically, the extensor mechanism operates as a highly efficient, load-sharing network. During normal digital extension, the central slip initiates PIP joint extension, while the lateral bands, maintained dorsal to the PIP joint's axis of rotation, assist in PIP extension and simultaneously extend the DIP joint. The oblique retinacular ligament (ORL) of Landsmeer, which originates from the volar proximal phalanx and inserts into the terminal tendon, links the motion of the PIP and DIP joints. As the PIP joint extends, the ORL tightens, passively driving the DIP joint into extension. Conversely, during PIP flexion, the ORL relaxes, allowing the DIP joint to flex smoothly.
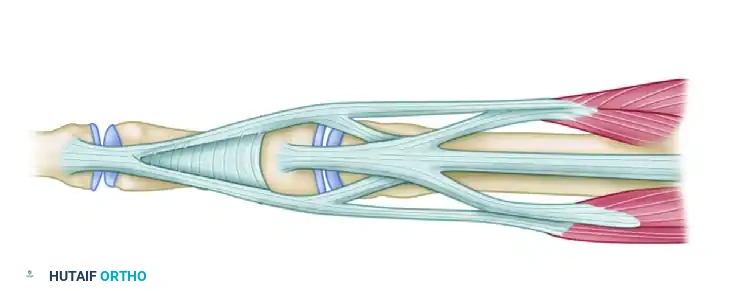
Figure 66-73A: Preoperative biomechanics of the supple buttonhole deformity. The lateral bands are subluxated, causing PIP flexion and DIP hyperextension.
In the pathomechanics of a Boutonnière deformity, the disruption of the central slip initiates a catastrophic failure of this interconnected system. Without the central slip anchoring the extensor mechanism to the middle phalanx, the proximal pull of the EDC is transmitted entirely to the lateral bands. The triangular ligament, unable to withstand this unremitting force, stretches and fails. The lateral bands subsequently subluxate volar to the PIP joint's axis of rotation. At this exact moment, the biomechanical role of the lateral bands reverses: they transition from being secondary extensors of the PIP joint to paradoxical flexors. Concurrently, the uninhibited proximal excursion of the lateral bands concentrates the entire extensor force onto the terminal tendon, driving the DIP joint into rigid hyperextension. The ORL and transverse retinacular ligaments subsequently undergo fibrotic contracture, permanently locking the digit in the classic Boutonnière posture.
Exhaustive Indications and Contraindications
The decision-making algorithm for surgical intervention in central slip dysfunction is highly nuanced, dictated primarily by the chronicity of the lesion, the suppleness of the involved joints, the integrity of the overlying soft tissue envelope, and the patient's functional demands. Acute lacerations or traumatic avulsions of the central slip represent absolute indications for urgent primary surgical repair. In these scenarios, the native anatomy has not yet undergone secondary contracture, and anatomic restoration of the central slip insertion yields highly predictable, excellent functional outcomes. Closed acute ruptures, conversely, are typically managed non-operatively with continuous PIP joint extension splinting for 6 weeks, provided the diagnosis is made within the first few weeks of injury and full passive extension is achievable.
Chronic Boutonnière deformities present a vastly more complex surgical challenge. The primary indication for surgical reconstruction in a chronic setting is a persistent, functionally limiting deformity that has failed an exhaustive course of conservative management and hand therapy. Crucially, the surgeon must differentiate between a "supple" and a "fixed" deformity. A supple deformity—where the PIP joint can be passively extended to neutral and the DIP joint passively flexed—is an indication for soft-tissue rebalancing procedures, such as the Fowler tenotomy or the Littler lateral band relocation. If the deformity is fixed, soft-tissue reconstruction is strictly contraindicated until passive motion is restored.
Contraindications to extensor mechanism reconstruction must be rigorously respected to avoid catastrophic surgical failures. Attempting a complex tendon transfer or relocation in the presence of a rigid volar plate contracture or shortened collateral ligaments will universally fail; the reconstructed central slip will simply stretch out or rupture against the unyielding joint capsule. Severe secondary osteoarthritis of the PIP joint, common in long-standing deformities, is another absolute contraindication to soft-tissue reconstruction, as restoring motion to a destroyed joint will only result in intractable pain. In such cases, salvage procedures (arthrodesis or arthroplasty) are indicated. Furthermore, patients who are non-compliant, cognitively impaired, or unable to participate in the rigorous, months-long postoperative hand therapy protocols are poor candidates for these delicate reconstructive procedures.
