Cleft Hand Reconstruction: Miura-Komada and Ueba Techniques
Key Takeaway
Cleft hand reconstruction requires meticulous surgical planning to restore both function and aesthetics. The Miura-Komada and Ueba techniques are cornerstone procedures for cleft closure and the release of thumb adduction contractures. These approaches utilize strategic skin flaps, metacarpal transposition, and soft-tissue balancing to deepen the first web space, reconstruct the transverse metacarpal ligament, and optimize digital biomechanics for superior long-term functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
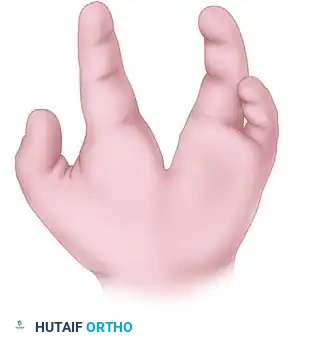
Typical cleft hand, historically and somewhat pejoratively referred to as ectrodactyly or split hand malformation, represents a profoundly complex congenital longitudinal deficiency. This rare anomaly is morphologically characterized by the absence of central rays (most frequently the third ray), the presence of a deep V-shaped central cleft extending proximally into the metacarpal region, and frequently, concomitant syndactyly of the border digits. The condition falls under the broader umbrella of Split Hand/Foot Malformation (SHFM), a genetically heterogeneous disorder that manifests with remarkable phenotypic variability. While the morphological absence of the central digits is the most visually striking feature, the functional impairment in a cleft hand is rarely dictated by the missing digits alone. Instead, the profound functional deficits are driven by the secondary deformities, most notably the progressive adduction contracture of the thumb and the malrotation of the index ray.
The embryological pathogenesis of the typical cleft hand involves a central failure of the apical ectodermal ridge (AER) during the critical period of limb bud development, typically occurring between the fourth and seventh weeks of gestation. The AER is the primary signaling center responsible for the proximodistal outgrowth and patterning of the limb. A localized, wedge-shaped defect in the AER leads to the cessation of signaling molecules, particularly Fibroblast Growth Factors (FGFs), resulting in the failure of the central mesenchyme to differentiate into the central rays. Unlike atypical cleft hands (symbrachydactyly), which are usually unilateral, sporadic, and associated with a U-shaped defect and rudimentary nubbins, typical cleft hands are frequently bilateral and often involve the feet.
Epidemiologically, typical cleft hand is a rare entity, with an estimated incidence of approximately 1 in 90,000 to 100,000 live births. The genetic underpinnings are highly complex and predominantly exhibit an autosomal dominant pattern of inheritance with incomplete penetrance and variable expressivity. Advancements in molecular genetics have identified at least six distinct chromosomal loci associated with SHFM (SHFM1 through SHFM6). Key genes implicated in the pathogenesis include DLX5, DLX6, TP63, and WNT10b. Mutations in TP63 (SHFM4) are particularly notable as they can present syndromically, such as in Ectrodactyly-Ectodermal Dysplasia-Clefting (EEC) syndrome. For the orthopedic surgeon, understanding this genetic and syndromic association is critical, as it necessitates a comprehensive multidisciplinary evaluation prior to any surgical intervention, ensuring that concomitant systemic, craniofacial, or renal anomalies are appropriately managed.
The natural history of an untreated typical cleft hand is one of progressive functional deterioration. As the child grows, the anomalous fibrous bands within the cleft and the unopposed pull of the contracted adductor pollicis muscle exacerbate the thumb adduction contracture. This progressive collapse of the first web space obliterates the functional span of the hand, severely compromising the child's ability to perform large object grasp and refined tip-to-tip pinch. Consequently, surgical intervention is not merely an aesthetic endeavor but a crucial functional necessity aimed at fundamentally altering the biomechanical trajectory of the developing hand.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the aberrant surgical anatomy is the cornerstone of successful cleft hand reconstruction. The typical cleft hand presents a highly variable skeletal landscape. While the phalanges of the third ray are invariably absent, the third metacarpal is frequently present to varying degrees. Most commonly, the proximal base of the third metacarpal is preserved, articulating normally with the capitate. This remnant plays a pivotal role in surgical reconstruction, serving as an optimal, robust docking site for the transposition of the index ray. The deep V-shaped cleft extends proximally, dividing the hand into distinct radial and ulnar functional units. The border digits (thumb/index and ring/small fingers) frequently exhibit complex syndactyly, which further tethers the functional units and complicates the reconstructive algorithm.
