Zancolli Reconstruction for Tetraplegia: Surgical Guide
Key Takeaway
The Zancolli reconstruction is a two-stage surgical technique designed to restore hand function in patients with C6 tetraplegia. The first stage establishes active finger and thumb extension alongside thumb stabilization. The second stage, performed four to six months later, restores active grasp and pinch through synergistic tendon transfers. This evidence-based guide details the biomechanics, step-by-step surgical approaches, and postoperative protocols essential for optimizing functional outcomes in the tetraplegic hand.
Comprehensive Introduction and Patho-Epidemiology
The restoration of upper extremity function in the tetraplegic patient represents one of the most profound and technically demanding interventions in reconstructive orthopedic and hand surgery. For individuals who have sustained a cervical spinal cord injury, particularly at the C6 neurological level, the sudden and catastrophic loss of prehension, grasp, and pinch fundamentally devastates their functional independence and quality of life. Extensive epidemiological surveys and patient-reported outcome metrics consistently demonstrate that tetraplegic patients prioritize the recovery of hand and arm function above all other neurological deficits, including bowel, bladder, and sexual function, as well as the ability to walk. The preservation of active, strong wrist extension in the C6 tetraplegic—typically mediated by the extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB)—provides a critical biomechanical foundation upon which reconstructive surgeons can build a functional hand.
Eduardo Zancolli revolutionized the surgical management of the tetraplegic upper extremity by pioneering a highly systematic, two-step reconstructive technique designed specifically for this unique patient population. Prior to Zancolli’s formalized approach, single-stage multi-tendon transfers frequently yielded suboptimal outcomes due to the simultaneous introduction of antagonistic forces. When a patient with profound upper motor neuron deficits is simultaneously presented with newly transferred flexors and extensors, the resulting cortical confusion often leads to co-contraction, profound stiffness, and ultimate failure of the reconstructive effort. Zancolli’s brilliance lay in his recognition that the cerebral re-education required to master a transferred muscle is best achieved sequentially.
The Zancolli reconstruction aims to restore two fundamental upper extremity functions in a staged manner. The first step is dedicated entirely to the restoration of active finger and thumb extension, coupled with critical stabilization of the thumb carpometacarpal (CMC) or metacarpophalangeal (MCP) joints. By isolating the extension phase, the patient can focus entirely on utilizing a donor muscle—typically the brachioradialis—to open the hand, relying on gravity and passive tenodesis for closure. Once the patient has successfully integrated this new motor pattern into their cortical schema, the second step is undertaken to restore active finger flexion and thumb flexion, thereby providing a powerful grasp and a functional key pinch.
Understanding the patho-epidemiology of cervical spinal cord injuries is essential for the reconstructive surgeon. The majority of these injuries occur secondary to high-energy trauma, such as motor vehicle collisions, falls from height, and diving accidents, predominantly affecting young males. The resulting neurological deficit is a complex amalgamation of upper motor neuron and lower motor neuron lesions. At the level of the injury, anterior horn cell destruction results in flaccid paralysis and profound muscle atrophy. Caudal to the injury level, the disruption of descending inhibitory pathways leads to spasticity, hyperreflexia, and synergistic mass movement patterns. The surgeon must meticulously evaluate the interplay between flaccidity and spasticity, as the presence of severe, uncontrollable spasticity can easily overpower even the most robust tendon transfer, leading to fixed contractures and functional failure.
Detailed Surgical Anatomy and Biomechanics
The success of the Zancolli reconstruction relies heavily on a profound understanding of the surgical anatomy of the forearm and hand, coupled with the precise manipulation of biomechanical principles, specifically the tenodesis effect and the length-tension relationship of transferred muscle-tendon units. The surgeon must evaluate not only the absolute strength of the donor muscles but also their physiological cross-sectional area (which determines force generation) and their resting fiber length (which determines excursion).
The brachioradialis (BR) is the workhorse donor muscle utilized in the first step of the Zancolli reconstruction to restore digital extension. Anatomically, the BR originates from the proximal two-thirds of the lateral supracondylar ridge of the humerus and inserts on the lateral surface of the distal radius. While the BR possesses a substantial cross-sectional area capable of generating significant force, its inherent excursion is notoriously limited, typically measuring approximately 30 millimeters. Because functional finger extension requires an excursion of at least 50 millimeters, the BR must undergo extensive proximal mobilization. The surgeon must meticulously release the dense fascial attachments tethering the BR to the underlying extensor carpi radialis longus and the radial shaft, dissecting proximally almost to its humeral origin while carefully preserving its neurovascular pedicle from the radial nerve, which enters the muscle in its proximal third.