| Parameter | Indications for Surgical Intervention | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Acute Injuries | Open lacerations of the central slip; Volar PIP dislocations with avulsion; Displaced avulsion fractures (>2mm). | Active local soft tissue infection; Medically unstable patient. | Crush injuries with severe soft tissue compromise (delay repair). |
| Chronic Supple Deformity | Failure of >6-8 weeks of strict splinting; Functionally limiting PIP lag with preserved passive ROM. | Fixed PIP flexion contracture (must be released first); Destroyed PIP joint articular cartilage. | Severe rheumatoid disease with multiple joint involvement (consider arthroplasty). |
| Chronic Fixed Deformity | Severe contracture failing serial casting (requires joint release + reconstruction/salvage). | Attempting tendon reconstruction WITHOUT prior/concurrent capsular release. | Poor patient compliance; Inability to attend extensive hand therapy. |
| Salvage Scenarios | Painful, arthritic PIP joint; Multiple failed prior soft-tissue reconstructions. | Active infection (for arthroplasty); Lack of functioning flexor tendons. | Heavy manual laborer (relative contraindication for silicone arthroplasty). |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of successful Boutonnière reconstruction. The clinical evaluation must be exhaustive, quantifying the exact degree of active and passive motion at the metacarpophalangeal (MCP), PIP, and DIP joints. The Boyes test is utilized to assess the contracture of the oblique retinacular ligaments; if passive DIP flexion is greater when the PIP joint is flexed compared to when it is extended, ORL contracture is present and must be addressed surgically or therapeutically. High-quality, multi-planar radiographs are mandatory to evaluate the joint space for arthritic changes, assess for volar subluxation of the middle phalanx, and identify any old, ununited avulsion fractures at the dorsal base of the middle phalanx that might complicate anchor placement.
Preoperative rehabilitation is arguably as critical as the surgical intervention itself. For chronic deformities, the surgeon must prescribe a rigorous, therapist-directed program of serial splinting or casting to stretch the contracted volar structures. Dynamic extension splints (e.g., Capener splints) or static progressive serial cylinder casts are utilized over several weeks to restore passive PIP joint extension. Concurrently, the patient performs active and passive DIP joint flexion exercises to stretch the contracted lateral bands and ORL. Surgery should be delayed until maximal passive motion is achieved; operating on a stiff joint guarantees a stiff, non-functional outcome.
Surgical planning involves anticipating the need for various reconstructive techniques based on the intraoperative findings. The surgeon must have a comprehensive armamentarium available, including 0.045-inch and 0.035-inch Kirschner wires for transarticular fixation, micro-suture anchors (1.0mm to 1.5mm) for avulsion repairs, and a variety of non-absorbable and slowly absorbable sutures (e.g., 4-0 braided polyester, 4-0 monofilament nylon). If a tendon graft is anticipated, the patient must be consented for a palmaris longus or plantaris harvest.
Patient positioning and anesthesia are tailored to the complexity of the procedure. While traditional regional blocks (axillary or supraclavicular) combined with a proximal arm tourniquet are standard, there is a growing paradigm shift toward utilizing Wide Awake Local Anesthesia No Tourniquet (WALANT). By utilizing a mixture of lidocaine and epinephrine injected locally, the surgeon achieves excellent hemostasis without a tourniquet, while the patient remains fully awake. This allows the surgeon to ask the patient to actively flex and extend the digit intraoperatively, permitting real-time assessment of the tension and tracking of the reconstructed extensor mechanism. Regardless of the anesthetic choice, the patient is positioned supine with the arm extended on a radiolucent hand table, ensuring unencumbered access for intraoperative fluoroscopy.
Step-by-Step Surgical Approach and Fixation Technique
Acute Primary Repair of the Central Slip
Acute disruptions of the central slip, whether sharp lacerations or traumatic avulsions, necessitate precise anatomic restoration. The surgical approach must be carefully planned to avoid creating a longitudinal scar directly over the extensor mechanism, which can lead to severe tethering and secondary contracture. A lazy-S, bayonet, or gently curved dorsal incision is utilized, elevating full-thickness skin flaps to expose the paratenon. Once the extensor apparatus is visualized, the PIP joint is meticulously cleared of hematoma and debris.
Before any tendon repair is attempted, the PIP joint must be stabilized in a position of absolute, zero-degree extension. This is achieved by driving a 0.045-inch K-wire obliquely across the PIP joint from a distal-dorsal to proximal-volar direction, or via a crossed K-wire technique. This transarticular fixation is paramount; it completely neutralizes all tension on the delicate repair site during the critical early phases of biological healing.
