Mastering Tendon Repair: Modified Kessler-Tajima and Pulvertaft Weave Techniques
Key Takeaway
The Modified Kessler-Tajima suture, augmented by the Strickland technique, provides a robust four-strand core repair essential for early active mobilization in flexor tendon injuries. Combined with a running-lock epitendinous stitch, it optimizes biomechanical strength and glide. For tendon transfers involving size mismatches, the Pulvertaft weave remains the gold standard, ensuring superior tensile strength through interlacing tendon integration.
Comprehensive Introduction and Patho-Epidemiology
The primary objective of flexor tendon repair is to achieve a coaptation that is biomechanically robust enough to withstand the physiological forces of early active motion (EAM) while simultaneously maintaining a low-profile, non-bulky configuration that permits unhindered excursion through the complex fibro-osseous digital sheath. The historical evolution of tendon repair has witnessed a dramatic paradigm shift over the past several decades. Early surgical dogma, heavily influenced by Bunnell, dictated prolonged postoperative immobilization due to the inherent weakness of simple two-strand core sutures. However, this approach frequently resulted in devastating peritendinous adhesions, joint contractures, and functional failure, particularly in the notoriously unforgiving Zone II of the hand, famously dubbed "No Man's Land." Modern reconstructive hand surgery has definitively shifted away from simple two-strand techniques, which frequently fail under the physiological loads of active flexion, toward sophisticated multi-strand configurations combined with meticulous epitendinous repairs.
The Modified Kessler-Tajima Suture, particularly when augmented by the Strickland modification (1995), represents a watershed moment in the management of Zone II flexor tendon lacerations. By converting a standard two-strand core into a biomechanically superior four-strand construct and supplementing it with a continuous running-lock epitendinous suture, hand surgeons can reliably achieve a repair strength exceeding 40 to 50 Newtons. This specific tensile strength represents the critical threshold required for safe early active mobilization, allowing the tendon to glide, thereby preventing adhesion formation while simultaneously stimulating intrinsic tenocyte healing and collagen realignment. The epidemiology of these injuries remains significant; flexor tendon lacerations predominantly affect young, working-age males, often resulting from occupational hazards involving sharp implements, glass, or industrial machinery. The economic burden of these injuries, compounded by the rigorous and prolonged rehabilitation required, underscores the necessity for a surgical repair that minimizes the risk of rupture and maximizes functional recovery.
Conversely, when the reconstructive hand surgeon is faced with addressing tendon transfers, intercalary tendon grafting, or complex salvage scenarios involving significant diameter mismatches between donor and recipient tendons, standard end-to-end repairs are biomechanically insufficient and clinically contraindicated. In these specific instances, the Pulvertaft Weave remains the undisputed gold standard of surgical technique. Originally described by Guy Pulvertaft in the mid-20th century, this interlacing technique provides massive surface area integration, translating to unparalleled immediate tensile strength. This robust fixation is paramount in tendon transfers, where the resting tension must be meticulously set to restore the physiological cascade of the hand and re-establish the precise length-tension relationship of the transferred muscle-tendon unit.
The patho-epidemiology of tendon injuries and subsequent repairs is deeply intertwined with the biological phases of tendon healing: the inflammatory phase, the fibroblastic (proliferative) phase, and the remodeling phase. During the inflammatory phase (days 1 to 5), the repair relies entirely on the mechanical strength of the suture construct. As the fibroblastic phase ensues (days 5 to 28), the tendon undergoes a dangerous period of intrinsic softening; the holding power of the tendon ends diminishes, making the repair highly susceptible to gap formation or catastrophic rupture if the initial surgical construct is suboptimal. It is precisely during this vulnerable window that the biomechanical superiority of the four-strand Strickland modification and the geometric interlacing of the Pulvertaft weave prove their clinical indispensability, bridging the critical gap between mechanical suture strength and biological tissue integration.
Detailed Surgical Anatomy and Biomechanics
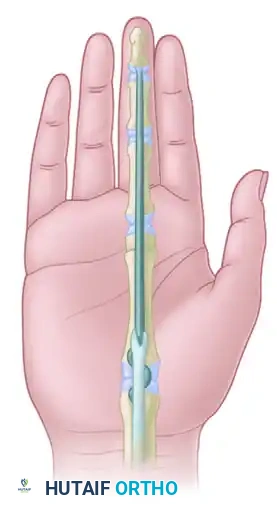
A profound mastery of tendon repair necessitates an exhaustive understanding of the surgical anatomy and the intricate biomechanical forces acting upon the flexor tendon system. The flexor apparatus of the digits is a highly specialized, multi-layered anatomical construct designed to translate linear muscle contraction into precise angular joint rotation. The flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons glide within a tightly constrained synovial environment bounded by the fibro-osseous sheath. This sheath is reinforced by a series of thickened fascial bands known as pulleys—specifically, the five annular (A1-A5) and three cruciate (C1-C3) pulleys. The A2 and A4 pulleys are biomechanically critical; they arise directly from the periosteum of the proximal and middle phalanges, respectively, and serve to prevent tendon bowstringing, thereby maintaining the mechanical advantage and moment arm of the flexor tendons.
