Comprehensive Postoperative Management and Rehabilitation in Hand Surgery
Key Takeaway
Optimal postoperative care in hand surgery requires a delicate balance between tissue protection and early functional rehabilitation. This comprehensive guide details evidence-based protocols for dressing application, edema control, and splinting. It emphasizes the critical role of multidisciplinary hand therapy, strict elevation, and strategic wound surveillance to prevent complications, minimize scar contracture, and maximize functional outcomes in the upper extremity.
Comprehensive Introduction and Patho-Epidemiology
The success of any surgical intervention in the upper extremity is inextricably linked to the quality of the postoperative management. Care after surgery must be orchestrated intelligently and meticulously so that traumatized tissues are allowed to heal without disruption, while the biomechanical functions of the affected part are restored as rapidly and safely as possible. The hand is an unforgiving anatomical structure; it represents a highly concentrated, mechanically complex arrangement of gliding tissues, articular surfaces, and delicate neurovascular bundles confined within tight fascial compartments. Even minor deviations in postoperative protocols can result in catastrophic stiffness, debilitating edema, or irreversible joint contractures. The concept of the "one wound" phenomenon, classically described by Peacock, dictates that all injured tissues in the hand heal through a single, unified scar bed. The overarching goal of postoperative care is to modulate this scar formation, ensuring that differential gliding between tendons, nerves, and bone is preserved.
Postoperative care does not begin in the recovery room; it begins in the operating theater with the application of the surgical dressing and the controlled deflation of the pneumatic tourniquet. The pathophysiology of postoperative hand complications is driven primarily by the inflammatory cascade initiated by surgical trauma. The accumulation of protein-rich interstitial fluid rapidly organizes into a fibrinous glue. If this exudate is not aggressively managed through elevation, compression, and controlled motion, fibroblasts will infiltrate the matrix, depositing disorganized Type III collagen. Over the subsequent weeks, this collagen cross-links and matures into dense, unyielding Type I collagen scar tissue, permanently tethering the gliding planes of tendons and obliterating the redundant folds of joint capsules.
Epidemiologically, postoperative stiffness remains the most frequent complication following hand surgery, significantly outpacing infection, hardware failure, or tendon rupture. Studies indicate that up to 30% of patients undergoing complex intra-articular fracture fixation or multi-zone tendon repairs will experience clinically significant stiffness requiring prolonged therapeutic intervention or secondary surgical release (tenolysis or capsulotomy). Furthermore, the incidence of Complex Regional Pain Syndrome (CRPS) can approach 5% to 10% in susceptible populations, particularly following distal radius fractures or crush injuries. The prevention of these pathological states requires a profound understanding of tissue biomechanics, rigorous adherence to edema control protocols, and the seamless integration of a multidisciplinary hand therapy team.
This comprehensive guide delineates the textbook-level, evidence-based protocols for postoperative management. It encompasses the intricate biomechanics of immobilization, the physiological principles of the surgical dressing, meticulous wound surveillance, and the phased integration of rehabilitation protocols. By mastering these postoperative principles, the orthopedic surgeon ensures that the technical perfection achieved in the operating room translates into optimal functional outcomes for the patient.
Detailed Surgical Anatomy and Biomechanics
The biomechanical foundation of postoperative hand management relies heavily on an intimate understanding of articular geometry and ligamentous kinematics. The metacarpophalangeal (MCP) joints and the interphalangeal (IP) joints possess fundamentally different architectural characteristics, which dictate the mandatory "position of safe immobilization" (the intrinsic-plus or James position). The metacarpal head is asymmetric; it is wider on its volar aspect than on its dorsal aspect. Furthermore, the origin of the MCP collateral ligaments is eccentric, situated dorsal to the axis of rotation. This anatomical arrangement creates a "cam effect." When the MCP joint is extended, the collateral ligaments are lax, allowing for lateral mobility (abduction/adduction). When the MCP joint is flexed to 70-90 degrees, the collateral ligaments are stretched to their maximal length over the broad volar condyles, becoming taut. Immobilizing the MCP joints in extension allows these ligaments to shorten and fibrose, resulting in an intractable extension contracture.