The extensor carpi radialis longus (ECRL) and extensor carpi radialis brevis (ECRB) represent the critical motors for wrist extension, which is the sine qua non for the tenodesis effect. The ECRL inserts on the dorsal base of the second metacarpal, while the ECRB inserts on the dorsal base of the third metacarpal. Biomechanically, the centralized insertion of the ECRB makes it the primary and most efficient wrist extensor, generating pure extension without significant radial deviation. Consequently, in the Zancolli reconstruction, the ECRB must be rigorously preserved to maintain the active wrist extension necessary to drive the tenodesis effect. The ECRL, which acts more as a radial deviator and secondary wrist extensor, is therefore considered expendable and serves as the ideal donor muscle for transfer to the flexor digitorum profundus (FDP) in the second stage of the reconstruction. Its synergistic relationship with finger flexion makes motor re-education highly intuitive for the patient.
Joint stabilization principles form the final biomechanical pillar of the Zancolli procedure. In the paralyzed hand, transferring a tendon across an unstable, flaccid joint will inevitably result in joint collapse rather than the intended distal motion. This is particularly critical in the thumb ray. If the thumb CMC joint is unstable, the force generated by a transferred flexor pollicis longus (FPL) will cause the first metacarpal to collapse into the palm, completely negating the key pinch. Therefore, the thumb CMC joint or MCP joint must be stabilized during the first step of the procedure to provide a rigid, unyielding post against which the transferred tendons can effectively act. Understanding the complex saddle joint mechanics of the CMC joint and the volar plate anatomy of the MCP joint is essential for executing these stabilizing procedures effectively.
Exhaustive Indications and Contraindications
Patient selection is the most critical determinant of success in the surgical rehabilitation of the tetraplegic upper extremity. The Zancolli procedure is primarily indicated for patients classified with a C6 neurological level of function. However, chronological neurological levels often fail to accurately describe the specific muscular assets available for transfer. Therefore, the International Classification Scheme for Tetraplegia, established at the Edinburgh conference, is the gold standard for preoperative evaluation. This scheme classifies patients based on the number of muscles below the elbow that possess a Medical Research Council (MRC) grade of 4 or better, provided that the patient has intact sensibility (two-point discrimination of less than 10 mm) in the thumb and index finger.
The Zancolli two-stage reconstruction is the primary indication for patients falling into Groups 3, 4, and 5 of the International Classification Scheme. In Group 3, the patient possesses a strong ECRB in addition to the BR and ECRL, providing the minimum requisite motors to execute the classic Zancolli transfer. In Group 4, the addition of a strong pronator teres (PT) provides an excellent synergistic motor for finger or thumb flexion, offering the surgeon additional reconstructive options. Group 5 patients, who also possess a strong flexor carpi radialis (FCR), have even greater reconstructive potential, though the core tenets of the Zancolli two-stage approach remain highly applicable to prevent cortical confusion during rehabilitation.
| International Classification Group | Retained Motor Function Below Elbow (Grade ≥ 4) | Primary Surgical Reconstructive Options |
|---|---|---|
| Group 0 | None | Elbow extension restoration (e.g., Moberg posterior deltoid to triceps transfer). |
| Group 1 | Brachioradialis (BR) | Elbow extension; passive key grip (Moberg tenodesis). |
| Group 2 | Extensor Carpi Radialis Longus (ECRL) | Elbow extension; active wrist extension; passive key grip. |
| Group 3 | Extensor Carpi Radialis Brevis (ECRB) | Zancolli Two-Stage Reconstruction (Classic Indication). Active extension and active grasp/pinch. |
| Group 4 | Pronator Teres (PT) | Zancolli Two-Stage Reconstruction. PT available for FPL or FDP transfer. |
| Group 5 | Flexor Carpi Radialis (FCR) | Zancolli Two-Stage Reconstruction. FCR available for transfer; robust wrist control. |
| Group 6 | Finger Extensors (EDC) | Modified House procedure; single-stage flexor reconstruction. |
| Group 7 | Thumb Extensor (EPL) | House two-stage procedure; intrinsic balancing. |
| Group 8 | Partial Finger Flexors (FDP) | Zancolli two-stage or targeted intrinsic reconstruction. |
| Group 9 | Lacks only intrinsics | Opponensplasty; intrinsic tenodesis. |
Contraindications to the Zancolli reconstruction must be rigorously respected to prevent catastrophic outcomes. Severe, medically refractory spasticity in the upper extremity is an absolute contraindication, as spastic antagonist muscles will rapidly overpower the transferred tendons, leading to severe contractures and loss of function. Fixed joint contractures that cannot be corrected with preoperative serial casting or therapy also preclude successful tendon transfer, as the transferred muscle will lack the excursion necessary to overcome the mechanical block. Furthermore, poor patient cognition, lack of psychological readiness, or inability to comply with the grueling, months-long postoperative rehabilitation protocol are significant contraindications. The patient must possess the cognitive fortitude to engage in extensive cortical remapping exercises. Finally, a lack of adequate donor muscles (e.g., BR or ECRL graded less than MRC 4) or severe autonomic dysreflexia that prevents safe surgical intervention represent strict contraindications to this elective reconstructive procedure.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful Zancolli reconstruction. The initial clinical evaluation must involve repeated, meticulous manual muscle testing (MMT) of all upper extremity musculature. Because muscle strength in tetraplegia can fluctuate based on fatigue, positioning, and spasticity, MMT should be performed on multiple occasions to confirm that the donor muscles (BR, ECRL) consistently demonstrate an MRC grade of 4 or 5. The surgeon must carefully palpate the BR during resisted elbow flexion to assess its bulk and excursion potential. Additionally, a critical assessment of the "supple hand" must be conducted. The surgeon must verify full passive range of motion (PROM) in all digital joints, the thumb web space, and the wrist. Any soft tissue contractures, particularly first web space adduction contractures, must be aggressively managed preoperatively with serial splinting and therapy; failure to achieve a supple hand preoperatively will doom the tendon transfer to mechanical failure.