Tendon nutrition is a dual-source system that profoundly impacts surgical decision-making. Approximately 30% of the tendon's nutritional requirement is supplied via vascular perfusion through the segmental vincula (vincula brevia and vincula longa), which carry delicate vessels from the digital arteries to the dorsal aspect of the tendons. The remaining 70% of nutrition is derived from synovial diffusion within the digital sheath. This diffusion is actively pumped into the tendon substance by the pressure variations generated during tendon excursion (imbibition). Consequently, surgical techniques must meticulously preserve the vincula and minimize trauma to the dorsal aspect of the tendon. Furthermore, because synovial diffusion requires tendon gliding, early active motion is not merely a rehabilitation strategy to prevent adhesions; it is a fundamental biological requirement for intrinsic tendon healing and tenocyte survival.
The biomechanics of tendon repair center around the concepts of tensile strength, gap resistance, and gliding resistance (the "work of flexion"). The physiological forces experienced by a flexor tendon vary dramatically based on activity. Passive mobilization generates approximately 2 to 4 Newtons (N) of force. Light active unresisted flexion requires roughly 10 to 15 N. A strong grasp or pinch can generate forces exceeding 50 to 70 N. A standard two-strand modified Kessler repair yields an ultimate tensile strength of approximately 20 to 30 N, which is dangerously close to the forces generated during simple active motion, particularly when post-traumatic edema increases the gliding resistance within the sheath. By upgrading to a four-strand core configuration (such as the Strickland modification), the ultimate tensile strength is effectively doubled to 40-50 N, providing a safe margin for early active motion protocols.
The epitendinous suture is not a mere cosmetic adjunct; it is a critical biomechanical component of the repair construct. A meticulously executed running-lock (Silfverskiöld) epitendinous suture increases the ultimate tensile strength of the repair by up to 50%. More importantly, it provides superior resistance to gap formation. A gap greater than 3 mm is considered a clinical failure; it disrupts the smooth gliding surface, significantly increases the work of flexion, invites the ingrowth of dense vascularized adhesions from the surrounding sheath, and dramatically increases the risk of secondary rupture by exposing the core sutures to sheer stress. In the context of the Pulvertaft weave, the biomechanics rely on maximizing the surface area of contact between the donor and recipient tendons. The alternating 90-degree perpendicular passes convert longitudinal tensile forces into sheer forces distributed across a massive biological interface, resulting in an immediate mechanical strength that frequently exceeds the ultimate tensile strength of the native tendon substance itself.
Exhaustive Indications and Contraindications
The selection of the appropriate tendon repair technique is dictated by a multitude of factors, including the chronicity of the injury, the anatomical zone, the degree of tissue loss, the caliber of the tendons involved, and the patient's physiological and psychological capacity to adhere to rigorous postoperative rehabilitation. The Modified Kessler-Tajima (Strickland modification) and the Pulvertaft weave serve distinct, albeit occasionally overlapping, roles in the reconstructive surgeon's armamentarium.
The Modified Kessler-Tajima technique is the procedure of choice for acute primary repairs of the flexor tendons, particularly within Zones I and II. It is specifically indicated for sharp, clean lacerations where the tendon ends can be approximated without excessive tension. The four-strand core combined with an epitendinous stitch provides the optimal balance of strength and volume, allowing the repaired tendon to pass smoothly beneath the critical A2 and A4 pulleys. This technique is also indicated in delayed primary repairs (within 10 to 14 days post-injury), provided that the retracted proximal stump can be mobilized without causing ischemic damage to the muscle belly or requiring excessive force that would compromise the repair site.