Conversely, the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are bicondylar hinge joints with collateral ligaments that remain relatively isometric throughout the arc of motion. However, the volar plates of the IP joints are highly susceptible to contracture. The volar plate is a thick, fibrocartilaginous structure that prevents hyperextension. If the IP joints are immobilized in flexion, the check-rein ligaments and the proximal membranous portion of the volar plate will rapidly shorten and adhere to the underlying periosteum of the proximal phalanx. This results in a devastating flexion contracture. Therefore, the biomechanical imperative for IP joint immobilization is full, unremitting extension, maintaining the volar structures at their maximum physiological length.
The gliding planes of the flexor and extensor mechanisms represent another critical anatomical consideration in postoperative management. In the flexor system, particularly within the unforgiving Zone II (Bunnell’s "no man's land"), the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons must glide smoothly within a tightly constrained fibro-osseous sheath. The sheath is reinforced by a complex system of annular (A1-A5) and cruciform (C1-C3) pulleys. Postoperative edema and hematoma formation within this sheath disrupt the delicate vincula (blood supply) and promote the formation of restrictive adhesions. Rehabilitation protocols must balance the protection of the healing tendon repair with the necessity of early controlled motion to stimulate intrinsic tendon healing and prevent adherence to the sheath.
On the dorsal aspect, the extensor mechanism is an intricate web of central slips, lateral bands, and retinacular ligaments, covered by exceptionally thin dorsal skin with minimal subcutaneous fat. The extensor tendons lack a defined synovial sheath over the phalanges, relying instead on a paratenon for gliding. This makes them highly vulnerable to adherence to the overlying skin or underlying bone following trauma or surgery. Immobilization protocols for extensor injuries must carefully manage the delicate balance between the intrinsic musculature (lumbricals and interossei) and the extrinsic extensors, often requiring highly specific dynamic or static-progressive splinting to prevent extensor lag or secondary deformities such as boutonnière or swan-neck configurations.
Exhaustive Indications and Contraindications
The selection of a postoperative management strategy—ranging from rigid static immobilization to immediate early active motion (EAM)—must be tailored to the specific surgical intervention, the biological quality of the tissues, and the patient's capacity for compliance. The indications for specific protocols are derived from the biomechanical demands of the repaired structures and the timeline of cellular healing. Conversely, certain therapeutic modalities and patient behaviors represent absolute contraindications, threatening the integrity of the repair and precipitating severe complications.
Rigid static immobilization in the intrinsic-plus position is strictly indicated for non-displaced or rigidly fixed metacarpal and phalangeal fractures, severe soft tissue crush injuries requiring massive edema control, and the immediate postoperative phase following complex skin grafting or flap coverage. In these scenarios, the primary objective is the prevention of mechanical shear at the wound interface and the mitigation of the inflammatory response. Conversely, early active motion (EAM) protocols are strongly indicated following primary flexor and extensor tendon repairs (provided a robust core suture technique, such as a 4-strand or 6-strand repair, has been utilized), tenolysis procedures, and uncomplicated joint arthroplasties. EAM prevents adhesion formation, promotes intrinsic cellular healing through mechanotransduction, and significantly improves ultimate excursion.
Contraindications in postoperative hand therapy are critical parameters that must be explicitly communicated to both the patient and the hand therapist. The application of dependent heat (e.g., hot packs or paraffin baths applied while the arm is hanging down) is absolutely contraindicated. Heat induces profound vasodilation, which, when combined with gravity, results in massive, rapid edema formation, overwhelming the lymphatic drainage capacity of the extremity. Furthermore, forced passive manipulation of stiff joints by the patient, therapist, or surgeon is strictly prohibited. Aggressive passive stretching tears delicate, healing collagen fibers, inducing micro-hemorrhage and a renewed inflammatory cascade, ultimately resulting in a thicker, more restrictive scar.