Radiographic evaluation is mandatory, particularly when joint stabilization procedures are planned for the first stage. Standard posteroanterior, lateral, and oblique radiographs of the hand and wrist are obtained to assess bone quality, joint congruency, and the presence of any heterotopic ossification. If a CMC arthrodesis is planned, the surgeon must template the exact angles of fusion (45 degrees of palmar abduction and 20 degrees of radial abduction) to ensure that the thumb will be perfectly positioned to meet the index finger during the second-stage key pinch reconstruction. The bone stock of the trapezium and first metacarpal must be evaluated to ensure it can support Kirschner wire or screw fixation, as osteopenia is a ubiquitous finding in the chronic spinal cord injury population.
Patient positioning and intraoperative setup require meticulous attention to detail, given the unique physiological vulnerabilities of the tetraplegic patient. The patient is positioned supine on a well-padded operating table, with all bony prominences meticulously protected to prevent intraoperative pressure ulceration. The operative arm is placed on a radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm, though the surgeon must be acutely aware of the risks of autonomic dysreflexia triggered by tourniquet pain in patients with injuries above T6. Close communication with the anesthesia team is paramount, and deep regional or general anesthesia is typically employed to blunt sympathetic responses.
The arm is prepped and draped in a standard sterile fashion, ensuring exposure from the mid-humerus to the fingertips. The surgeon must ensure that the elbow can be freely flexed and extended intraoperatively, as precise elbow positioning is critical for determining the correct tension of the BR transfer. A sterile marking pen is used to delineate the planned incisions, carefully mapping the course of the superficial radial nerve and the cephalic vein to prevent inadvertent iatrogenic injury during the extensive proximal dissection required for donor muscle mobilization.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of the Zancolli reconstruction is a masterclass in tissue handling, precise tensioning, and rigid skeletal stabilization. The procedure is strictly divided into two distinct operative stages, separated by a minimum of four to six months of intensive rehabilitation.
First Step: The Extension Phase and Thumb Stabilization
The primary objectives of the first stage are to provide active, synchronized extension of the fingers and thumb, and to rigidly stabilize the thumb column to prepare for future pinch reconstruction. Three primary incisions are typically required. A long, curved radial incision is utilized to harvest the brachioradialis and expose the extensor compartments, while additional incisions are made over the thumb CMC or MCP joints for stabilization.
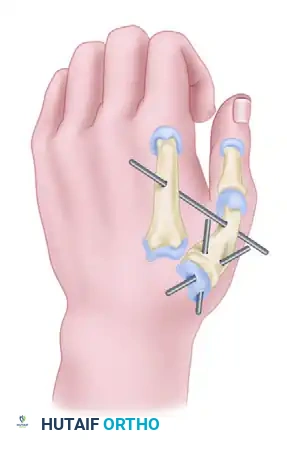
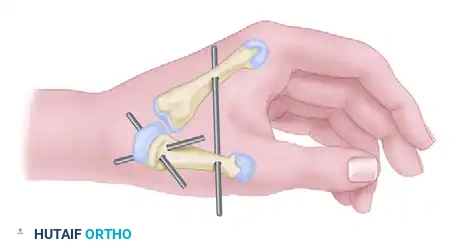
Thumb stabilization is the critical first maneuver. Depending on the patient's specific joint laxity, this is achieved either through CMC arthrodesis or MCP capsuloplasty. If CMC arthrodesis is selected, the joint is approached dorsoradially. The articular cartilage of the trapezium and the base of the first metacarpal is meticulously denuded down to bleeding subchondral bone. The joint is then compressed and fused in a highly specific functional position: 45 degrees of palmar abduction and 20 degrees of radial abduction. Fixation is typically achieved using two crossed Kirschner wires across the CMC joint, with a third wire placed between the first and second metacarpals to rigidly maintain the first web space during the osseous integration phase.