The Pulvertaft weave is indicated when end-to-end coaptation is either anatomically impossible or biomechanically unsound. Its primary indication is in tendon transfers, such as the extensor indicis proprius (EIP) to extensor pollicis longus (EPL) transfer for chronic EPL ruptures, or superficialis-to-profundus transfers. It is also the technique of choice for intercalary tendon grafting, typically utilized in two-stage flexor tendon reconstructions where a silicone Hunter rod has previously formed a pseudosheath, and a free graft (e.g., palmaris longus or plantaris) is being introduced. Furthermore, the Pulvertaft weave is essential when there is a significant discrepancy in the cross-sectional diameter of the tendons being joined, as a standard core suture would pull through the smaller tendon under physiological load.
Contraindications to primary multi-strand flexor tendon repair include massive crush injuries with severe contamination, where the risk of deep space infection precludes the placement of permanent braided suture material. In such cases, delayed primary repair or staged reconstruction is mandated. Segmental tendon loss exceeding 1.5 cm typically precludes primary repair due to excessive tension, necessitating grafting. Relative contraindications include patients with severe cognitive impairment, psychiatric conditions, or documented non-compliance, as the success of these repairs is entirely dependent on strict adherence to complex early active motion protocols.
| Clinical Scenario | Preferred Surgical Technique | Primary Rationale / Biomechanical Advantage | Absolute Contraindications |
|---|---|---|---|
| Acute Zone II Laceration (Clean, <10 days) | Modified Kessler-Tajima (Strickland 4-Strand) | Low profile, prevents pulley impingement, sufficient strength for EAM (40-50N). | Severe crush injury, active gross infection, segmental loss >1.5 cm. |
| Tendon Transfer (e.g., EIP to EPL) | Pulvertaft Weave | Massive surface area integration, immediate high tensile strength, accommodates size mismatch. | Inadequate excursion of donor, stiff recipient joint, denervated donor muscle. |
| Two-Stage Tendon Grafting (Stage II) | Pulvertaft Weave (Proximal coaptation) | Secures small-diameter graft (palmaris longus) to large-diameter motor tendon (FDP). | Collapsed pseudosheath, active infection, severe joint contracture. |
| Chronic Flexor Rupture (>4 weeks) | Tendon Grafting with Pulvertaft Weave | Primary repair impossible due to myostatic contracture and tendon end degeneration. | Poor passive range of motion, inadequate soft tissue coverage. |
| Frayed/Degenerative Tendon Ends | Double Right-Angle or Krackow Core | Grasping configuration prevents suture pull-out in structurally compromised tissue. | Complete loss of tendon substance requiring graft. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful tendon surgery. The clinical examination must systematically isolate and test the FDS and FDP tendons of each digit. The FDP is tested by blocking the middle phalanx and asking the patient to flex the distal interphalangeal (DIP) joint. The FDS is tested by holding all non-injured fingers in full extension (neutralizing the shared muscle belly of the FDP) and asking the patient to flex the proximal interphalangeal (PIP) joint of the injured digit. The resting cascade of the hand must be carefully observed; a loss of the normal progressive flexion from the index to the small finger is a pathognomonic sign of a flexor tendon disruption. The tenodesis effect—passive extension of the wrist causing spontaneous flexion of the digits—should also be evaluated to confirm complete structural discontinuity.
Advanced imaging is rarely required for acute, open lacerations, as the diagnosis is clinical and surgical exploration is mandated. However, in cases of closed avulsions (e.g., Jersey finger) or delayed presentations, ultrasound or magnetic resonance imaging (MRI) can be invaluable for localizing the retracted proximal stump. Identifying the level of retraction (e.g., into the palm versus into the carpal tunnel) allows the surgeon to plan the surgical incisions accurately, minimizing unnecessary dissection and trauma to the palmar fascia and neurovascular bundles.
The choice of anesthesia has undergone a revolutionary transformation in recent years. While regional blocks (axillary or supraclavicular) or general anesthesia remain viable options, Wide-Awake Local Anesthesia No Tourniquet (WALANT) is increasingly recognized as the gold standard for tendon repair and reconstruction. The WALANT technique utilizes a tumescent mixture of lidocaine (for local anesthesia) and epinephrine (for profound hemostasis), buffered with sodium bicarbonate to eliminate the pain of injection. By eliminating the pneumatic tourniquet and maintaining patient consciousness, the surgeon can perform intraoperative active movement testing. The patient is instructed to actively flex and extend the digit once the repair is completed. This allows the surgeon to visually confirm the integrity of the repair under true physiological load, identify and immediately correct any gap formation, and assess for impingement of the repair site against the A2 or A4 pulleys. If impingement occurs, the surgeon can precisely vent the pulley just enough to allow clearance without causing bowstringing.