| Modality / Protocol | Primary Indications | Absolute Contraindications | Clinical Rationale / Biomechanical Impact |
|---|---|---|---|
| Static Intrinsic-Plus Immobilization | Metacarpal/phalangeal fractures, crush injuries, skin grafts, severe infections. | Flexor tendon repairs requiring excursion, tenolysis, capsulotomies. | Maintains collateral ligaments and volar plates at maximal length; prevents shear forces on delicate skin grafts; controls massive edema. |
| Early Active Motion (EAM) | Multi-strand flexor tendon repairs, robust extensor repairs, tenolysis. | Tenuous 2-strand tendon repairs, non-compliant patients, active joint infections. | Mechanotransduction stimulates intrinsic tendon healing; prevents restrictive adhesions in Zone II; requires strong surgical construct to prevent gap formation. |
| Dynamic Splinting (e.g., Kleinert) | Traditional flexor tendon protocols, specific extensor tendon zones, nerve palsies. | Rigid joint contractures, severe fluctuating edema, uncooperative pediatric patients. | Provides controlled stress to healing tissues; utilizes reciprocal inhibition; protects repair while allowing passive glide. |
| Dependent Heat Therapy | Rarely indicated in acute phases. May be used late for chronic stiffness only with elevation. | Acute postoperative phase (0-3 weeks), active inflammation, CRPS exacerbations. | Profound vasodilation combined with gravity causes catastrophic interstitial fluid accumulation and fibrinous exudate. |
| Forced Passive Manipulation | None. Passive motion should always be gentle and within pain limits. | Stiff joints, acute fractures, recent tendon repairs, CRPS. | Tearing of collagen fibers induces micro-hemorrhage, restarts the inflammatory cascade, and results in thicker, unyielding scar tissue. |
Pre-Operative Planning, Templating, and Patient Positioning
The orchestration of postoperative care is deeply rooted in meticulous preoperative planning and intraoperative execution. The surgeon must conceptualize the final postoperative dressing and immobilization construct long before the first incision is made. This requires an assessment of the planned surgical exposure, the anticipated degree of tissue trauma, and the specific structures that will require protection versus early mobilization. Preoperative planning also involves templating the splinting material, ensuring adequate inventory of specialized dressings (e.g., non-adherent layers, synthetic sponges), and coordinating with the anesthesia team regarding the timing of tourniquet deflation and postoperative pain management strategies.
Tourniquet management represents a critical juncture in the transition from the intraoperative to the postoperative phase. The deflation of the pneumatic tourniquet dictates the immediate hemodynamic response of the extremity. A surgical warning of the highest order must be heeded: immediately before the tourniquet is removed, the hand must be elevated and kept constantly elevated above the level of the heart. Releasing the tourniquet while the hand is in a dependent position invites a massive, rapid influx of arterial blood against a closed, sluggish venous system. This leads to catastrophic venous engorgement, reactive hyperemia, and immediate hematoma formation within the surgical dead spaces. A hematoma is devastating; it acts as a highly inflammatory space-occupying lesion, increasing compartmental pressures, causing severe pain, and eventually organizing into dense, restrictive scar tissue.
Patient positioning in the immediate postoperative period is the cornerstone of edema control. Bed rest for 3 days or longer is strongly recommended after major reconstructive surgery on the hand. General body activity increases cardiac output and peripheral blood flow, which paradoxically increases edema in the dependent hand. Effective elevation requires the hand to be positioned above the level of the heart, utilizing modalities such as overhead suspension, firm pillows, or commercially available preformed rubber sponge blocks. Merely supporting the hand in a standard ambulatory arm sling is highly ineffective; in a standard sling, the hand often rests at or below the level of the right atrium, allowing gravity to promote venous pooling and interstitial fluid accumulation.
Pediatric patients present unique challenges in postoperative planning and positioning. The conical shape of the child's forearm inherently predisposes short arm splints and bandages to slip distally, compromising immobilization and exposing surgical wounds. Furthermore, a child's inherent non-compliance and high activity level necessitate highly robust constructs. To control this effectively, the surgeon should routinely apply a long arm splint or a long arm cast, locking the elbow at 90 degrees to prevent distal migration. Enclosing the entire extremity in a tube of stockinette that is secured proximally around the torso or shoulder prevents the child from pulling the dressing off, scratching the wound, or introducing foreign bodies into the cast, thereby mitigating the risk of postoperative infection.