The muscular and fascial anatomy of the cleft hand is characterized by significant pathological alterations that directly drive the biomechanical collapse of the hand. The most functionally limiting secondary deformity is the thumb adduction contracture. In a normal hand, the central rays provide a structural buttress that maintains the transverse metacarpal arch and supports the first web space. The absence of the central ray removes this critical keystone. Consequently, the index ray drifts ulnarward, and the thumb collapses into the palm. This skeletal instability is severely exacerbated by anomalous, unyielding fibrous bands known as "cleft bands," which span the defect and tether the thumb to the index or ring finger. Furthermore, the adductor pollicis muscle becomes structurally contracted, and the first dorsal interosseous muscle is often shortened, fibrotic, or anomalously inserted, creating an insurmountable mechanical block to thumb abduction and opposition.
Neurovascular anomalies are ubiquitous in the cleft hand and pose the greatest intraoperative risk during reconstruction. The superficial palmar arch is frequently incomplete or entirely absent. The arterial supply to the border digits bordering the cleft (the ulnar aspect of the index and the radial aspect of the ring finger) may be derived from a single, dominant anomalous vessel coursing directly through the central cleft. Similarly, the common digital nerves frequently bifurcate more proximally than normal or exhibit anomalous branching patterns, traversing the redundant skin of the cleft. Meticulous, loupe-assisted dissection is mandatory to identify and protect these vital structures before any fascial release or metacarpal osteotomy is performed. Injury to a dominant anomalous vessel during cleft closure can result in catastrophic ischemic necrosis of the transposed digit.
Biomechanically, surgical intervention aims to restore three primary functional pillars. First, closure of the central cleft is required to restore the transverse metacarpal arch, which is essential for cupping the hand and stabilizing the metacarpophalangeal joints. Second, aggressive release of the thumb adduction contracture is paramount to widen the first web space, thereby restoring the functional span required for opposition and cylindrical grasp. Third, realignment of the index ray is critical to prevent digital overlapping, or "scissoring," during active flexion. Because the natural flexion arc of the normal index finger is directed toward the scaphoid tubercle, an ulnarward transposition of the index metacarpal without concomitant rotational correction (supination) will inevitably cause the index finger to cross over the ring finger, severely impairing grip mechanics.
Exhaustive Indications and Contraindications
The decision-making process for surgical reconstruction of a cleft hand is highly nuanced and must be individualized based on the severity of the functional deficit, the specific anatomical variant, and the developmental stage of the child. The Manske and Halikis classification system is the most widely utilized framework for guiding surgical indications. This system categorizes cleft hands based on the status of the first web space, which is the primary determinant of hand function. Type I hands have a normal first web space; Type II have a mildly narrowed space; Type III have a severely narrowed space (often with syndactyly of the thumb and index finger); Type IV lack a first web space entirely (the thumb and index are completely syndactylized); and Type V lack a thumb altogether.
Surgical intervention is definitively indicated for Manske Types II, III, and IV, where the thumb adduction contracture significantly impairs grasp, pinch, and overall hand function. The primary goals are functional restoration and the prevention of progressive deformity. Aesthetic improvement, while a secondary benefit that significantly impacts the psychosocial well-being of the child, should never supersede functional considerations. The optimal timing for reconstruction is typically between 12 and 18 months of age. Surgery at this critical developmental juncture capitalizes on the child's immense neuroplasticity, allowing for rapid functional adaptation and cortical remapping of the reconstructed hand, while ensuring that the anatomical structures are sufficiently large to permit meticulous, safe surgical handling.