Patient positioning requires the patient to be supine with the operative arm extended on a stable, radiolucent hand table. If WALANT is not utilized, a pneumatic tourniquet is applied to the proximal arm over generous padding and inflated to 250 mm Hg (or 100 mm Hg above systolic pressure) after thorough exsanguination with an Esmarch bandage. The surgical field must be illuminated with high-quality overhead lighting, and the surgeon must utilize loupe magnification (typically 2.5x to 3.5x) to ensure precise suture placement and minimal trauma to the delicate epitenon. Instrumentation should include fine plastic surgery instruments, sharp tenotomy scissors, non-toothed micro-forceps to prevent crushing the tendon substance, and appropriate suture materials. Core sutures typically utilize 3-0 or 4-0 braided polyester (e.g., Ticron, Ethibond) or looped Supramid, while the epitendinous repair requires a fine 5-0 or 6-0 monofilament nylon or polypropylene (Prolene) on a tapered micro-needle.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach to the flexor tendon system must provide wide, extensile exposure while preventing flexion contractures of the overlying skin. Bruner zig-zag incisions or mid-lateral incisions are standard. The apex of the Bruner flaps must extend to the mid-axial line, and the angles should be approximately 90 degrees to prevent tip necrosis. Once the skin flaps are elevated, the neurovascular bundles are identified and protected. The fibro-osseous sheath is exposed, and the site of laceration is identified. The retracted proximal tendon must be retrieved with extreme care. Blind grasping with forceps severely damages the epitenon and induces dense adhesions. Instead, the tendon should be "milked" distally from the palm. If this fails, a pediatric feeding catheter can be passed proximally through the sheath, sutured to the tendon stump, and used to gently pull the tendon distally.
The Modified Kessler-Tajima Suture (Strickland Modification)
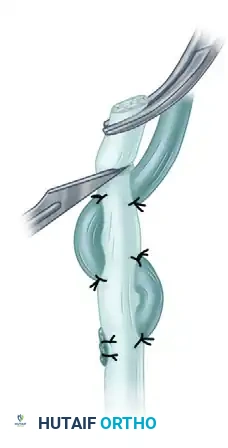
The Strickland modification of the Kessler-Tajima technique is a highly reliable four-strand repair that balances exceptional tensile strength with a low-profile volume. The procedure begins with the placement of the Tajima core sutures in both the proximal and distal stumps. The Tajima modification of the classic Kessler stitch involves passing the suture from the cut surface of the tendon, exiting laterally, traversing the epitenon longitudinally, and re-entering to exit through the cut surface. This specific routing ensures that when the knots are tied, they are buried deeply within the repair site, preventing them from protruding and catching on the intricate pulley system.
FIGURE 66-21 A: Tajima core sutures in place. The back wall (dorsal) running-lock peripheral epitendinous stitch is in progress.
Before the core sutures are approximated and tied, it is highly advantageous—and often critical—to repair the dorsal aspect (back wall) of the tendon. Once the core sutures are tied and the thick tendon ends are brought together, accessing the dorsal wall to place a meticulous epitendinous stitch becomes exceedingly difficult and risks iatrogenic damage to the dorsal vincula. Utilizing a 5-0 or 6-0 monofilament nylon, a running-lock (Silfverskiöld) peripheral epitendinous suture is performed along the dorsal margin. This back wall stitch provides a smooth gliding surface against the dorsal aspect of the flexor sheath and perfectly aligns the tendon ends.

FIGURE 66-21 B: Back wall suturing completed. The dorsal running-lock stitch provides a smooth gliding surface against the dorsal aspect of the flexor sheath.
To upgrade the repair from a standard two-strand construct to the robust four-strand Strickland modification, a horizontal mattress suture is introduced into the core configuration. Using a 4-0 braided polyester suture, the mattress stitch is placed in the palmar (volar) tendon gap. It is imperative that this mattress suture grasps an adequate volume of tendon tissue—typically entering and exiting at least 7 to 10 mm from the cut edge. If placed too close to the laceration site, the suture will simply pull out through the longitudinal collagen bundles under tension, rendering the four-strand upgrade useless.
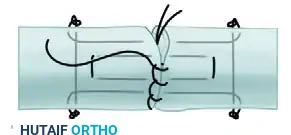
FIGURE 66-21 C: Mattress core suture added in the palmar tendon gap, effectively doubling the core strands crossing the repair site.