Step-by-Step Surgical Approach and Fixation Technique
In the context of postoperative hand management, the "surgical approach" refers to the highly structured, step-by-step application of the surgical dressing and the execution of scar optimization techniques. The surgical dressing in hand surgery is not merely a passive covering; it is an active therapeutic device designed to control edema, absorb exudate, immobilize specific joints, and protect the healing wound from mechanical shear and bacterial contamination. The routine dressing must be applied in a meticulous, multi-layered fashion by the operating surgeon, not delegated to inexperienced personnel.
The application begins with the primary contact layer. A closely woven, non-adherent patch of gauze, such as Xeroform (bismuth tribromophenate) or Adaptic (cellulose acetate impregnated with petrolatum emulsion), is placed directly over the meticulously approximated incision. The primary function of this non-adherent layer is to prevent granulation tissue from growing through the dressing material. If standard dry gauze is utilized, capillary loops will interweave with the fabric within 48 hours. Upon removal, this causes severe pain, disruption of the delicate healing epithelium, and micro-hemorrhage, thereby delaying wound maturation. The petrolatum-based layer allows serous exudate to pass through to the secondary layer while maintaining a physiologically moist wound environment, which is critical for optimal keratinocyte migration.
Following the primary layer, the hand is positioned precisely in the intrinsic-plus position, and the intermediate conforming layer is applied. This layer consists of cotton sponges or synthetic Acrilan sponges that have been thoroughly moistened in sterile saline or a glycerin solution. The use of moistened sponges is a critical biomechanical technique. Moist sponges conform to the complex, three-dimensional contours of the hand—specifically the web spaces and the palmar arches—much more accurately than dry sponges. By conforming perfectly, they distribute compressive pressure evenly across the integument, adhering to Pascal’s principle of fluid pressure. This uniform distribution prevents focal areas of ischemia that can lead to pressure necrosis over bony prominences. Additionally, the capillary action of the moistened sponges promotes the rapid absorption of blood and serous exudate, drawing it away from the incision site and into the bulk of the dressing.
Once the conforming layer is meticulously packed, the outer compressive and splinting layer is applied. A roll of cotton or synthetic sheet wadding (cast padding) is wrapped circumferentially around the hand and forearm to provide a uniform layer of soft tissue protection. An appropriate splint, constructed of either 10-15 layers of plaster of Paris or modern fiberglass, is then applied to the volar or dorsal aspect depending on the surgical requirement. The splint is secured and held in precise position with a roll of 2-inch or 3-inch conforming gauze bandage (e.g., Kling or Kerlix), applied with firm, even tension. Care must be taken to avoid a tourniquet effect at the proximal edge of the dressing.