Contraindications to complex cleft hand reconstruction are relatively few but absolute when present. Severe, global hypoplasia of the hand where surgical intervention will not yield any meaningful improvement in prehension is a primary contraindication. In such cases, the child often develops highly effective, albeit atypical, compensatory grasp patterns that should not be disrupted by surgically enforced anatomical normalization. Additionally, mild atypical clefts (symbrachydactyly) with excellent baseline function and no progressive contracture may be managed non-operatively. Furthermore, any severe concomitant systemic or syndromic anomalies that render the child an unacceptably high anesthetic risk must preclude elective orthopedic reconstruction until medical optimization is achieved.
| Parameter | Indications for Reconstruction | Contraindications for Reconstruction |
|---|---|---|
| Functional Deficit | Progressive thumb adduction contracture; inability to perform large object grasp; severe impairment of tip-to-tip pinch. | Excellent compensatory function despite anatomical abnormality; functional stability without progression. |
| Manske Classification | Manske Types II, III, and IV (narrowed or absent first web space). | Manske Type I (normal web space) with minimal clefting; Manske Type V (absent thumb) requiring pollicization rather than cleft closure. |
| Anatomical Factors | Presence of a functional index ray; adequate proximal 3rd metacarpal base for docking; syndactyly requiring release. | Severe global hypoplasia; absent proximal 3rd metacarpal base combined with severe vascular anomalies precluding transfer. |
| Patient Factors | Age 12-18 months (optimal window for neuroplasticity); severe psychosocial stigma affecting development. | Medically unstable patient; severe cardiopulmonary syndromic anomalies; lack of postoperative therapy support. |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive preoperative planning is the absolute prerequisite for a successful cleft hand reconstruction. The clinical evaluation must rigorously assess the functional capacity of the hand, focusing on pinch strength, grasp mechanics, and the active tracking of the digits during flexion and extension. The surgeon must carefully palpate the first web space to ascertain the severity of the adductor contracture and identify any palpable anomalous fibrous bands. If concomitant syndactyly is present, the flexibility of the tethered digits must be evaluated to determine if syndactyly release should be staged or performed simultaneously with the cleft closure, though simultaneous procedures increase the risk of vascular compromise.
Radiographic evaluation is mandatory and forms the basis of surgical templating. High-quality, orthogonal plain radiographs (anteroposterior, lateral, and oblique views) of the bilateral hands and wrists are obtained to delineate the skeletal anatomy. The surgeon must specifically evaluate the presence, size, and morphology of the third metacarpal base, as this will dictate the docking site for the index ray transposition. The angulation of the index and ring metacarpals should be measured to plan the necessary osteotomies. In highly complex or atypical cases where vascular anomalies are strongly suspected, advanced imaging modalities such as Magnetic Resonance Angiography (MRA) or high-resolution Doppler ultrasonography may be indicated to map the superficial and deep palmar arches and identify dominant anomalous vessels traversing the cleft.
Surgical templating involves the precise mapping of the proposed incisions and skin flaps. The choice between the Miura-Komada technique and the Ueba technique is heavily influenced by the specific morphology of the cleft and the severity of the rotational deformity of the index ray. The surgeon should mentally rehearse the flap transpositions, ensuring that the redundant skin of the cleft can be adequately mobilized to line the deepened first web space without excessive tension. The planned trajectory of the index metacarpal transposition must be templated to ensure that the resultant digital tracking will be parallel to the scaphoid tubercle.
Patient positioning and intraoperative setup must be optimized for meticulous pediatric hand surgery. The patient is placed supine on the operating table with the operative arm extended onto a radiolucent hand table, allowing for unhindered fluoroscopic access. General anesthesia is required, and a well-padded pneumatic pediatric upper arm tourniquet is applied. The tourniquet is typically inflated to 100 mmHg above the patient's systolic blood pressure after thorough exsanguination of the limb using an Esmarch bandage. High-quality surgical loupe magnification (minimum 2.5x to 3.5x) and specialized pediatric hand instruments are absolute necessities for the safe identification and mobilization of the delicate neurovascular bundles and the execution of precise osteotomies.