With all four core strands precisely placed, the tendon ends are carefully approximated. The tension on the knots must be meticulously balanced. Over-tensioning the core sutures will cause the tendon ends to bunch and buckle, significantly increasing the cross-sectional area of the repair, leading to severe impingement within the sheath and increasing the work of flexion. Conversely, under-tensioning will lead to immediate gap formation. The knots are tied securely, ensuring they are buried deeply within the tendon substance.
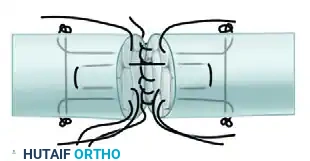
FIGURE 66-21 D: All core sutures tied. The tendon ends are now flush, with no visible gapping.
The final step of the repair involves completing the peripheral epitendinous envelope. The 5-0 or 6-0 nylon running-lock stitch is continued from the dorsal wall around the palmar (volar) aspect of the tendon. The needle should take shallow but secure bites, purchasing approximately 1 to 2 mm of the epitenon and the superficial endotenon. The running-lock configuration is biomechanically superior to a simple running stitch because it actively tightens upon itself under longitudinal load, acting as a Chinese finger trap to resist gap formation and neaten the frayed edges of the repair site.
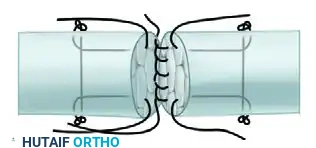
FIGURE 66-21 E: Completion of the running-lock peripheral epitendinous suture on the palmar aspect.
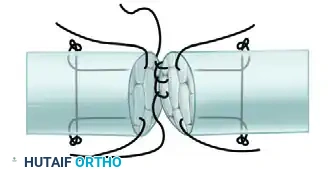
FIGURE 66-21 F: Repair completed. The final construct is a simplified four-strand repair in which the basic two-strand core suture is supplemented by a horizontal mattress suture and a running-lock stitch.
Alternative Core Configurations
While the Modified Kessler-Tajima core is highly effective for clean, sharp lacerations, surgeons must be well-versed in alternative core grasping techniques. In scenarios involving avulsions, crush injuries, or delayed presentations, the tendon ends may be frayed, softened, or degenerative. A standard Kessler stitch relies on the longitudinal integrity of the collagen fibers; in degenerative tissue, it will easily pull out. In these instances, a grasping configuration, such as a double right-angle suture or a Krackow stitch, is required. These configurations cross the longitudinal fibers transversely, providing excellent grip and preventing pull-out in structurally compromised tissue.
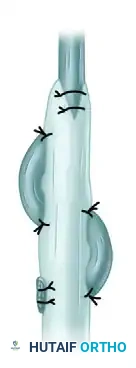
FIGURE 66-22: Double right-angle suture with a single monofilament or multifilament wire suture threaded on a curved needle. This configuration provides excellent grip in softer tendon tissue.
The Pulvertaft Weave Technique
When performing tendon transfers or utilizing tendon grafts, the surgeon frequently encounters tendons of disparate diameters. An end-to-end repair in these scenarios is biologically prone to non-union and biomechanically prone to catastrophic rupture. The Pulvertaft weave technique solves this dilemma by interlacing the smaller donor tendon directly through the substance of the larger recipient tendon, creating a massive surface area for biological healing and immediate mechanical strength.
The preparation of the tendons requires meticulous tissue handling. Both the donor and recipient tendons must be mobilized adequately to allow for sufficient excursion. Crucially, the larger recipient tendon should be cleared of its paratenon only at the exact site of the weave. Stripping the paratenon over a larger area will devascularize the tendon and lead to dense, restrictive adhesions.
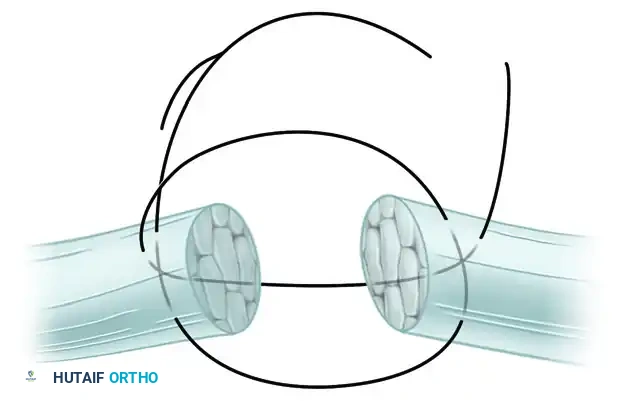
FIGURE 66-23: Pulvertaft technique of suturing a tendon of small diameter to one of larger diameter. This composite illustrates the sequential weaving and anchoring process.