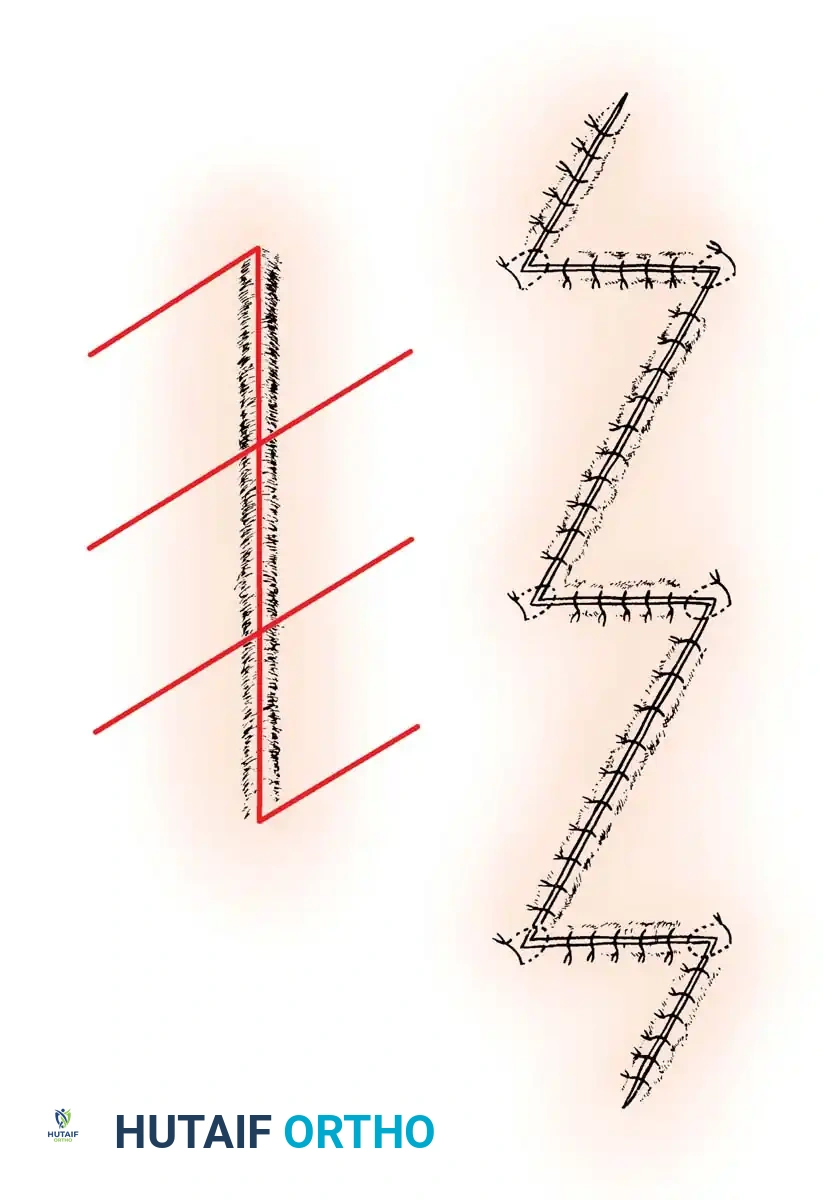
Surgical planning for scar optimization is a critical component of the operative technique that directly impacts postoperative rehabilitation. Linear scars that cross flexion creases perpendicularly (e.g., across the volar PIP joint or the wrist crease) are prone to severe longitudinal hypertrophy and contracture. As the scar matures and shortens, it acts as a restrictive bowstring, severely limiting joint extension. When a surgeon is faced with a traumatic laceration that crosses a crease, or when planning an extensive exposure, the integration of multiple Z-plasties is mandatory.
As illustrated above, the execution of multiple Z-plasties effectively breaks up the linear tension of a long scar. By transposing the triangular flaps, the contractile forces are redistributed laterally, and the overall longitudinal length of the scar line is significantly increased. This technique is invaluable in postoperative rehabilitation; it prevents the formation of a rigid, linear tether, allowing the hand therapist to initiate earlier and more aggressive range of motion protocols without the risk of wound dehiscence or the development of a debilitating flexion contracture.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and rigorous postoperative protocols, complications in hand surgery can and do occur. The ability to recognize these complications early and institute aggressive salvage management is the hallmark of an expert hand surgeon. Complications can be broadly categorized into vascular (hematoma, ischemia), infectious, biomechanical (stiffness, adhesions), and neurological (CRPS). Wound surveillance is critical; even when no complications are suspected, inspecting the wound at approximately 7 days postoperatively is a highly recommended practice. This "window" inspection allows for the timely management of unexpected superficial infections, marginal skin necrosis, or suture line dehiscence.
Hematoma formation is perhaps the most immediate and devastating postoperative complication. It occurs due to inadequate hemostasis prior to closure, failure to elevate the extremity during tourniquet deflation, or the premature initiation of dependent positioning. A hematoma acts as a culture medium for bacteria, vastly increasing the risk of deep space infection. Furthermore, the breakdown products of blood are highly irritating to synovial tissues, provoking a massive inflammatory response that inevitably leads to dense, restrictive adhesions. If a significant hematoma is clinically suspected (manifesting as throbbing pain, excessive swelling, or ecchymosis extending beyond the dressing), the dressing must be opened immediately under sterile conditions. The wound may require partial opening to evacuate the clot, followed by copious irrigation and re-suturing or healing by secondary intention.