Step-by-Step Surgical Approach and Fixation Technique
The surgical reconstruction of the cleft hand requires a masterful orchestration of soft tissue rearrangement, skeletal realignment, and ligamentous reconstruction. The Miura and Komada technique and the Ueba technique represent two highly sophisticated, evidence-based approaches designed to achieve the triad of cleft closure, thumb web space widening, and index ray realignment. The selection of the specific technique depends on the surgeon's preference, the availability of local tissue, and the degree of rotational correction required for the index ray.
The Miura and Komada Technique
The Miura and Komada technique is a powerful reconstructive option that utilizes a combination of dorsal and palmar incisions to simultaneously address the central cleft and the narrowed first web space. This technique leverages the redundant skin of the cleft to deepen the thumb web, while transposing the index ray ulnarward to close the central defect.
1. Incision Design and Flap Elevation: The procedure commences with the design of a linear incision beginning on the radial aspect of the base of the ring finger, extending continuously to the ulnar side of the base of the index finger, crossing directly through the cleft space. A second, curved incision is designed around the base of the index finger, with its apex corresponding to the desired depth of the newly reconstructed thumb web space. The skin flaps are meticulously elevated, taking extreme care to preserve the subdermal vascular plexus. Marginal necrosis of these delicate flaps is a catastrophic complication that can lead to severe contractures.
2. Metacarpal Detachment and Muscle Release: The base of the index (second) metacarpal is identified through a subperiosteal dissection. The metacarpal is detached at its base. Crucially, the first dorsal interosseous muscle must be mobilized and partially detached along with the metacarpal to allow for a tension-free transposition. If visualization is inadequate, an additional longitudinal dorsal skin incision centered over the bases of the index and third metacarpals is utilized as an exposure adjunct.
3. Release of the Thumb Adduction Contracture: The tight fascial bands contributing to the narrowed first web space are systematically identified and excised. The fascia of the adductor pollicis muscle and the first dorsal interosseous muscle is aggressively released. In severe cases, a fractional lengthening or partial release of the adductor pollicis origin from the third metacarpal is necessary to achieve a fully abducted thumb posture. Strict hemostasis and direct visualization of the neurovascular structures are mandatory before transecting any deep fascial bands.
4. Skeletal Stabilization and Ligamentous Reconstruction: The transposed index ray is impaled onto the base of the third metacarpal, which serves as the ideal docking site. Rigid skeletal fixation is achieved using two crossed or parallel smooth Kirschner wires (0.045 or 0.062 inches). The rotation of the index ray must be anatomically aligned to prevent scissoring. To prevent future splaying of the reconstructed hand, the deep transverse metacarpal ligament is recreated by placing heavy, nonabsorbable sutures (e.g., 3-0 Ethibond) between the volar plates and deep fascial tissues of the index and ring fingers. The redundant cleft skin is then transposed radially to line the deepened first web, and the wounds are closed meticulously.
The Ueba Technique
The Ueba technique is a highly sophisticated alternative that utilizes a specialized palmar approach and an interdigital flap to reconstruct the commissure. This technique is particularly advantageous when addressing severe rotational deformities of the index ray, as it explicitly incorporates metacarpal supination and extensor tendon reconstruction to optimize digital tracking.
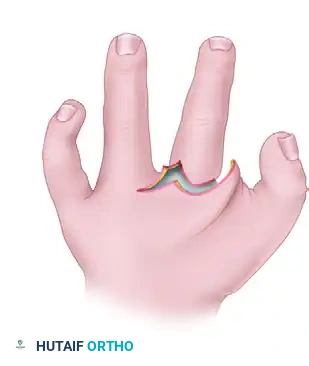
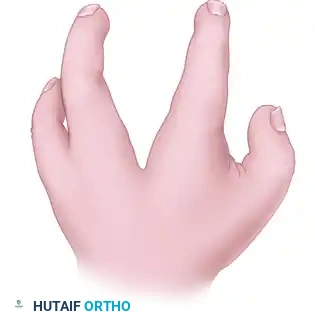
1. Incision Design and Flap Creation: The Ueba technique begins with the design of a V-shaped skin incision forming a triangular skin flap on the radial side of the ring finger. This critical flap will be transposed to form the new, smooth commissure between the index and ring fingers.