The first pass of the weave establishes the foundation of the repair. The recipient (larger) tendon is pierced through its central axis using a No. 11 Bard-Parker knife blade. A straight hemostat is used to grasp the blade on the opposite side; as the blade is withdrawn, the hemostat is advanced through the slit, dilating the tract. The tip of the smaller tendon is then grasped with the hemostat and pulled completely through the larger tendon.

FIGURE 66-23 A: The smaller tendon is brought through the larger tendon. Tension is meticulously adjusted before anchoring with one or two sutures.
Adjusting the resting tension of the transfer is arguably the most critical and challenging step of the entire procedure. The cascade of the hand must be evaluated, and the tension must be set to slightly over-correct the deformity, accounting for the inevitable viscoelastic creep and stretching of the muscle-tendon unit postoperatively. Once the precise tension is established, the smaller tendon is anchored to the larger tendon at the site of the first pass using 3-0 or 4-0 non-absorbable braided sutures (e.g., Ticron or Ethibond) placed in a mattress fashion.
Subsequent passes are then performed to maximize the biomechanical strength of the weave. A second slit is created in the larger tendon, approximately 5 to 10 mm proximal to the first slit. It is a crucial biomechanical requirement that this second slit be oriented at a 90-degree angle (perpendicular) to the first slit. If the slits are made in the same plane, the longitudinal collagen bundles of the larger tendon will split, completely destroying its structural integrity. The smaller tendon is pulled through this perpendicular hole and anchored again.
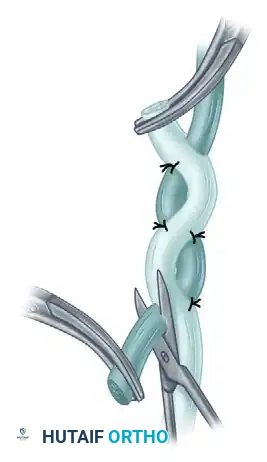
FIGURE 66-23 B: The tendon is brought through a more proximal hole and is anchored again with one or two sutures after tension is verified.
Alternative view demonstrating the perpendicular passes of the smaller tendon through the larger recipient tendon, maximizing contact area.
After 3 to 4 perpendicular passes (depending on the available length of the donor tendon), the excess of the smaller tendon is cut flush with the surface of the larger tendon. The exit hole is meticulously closed over the cut stump with one or two fine sutures to prevent it from catching on surrounding fascial planes. To ensure a smooth glide and prevent a bulky, restrictive stump at the proximal end of the weave, the excess of the larger tendon is trimmed into a "V" shape. This creates a "fish mouth" that is wrapped circumferentially around the central location of the smaller tendon and sutured closed, beautifully streamlining and tapering the repair site.

FIGURE 66-23 C & D: After the excess is cut flush, the exit hole is closed. The excess of the larger tendon is trimmed to permit central location of the smaller tendon. This so-called fish mouth is closed with sutures to streamline the repair.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and rigorous adherence to postoperative protocols, tendon repairs remain fraught with potential complications. The delicate balance between achieving sufficient mechanical strength and preventing restrictive scar tissue formation makes complications relatively common, requiring the surgeon to be well-versed in salvage management and secondary reconstructive procedures.
The most frequent complication following flexor tendon repair is the formation of restrictive peritendinous adhesions, occurring in approximately 15% to 20% of cases, particularly in Zone II. Adhesions tether the tendon to the surrounding fibro-osseous sheath or adjacent skeletal structures, severely limiting active excursion and resulting in a discrepancy between passive and active range of motion. If aggressive hand therapy and dynamic splinting fail to resolve the stiffness by 4 to 6 months postoperatively, and the soft tissue envelope is supple, a surgical tenolysis is indicated. Tenolysis is a technically demanding salvage procedure requiring extensive release of scar tissue while preserving the critical A2 and A4 pulleys. It is strictly contraindicated if the patient lacks full passive range of motion, as the limitation is likely capsular rather than tendinous.
Tendon rupture is a catastrophic complication, occurring in 3% to 5% of modern multi-strand repairs. Ruptures typically occur between days 7 and 21 postoperatively, coinciding with the fibroblastic phase of healing when the tendon ends are biologically softest and the mechanical strength of the suture construct begins to degrade before intrinsic collagen cross-linking has matured. Ruptures are clinically identified by a sudden loss of active flexion, often accompanied by a palpable pop or a sudden change in the resting cascade of the digit. Immediate surgical re-exploration is mandated. If recognized acutely (within 7-