Infection in the postoperative hand can rapidly destroy gliding mechanisms and articular cartilage. Superficial cellulitis may be managed with empirical oral antibiotics targeting Staphylococcus and Streptococcus species. However, deep space infections (e.g., suppurative flexor tenosynovitis, deep palmar space abscesses) represent surgical emergencies. The incidence of deep infection following clean elective hand surgery should be less than 1-2%, but this rises significantly in traumatic open injuries. Salvage management for deep infections mandates immediate return to the operating room for radical debridement, copious pulsatile lavage, and the potential insertion of antibiotic-impregnated polymethylmethacrylate (PMMA) beads, followed by targeted intravenous antibiotic therapy based on intraoperative cultures.
Complex Regional Pain Syndrome (CRPS), formerly known as Reflex Sympathetic Dystrophy (RSD), is a devastating neuropathic complication characterized by severe, out-of-proportion burning pain, sudomotor changes (hyperhidrosis or anhidrosis), vasomotor instability (temperature and color asymmetry), and trophic changes to the skin and nails. The incidence of CRPS is notably high following distal radius fractures (up to 10%) and severe crush injuries. Early recognition is paramount. Salvage management requires a multidisciplinary approach involving the surgeon, pain management specialists, and hand therapists. Modalities include aggressive active range of motion (avoiding passive pain-inducing stretches), desensitization protocols, pharmacological intervention (gabapentinoids, tricyclic antidepressants, short-course corticosteroids), and in refractory cases, stellate ganglion blocks.
| Complication | Estimated Incidence | Clinical Presentation | Salvage Management / Intervention |
|---|---|---|---|
| Hematoma | 2 - 5% | Throbbing pain, tight/bulging dressing, excessive ecchymosis, decreased capillary refill. | Immediate sterile dressing removal. Evacuation of clot, potentially requiring partial suture removal. Strict elevation. |
| Deep Space Infection | 1 - 3% (Higher in trauma) | Erythema, systemic fever, malodor, severe pain on passive stretch (Kanavel's signs). | Surgical emergency. Immediate I&D in the OR, copious lavage, culture-directed IV antibiotics, delayed closure. |
| Tendon Adhesions / Stiffness | 15 - 30% (Zone II flexor repairs) | Failure to progress in active ROM, discrepancy between active and passive motion. | Intensive hand therapy, dynamic splinting. Surgical tenolysis or capsulotomy delayed until tissues reach biological equilibrium (usually 3-6 months post-op). |
| Complex Regional Pain Syndrome (CRPS) | 5 - 10% (Distal radius/crush) | Out-of-proportion burning pain, allodynia, sudomotor/vasomotor changes, trophic skin changes. | Multidisciplinary approach: aggressive active ROM, desensitization, gabapentinoids, vitamin C prophylaxis, stellate ganglion blocks. |
| Marginal Skin Necrosis | 2 - 4% | Dark, eschar-forming wound edges, delayed healing, exposed underlying structures. | Observation if superficial. Surgical debridement and local flap coverage or skin grafting if deep structures (tendon/bone) are exposed. |
Phased Post-Operative Rehabilitation Protocols
The transition from immobilization to active rehabilitation must be meticulously guided by the biological timeline of tissue healing. Rehabilitation is not a monolithic entity but rather a phased progression that respects the shifting mechanical strength of the surgical repair. Active use of the hand is unequivocally the most effective way to reestablish motion after surgery, but this must be balanced against the risk of structural failure. The development of the specialized field of hand therapy has been of immeasurable importance in assisting patients in this complex recovery process. The patient, the hand therapist, and the surgeon must function as a well-integrated team, with the surgeon taking the lead in prescribing specific biomechanical limitations.