For mid-substance lacerations, the tendon ends are mobilized, ensuring the lateral bands are anatomically reduced dorsal to the axis of rotation. The central slip is repaired using a core suture of 4-0 non-absorbable braided polyester (e.g., Ethibond) or monofilament nylon, utilizing a modified Kessler or Becker technique. This is supplemented with a running epitendinous Silfverskiöld cross-stitch using 5-0 or 6-0 monofilament to optimize the biomechanical strength and smooth the gliding surface. In cases of avulsion injuries where the distal stump is inadequate for suture purchase, a micro-suture anchor (1.0mm - 1.5mm) is deployed into the dorsal base of the middle phalanx. The central slip is then advanced and secured to the anatomic footprint using a horizontal mattress configuration, ensuring intimate tendon-to-bone contact.
Management of the Supple Chronic Deformity: The Fowler/Dolphin Tenotomy
In chronic cases where the PIP joint remains fully supple (passively extendable to zero degrees) but an active extensor lag persists alongside DIP hyperextension, a targeted release of the extensor mechanism may rebalance the digit. The Fowler or Dolphin tenotomy is an elegant, minimally invasive technique designed to alter the kinematic tension across the joints.
Figure 66-73B: Post-tenotomy biomechanics. The lateral bands are released distal to the insertion of the central slips. The resulting proximal migration of the extensor mechanism reduces tension at the DIP joint and increases extensor tension at the PIP joint.
Through a small dorsal incision over the middle phalanx, the extensor mechanism is identified. The lateral bands are sharply transected distal to the triangular ligament but proximal to the terminal tendon insertion. By completely releasing the distal continuity of the extensor apparatus, the entire mechanism is allowed to migrate proximally under the resting tension of the intrinsic and extrinsic muscles. This proximal shift has a dual biomechanical effect: it immediately abolishes the pathological hyperextension force acting on the DIP joint, and it simultaneously increases the resting tension of the extensor hood over the PIP joint, effectively correcting the extensor lag. The DIP joint relies on the retained oblique retinacular ligaments for future extension.
The Littler Technique (Dorsal Shift of Lateral Bands)
When the central slip is irreparably attenuated or absent, and the lateral bands have become fixed in a volar subluxated position, the Littler technique provides a robust, anatomic reconstruction by recruiting the lateral bands to recreate the central extensor force.
Step 1: Incision and Exposure. A generous dorsal curved longitudinal incision is made over the PIP joint, extending from the mid-proximal phalanx to the mid-middle phalanx. Full-thickness flaps are elevated to expose the entire dorsal apparatus.
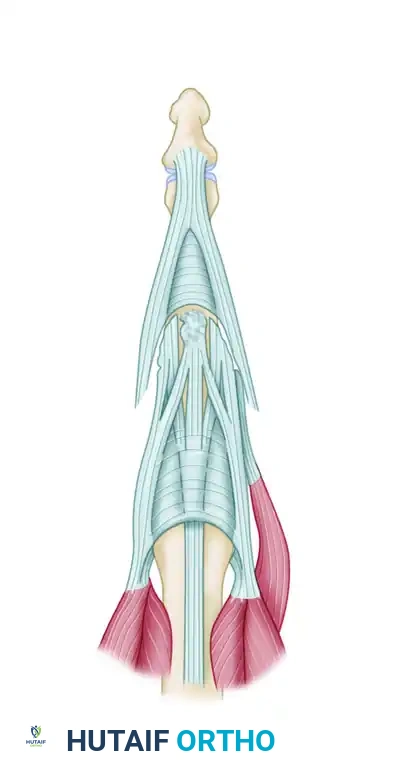
Figure 66-72B: Dorsal curved longitudinal incision.
Step 2: Mobilization of Lateral Bands. The volar-subluxated lateral bands are identified. The contracted transverse retinacular ligaments tethering them volarly are sharply released. The lateral bands are meticulously freed from their distal insertions, taking extreme care to preserve the radialmost fibers of the radial lateral band. This preservation is critical, as it maintains the lumbrical contribution required for active, independent DIP joint extension.

Figure 66-72C: The insertions of the lateral bands are completely freed except for the radialmost fibers of the radial lateral band.
Step 3: Dorsal Relocation. Once fully mobilized, the lateral bands are shifted dorsally and proximally toward the dorsal midline of the PIP joint, effectively bringing them back above the joint's axis of rotation.
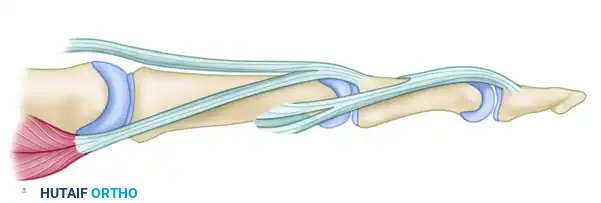
Figure 66-72D: The lateral bands are shifted dorsally and proximally.