(Fig. 79-32A: Dorsal view of incisions. Solid lines indicate dorsal incisions; broken lines indicate palmar incisions.)
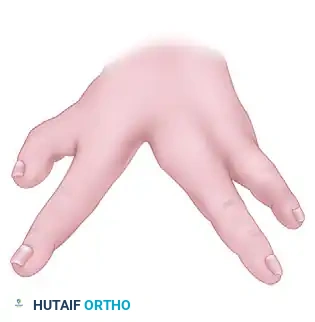
A second transverse incision extends from the palmar end of the V-shaped incision to the ulnar side of the palm.
(Fig. 79-32B: Palmar view of incisions. Solid lines indicate palmar incisions; broken lines indicate dorsal incisions.)
A third incision curves around the base of the index finger, connecting at the bottom of the cleft to allow complete mobilization.
(Fig. 79-32C: Incisions from the web space. Solid lines indicate dorsal incisions; broken lines indicate palmar incisions.)
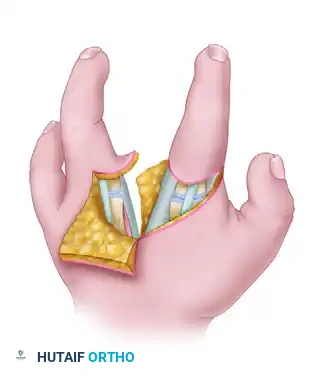
2. Flap Elevation and Contracture Release: The interdigital palmar and dorsal skin flaps are carefully elevated. The unyielding fibrous bands located between the thumb and the index finger are identified and severed, widening the thumb web space to its maximum anatomical potential.
(Fig. 79-32D: Flaps developed and elevated, exposing the underlying anomalous fibrous bands and skeletal anatomy.)
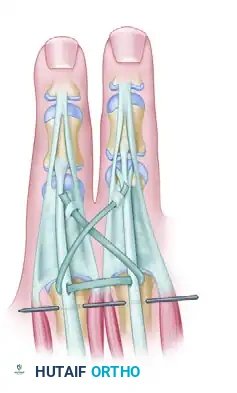
3. Metacarpal Transfer and The Supination Maneuver: The periosteum is incised circumferentially around the second metacarpal. An osteotomy is performed to transfer the metacarpal ulnarward toward the fourth metacarpal. The critical maneuver in the Ueba technique is the supination of the second metacarpal during transfer. Because the natural flexion arc of the index finger is directed toward the scaphoid, moving its base ulnarward without rotational correction will cause the index finger to cross over the ring finger. Supinating the metacarpal corrects this trajectory. The transposed metacarpal is fixed to the fourth metacarpal using smooth Kirschner wires, and the transverse metacarpal arch is reconstructed with heavy circumferential sutures.
4. Extensor Tendon Reconstruction and Flap Inset: To prevent an extensor lag or ulnar subluxation of the tendon due to the transposition, a free tendon graft from the palmaris longus is harvested. This graft connects the common extensor tendons of the index and ring fingers, passed transversely through the substance of the tendons at the MCP joint level and secured with a Pulvertaft weave.
(Fig. 79-32E: Reconstruction of the extensor tendon with a palmaris longus graft; Kirschner wire stabilizes the index to the ring metacarpal.)
The previously elevated flaps are then rotated into position. The triangular flap from the ring finger is inset to create a smooth, U-shaped commissure.
(Fig. 79-32F: Flaps rotated into position, demonstrating the obliteration of the cleft and the creation of the new commissure.)
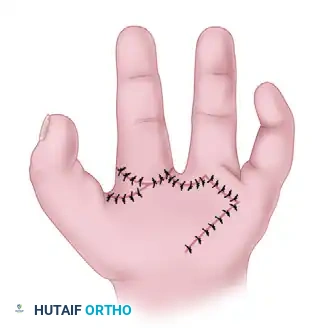
The final suture lines are designed transversely to conceal the original longitudinal cleft and deepen the first web space, followed by the application of a well-molded long-arm cast.