Phase I encompasses the Inflammatory and Early Fibroblastic stages (Days 1 to 14). The primary objectives during this phase are the absolute control of edema, the protection of the surgical repair, and the initiation of controlled motion in unaffected joints. Strict elevation protocols are enforced. If EAM is indicated (e.g., following a robust flexor tendon repair), it is initiated under the direct supervision of the hand therapist using highly specific orthoses (such as a dorsal blocking splint). A critical, yet often neglected, aspect of Phase I is proximal joint management. Fingers that are not explicitly splinted for protection should be exercised actively and frequently. Furthermore, the shoulder is highly susceptible to becoming stiff (adhesive capsulitis), especially in older patients holding their arm in a protective posture. The shoulder must be abducted and elevated toward the head through a full range of motion several times daily. Patients should be instructed to link these exercises to a recurring daily event, such as mealtimes, to build a reliable habit.
Phase II represents the Late Fibroblastic and Early Remodeling stages (Weeks 3 to 6). During this period, collagen synthesis is highly active, and the scar tissue is highly responsive to mechanical stress. The therapy protocols transition from passive or strictly protected active motion to more robust active range of motion (AROM) and active-assisted modalities. Dynamic splinting may be introduced to address specific joint contractures or to provide a prolonged, low-load stretch to maturing scar tissue. A cardinal rule must be observed during this phase: pain is a biological guide. The patient should never be required to carry out movements that are markedly painful. While mild discomfort and a stretching sensation are expected, sharp or severe pain is a warning sign of impending tissue failure, tendon subluxation, or complex regional pain syndrome. Motion must be regained allowing the patient's own pain threshold to dictate the limits of the stretch.
Phase III is the Late Remodeling and Functional Integration phase (Weeks 6 to 12 and beyond). The biological construct is now mechanically stable, and the focus shifts entirely to maximizing tendon excursion, increasing grip and pinch strength, and reintegrating the hand into activities of daily living (ADLs). Work conditioning and work hardening programs are implemented. Often, the most effective occupational therapy is the patient’s usual work. If biomechanically safe, patients should be offered the opportunity to return to work on a limited, light-duty, or modified basis. This return to the vocational environment provides continuous, functional AROM. Furthermore, it has a profoundly beneficial psychological effect, preventing the depression, anxiety, and loss of identity that frequently accompany prolonged disability, thereby driving vastly superior overall clinical outcomes.
Summary of Landmark Literature and Clinical Guidelines
The evolution of postoperative hand management is built upon a foundation of landmark anatomical studies and rigorous clinical trials. The fundamental principles of immobilization were championed by Sterling Bunnell and J.I.P. James in the mid-20th century. James meticulously described the "position of safe immobilization" (the intrinsic-plus position), providing the anatomical and biomechanical rationale for flexing the MCP joints and extending the IP joints to prevent catastrophic collateral ligament and volar plate contractures. This principle remains the absolute, inviolable cornerstone of modern hand surgery dressing and splinting protocols.
In the realm of tendon rehabilitation, the paradigm shift from prolonged static immobilization to early controlled motion was driven by the pioneering work of Kleinert, Duran, and Houser. Kleinert introduced the concept of dynamic traction, utilizing rubber bands to passively flex the digits while allowing active extension within a dorsal blocking splint. This protocol demonstrated that controlled stress significantly reduced adhesion formation in Zone II flexor tendon repairs while stimulating intrinsic tenocyte proliferation. Subsequent biomechanical studies by Strickland and Gelberman further refined these concepts, proving that early active motion (EAM), when paired with multi-strand core suture techniques, yields superior ultimate tendon excursion and tensile strength compared to passive protocols.
Modern clinical guidelines, supported by the American Society for Surgery of the Hand (ASSH) and the European Federation of Societies for Surgery of the Hand (FESSH), strongly advocate for the multidisciplinary approach detailed in this chapter. Current evidence-based literature emphasizes the critical importance of immediate postoperative edema control, highlighting that interstitial fluid accumulation is the primary catalyst for fibrosis. Furthermore, contemporary guidelines stress the psychological and economic imperatives of early vocational rehabilitation, demonstrating that structured, modified return-to-work programs significantly reduce the incidence of chronic pain syndromes and long-term disability in the hand surgery patient population.