Step 4: Suture Reconstruction. The relocated lateral bands are sutured to each other in the midline using interrupted 4-0 non-absorbable sutures. They are then secured to the soft tissues over the proximal third of the middle phalanx and interwoven with any viable remnant of the native central tendon. This creates a thick, robust central extensor batten.
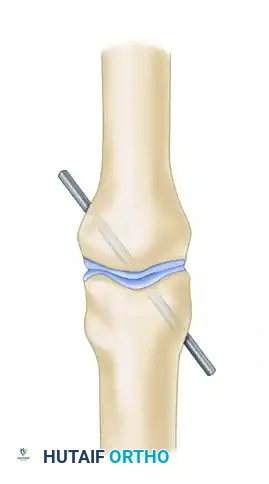
Figure 66-72E: The lateral bands are sutured together and to the central tendon.
Step 5: Transarticular Fixation. The PIP joint is pinned in absolute full extension using a 0.045-inch K-wire. This step is non-negotiable, as the newly reconstructed central slip will fail under the immense tension of early flexion if not rigidly protected.
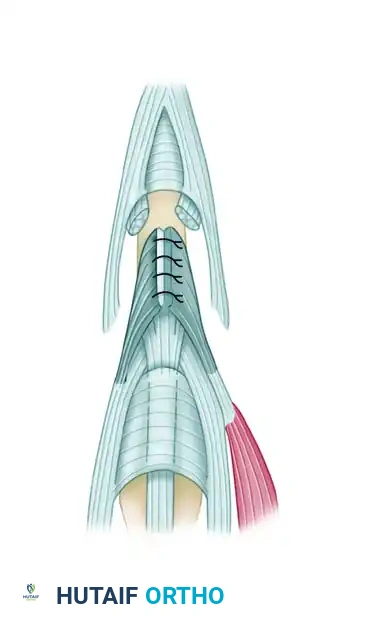
Figure 66-72F: The PIP joint is fixed in full extension by a Kirschner wire.
Step 6: Biomechanical Verification. Following fixation, the biomechanics are assessed. The PIP joint is now extended by the robust, centralized lateral band complex. The DIP joint extension is maintained by the preserved radial lumbrical fibers and the oblique retinacular ligament.

Figure 66-72G: Cross-sectional biomechanics after repair. The lateral bands are restored dorsal to the PIP axis of rotation.
Alternative Reconstructive Techniques
Depending on the specific pattern of tissue loss, the surgeon may need to employ alternative local tissue transfer techniques to span defects in the central slip.
The Snow Technique (Central Slip Flap): In scenarios where the central slip is severed but a thick, robust proximal stump remains over the proximal phalanx, a retrograde flap can be utilized to bridge the gap. A distally based split-thickness flap of the proximal central slip is elevated. After the primary severed ends of the central slip and lateral bands are approximated as closely as possible, this retrograde flap is folded distally over the juncture. It is sutured in place as a reinforcing batten, significantly increasing the mass and strength of the repair site over the critical zone of the PIP joint.
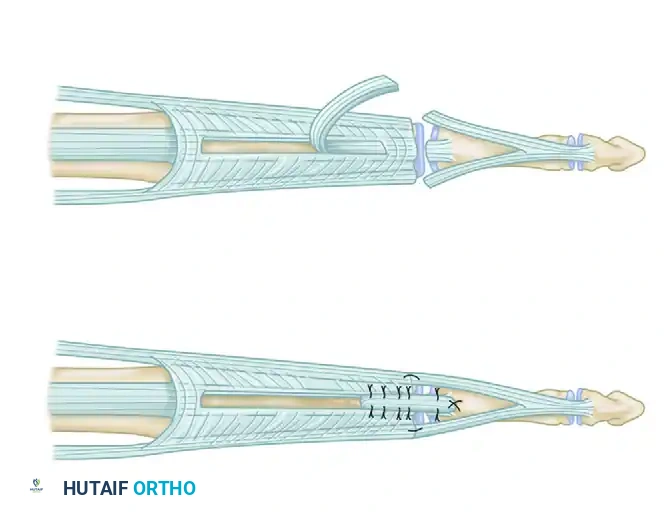
Figure 66-74: Severed extensor mechanism over the PIP joint. A retrograde flap of the central slip has been elevated and brought over the juncture as a batten.