(Fig. 79-32G: Final appearance of the palm after wound closure, showing a deepened first web space and a closed central cleft.)
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, cleft hand reconstruction carries a significant risk of postoperative complications, primarily due to the profound anatomical anomalies and the extensive soft tissue mobilization required. The most devastating early complication is vascular compromise leading to partial or complete flap necrosis. This typically occurs due to excessive tension on the transposed skin flaps, unrecognized injury to an anomalous dominant blood vessel during cleft dissection, or aggressive tourniquet times. Marginal flap necrosis can often be managed with diligent local wound care and secondary intention healing, but full-thickness necrosis requires urgent surgical debridement and subsequent coverage with full-thickness skin grafts or local rotational flaps to prevent severe secondary contractures.
Infection, particularly pin tract infection associated with the Kirschner wires used for skeletal stabilization, is a moderately common complication. Superficial pin tract infections can usually be managed effectively with a short course of oral antibiotics and enhanced local pin care. However, deep infections tracking into the osteotomy site or the newly reconstructed transverse metacarpal ligament are limb-threatening emergencies. Such deep infections mandate immediate hardware removal, aggressive surgical irrigation and debridement, and prolonged intravenous antibiotic therapy, often resulting in a loss of the achieved skeletal reduction and necessitating complex secondary reconstructive efforts once the infection is eradicated.
The most common late functional complication is digital scissoring, characterized by the overlapping of the index and ring fingers during active flexion. This complication is almost exclusively the result of a failure to adequately supinate the index metacarpal during its ulnarward transposition. If scissoring is severe and functionally limiting, salvage management requires a secondary rotational osteotomy of the index metacarpal to correct the trajectory. Another frequent late complication is the recurrence of the thumb adduction contracture. This occurs due to inadequate initial release of the adductor pollicis, failure to reconstruct the transverse metacarpal ligament, or poor compliance with postoperative night splinting. Recurrent contractures may necessitate a secondary first web space deepening procedure, often requiring a dorsal rotation flap or a full-thickness skin graft, combined with a repeat, more aggressive adductor release.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment |
|---|---|---|---|
| Flap Necrosis (Marginal/Partial) | 5% - 10% | Excessive tension on closure; poor flap design; unrecognized anomalous vascularity. | Local wound care; delayed full-thickness skin grafting if contracture develops. |
| Pin Tract Infection (Superficial) | 10% - 15% | Prolonged K-wire retention; poor cast hygiene. | Oral antibiotics; enhanced local pin care; early pin removal if consolidated. |
| Digital Scissoring (Overlapping) | 15% - 20% | Failure to perform the supination maneuver during index ray transposition. | Secondary rotational osteotomy of the index metacarpal. |
| Recurrent Adduction Contracture | 20% - 30% | Inadequate initial adductor release; failure of transverse ligament repair; non-compliance with splinting. | Secondary web space release; Z-plasty or dorsal rotation flap; repeat adductor tenotomy. |
| Loss of Skeletal Reduction | < 5% | Premature pin removal; inadequate initial K-wire fixation; deep infection. | Revision open reduction and internal fixation; potential bone grafting if nonunion occurs. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a complex cleft hand reconstruction is as critical to the final functional outcome as the surgical procedure itself. The rehabilitation protocol must be meticulously phased, balancing the need for rigid immobilization to allow for osseous and soft tissue healing with the imperative to initiate early motion to prevent devastating joint stiffness and tendon adhesions. The protocol is heavily reliant on the expertise of a specialized pediatric hand therapist and requires immense dedication and compliance from the patient's parents or caregivers.
Phase 1: Maximum Protection (Weeks 0 to 3)
Immediately postoperatively, the hand is immobilized in a bulky, non-adherent dressing and a well-molded, fiberglass long-arm cast. The cast must extend above the elbow to control forearm rotation and must be expertly molded in the intermetacarpal space to compress the transposed rays and prevent any separation of the newly closed cleft. The primary goals during this phase are strict edema control, protection of the delicate skin flaps, and maintenance of the skeletal reduction. The arm should be kept strictly elevated. At exactly three weeks postoperatively, the patient is evaluated in the clinic, often under mild sedation or in the operating room, to safely remove the initial cast and any non-absorbable skin sutures without traumatizing the healing wounds.
Phase 2: Protected Mobilization (Weeks 3 to 6)
At the three-week mark, assuming the skin flaps are completely healed and there is no evidence of infection, a secondary, well-molded short-arm cast or a custom-fabricated thermoplastic splint is applied. This secondary immobilization continues to protect the Kirschner wires and the healing extensor tendon graft (if the Ueba technique was utilized). During this phase, early, gentle passive range of motion (PROM) of the interphalangeal joints may be initiated by the hand therapist, provided the metacarpophalangeal joints remain strictly stabilized. The cast and Kirschner wires are typically removed at approximately six weeks postoperatively, entirely contingent upon definitive radiographic evidence of complete osseous consolidation at the transposition site.
Phase 3: Active Functional Integration (Weeks 6 to 12)
Following the removal of all hardware, the patient enters the active rehabilitation phase. The focus shifts dramatically toward restoring active range of motion (AROM), integrating the reconstructed hand into daily activities, and promoting cortical remapping. The pediatric hand therapist employs play-based therapy techniques to encourage large object grasp, cylindrical grip, and refined tip-to-tip pinch. Scar management techniques, including silicone gel sheeting and deep friction massage, are initiated to prevent the formation of restrictive hypertrophic scars within the first web space.
Phase 4: Long-Term Maintenance (Months 3 to 12+)
The final phase of rehabilitation is focused on the long-term maintenance of the achieved functional gains and the prevention of recurrent deformities, particularly the thumb adduction contracture. Night splinting of the first web space in a position of maximum abduction and opposition is often mandated for up to six months, and sometimes longer during periods of rapid skeletal growth. The child must be monitored longitudinally by the orthopedic surgeon, with clinical and radiographic evaluations scheduled at regular intervals to assess for any late manifestations of digital scissoring, growth arrest, or recurrence of the central cleft diastasis.
Summary of Landmark Literature and Clinical Guidelines
The evolution of cleft hand reconstruction has been shaped by a series of landmark anatomical studies and innovative surgical descriptions. Historically, the management of the cleft hand was highly variable, often relying on simple soft tissue syndactylization (the "Snow-Littler" procedure), which frequently failed to address the underlying skeletal instability and predictably resulted in recurrent central diastasis and severe adduction contractures. The modern era of cleft hand reconstruction is defined by a biomechanical approach that mandates skeletal transposition and rigid ligamentous reconstruction.
The foundational framework for surgical decision-making was established by Manske and Halikis in 1995. Their seminal publication in the Journal of Hand Surgery introduced a classification system based entirely on the morphology and functional capacity of the first web space, shifting the paradigm away from purely descriptive anatomical classifications. This system remains the universally accepted standard for determining surgical indications, emphasizing that the primary goal of intervention is the restoration of thumb opposition and functional grasp.
The technical execution of cleft closure was revolutionized by Miura and Komada in 1979. Their description of transposing the index ray to the base of the third metacarpal, combined with the utilization of the cleft skin to deepen the first web space, provided a reliable, reproducible method for restoring the transverse metacarpal arch. Subsequently, in 1981, Ueba introduced his sophisticated palmar approach, which specifically addressed the critical issue of digital scissoring. Ueba's emphasis on the mandatory supination of the index metacarpal during transfer and the concomitant reconstruction of the extensor mechanism represented a massive leap forward in optimizing the dynamic tracking of the reconstructed digits. Current clinical guidelines, supported by the Pediatric Orthopaedic Society of North America (POSNA) and the American Society for Surgery of the Hand (ASSH), strongly endorse these techniques, recommending intervention between 12 and 18 months of age to maximize neuroplastic adaptation and ensure optimal long-term functional outcomes.