The Aiache Technique (Lateral Band Flaps): This highly intricate technique utilizes split portions of the lateral bands to reconstruct the central slip without completely sacrificing their distal terminal insertions, theoretically preserving better DIP joint kinematics. First, the lateral bands are freed from their volar tethers (transverse retinacular ligaments).
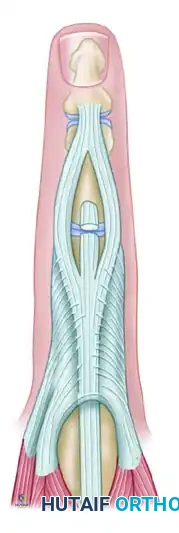
Figure 66-75 (Left): Injury to the middle slip. Lateral bands are freed.
Next, each lateral band is meticulously slit longitudinally into two equal halves, separating the medial and lateral fibers from the proximal phalanx down to the middle phalanx.
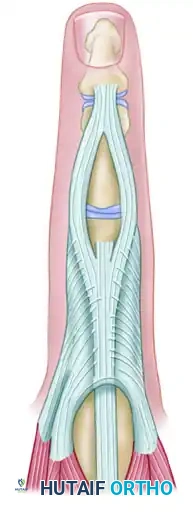
Figure 66-75 (Center): Each lateral band is slit longitudinally.
Finally, the medial halves of these split lateral bands are mobilized dorsally. They are sutured together in the midline directly over the PIP joint and secured to the dorsal capsule and middle phalanx base to recreate the central slip insertion. The lateral halves remain in situ to continue their function as DIP joint extensors.
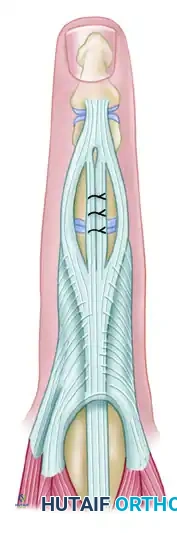
Figure 66-75 (Right): Medial halves of the lateral bands are sutured together and to the capsule in the midline.
Complications, Incidence Rates, and Salvage Management
Surgical reconstruction of the extensor mechanism over the PIP joint is fraught with potential complications. The most ubiquitous complication is a recurrent extensor lag at the PIP joint, with incidence rates reported between 20% and 40% in chronic reconstructions. This typically results from either progressive stretching of the reconstructed tendinous tissue during the early mobilization phase or from inadequate preoperative correction of volar capsular contractures. Conversely, an overly aggressive surgical tightening of the extensor apparatus, or prolonged postoperative immobilization, can result in a severe loss of PIP joint flexion. A stiff, straight finger is functionally far more debilitating than a digit with a mild Boutonnière deformity, as it severely impedes grip strength and the ability to grasp spherical objects.
Hardware-related complications are also prevalent. The transarticular K-wire utilized to protect the repair is a direct conduit for bacterial ingress. Superficial pin tract infections occur in up to 15% of cases and must be managed aggressively with oral antibiotics (e.g., cephalexin or clindamycin) and meticulous local pin care. If the infection tracks deep into the joint space, resulting in septic arthritis, the pin must be removed immediately, the joint surgically irrigated, and the tendon reconstruction potentially sacrificed to eradicate the infection. Micro-suture anchor pullout is a rare but catastrophic complication, usually occurring in osteopenic bone or if aggressive early motion is instituted in a non-compliant patient.
When soft-tissue reconstructions fail, or when the patient presents with a long-standing deformity accompanied by severe secondary osteoarthritis of the PIP joint, salvage procedures are the only viable option. The goal shifts from restoring normal kinematics to providing a painless, stable digit. PIP joint arthrodesis is the gold standard salvage procedure for the index and middle fingers, where stability for pinch grip is paramount. The joint is typically fused in 25 to 30 degrees of flexion for the index finger, increasing progressively to 40 degrees for the small finger to facilitate power grip. For the ring and small fingers in lower-demand patients, PIP joint arthroplasty (utilizing silicone elastomer implants or surface replacements) may be considered to preserve some arc of motion, though patients must be counseled on the high rates of eventual implant subsidence or fracture.
| Complication | Estimated Incidence | Etiology / Risk Factors | Management / Salvage Strategy |
|---|---|---|---|
| Recurrent Extensor Lag | 20% - 40% | Tendon attenuation; Inadequate volar release; Premature K-wire removal. | Dynamic extension splinting; Revision reconstruction (rarely successful); Arthrodesis. |
| Loss of PIP Flexion (Stiffness) | 15% - 30% | Over-tensioning of repair; Prolonged immobilization; Severe scar formation. | Aggressive hand therapy |