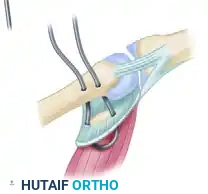
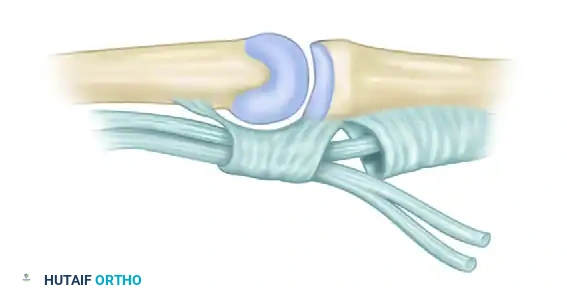
Alternatively, if the MCP joint demonstrates a profound tendency to hyperextend—a ubiquitous finding in the paralyzed thumb that destroys effective pinch—a volar plate capsuloplasty is indicated.
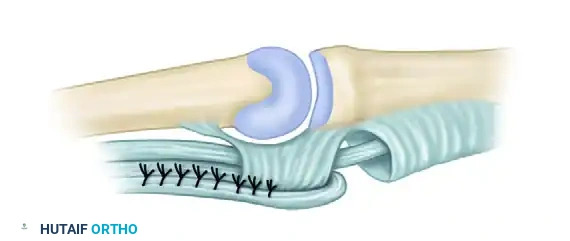
Through a volar incision over the thumb MCP joint, the flexor sheath is retracted, and the volar plate, along with its associated radial sesamoid, is identified. The volar plate is advanced proximally and sutured directly into a bony trough created at the neck of the first metacarpal using robust, non-absorbable sutures or suture anchors. This creates a powerful volar tether that absolutely prevents hyperextension while permitting functional flexion.

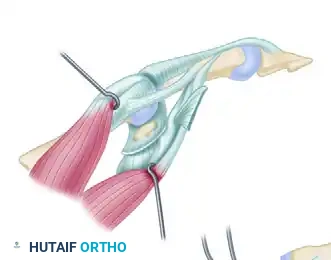
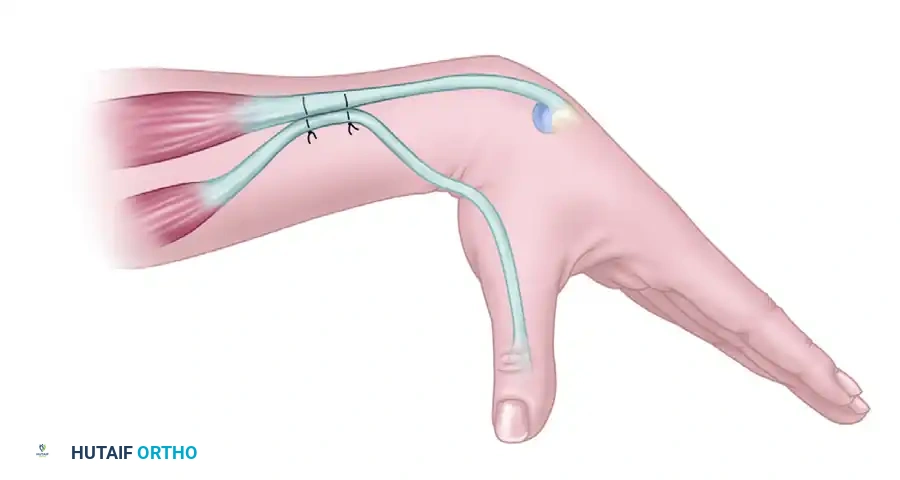
Following thumb stabilization, attention turns to the tendon transfer. The brachioradialis (BR) is identified and mobilized proximally to its fascial origin on the humerus to maximize excursion. The extensor digitorum communis (EDC) tendons and the extensor pollicis longus (EPL) are identified and transected at their musculotendinous junctions. The BR is then transferred to the EDC and EPL using a classic Pulvertaft weave to ensure a biomechanically superior, pull-out resistant repair.
Tensioning the BR transfer is arguably the most critical and unforgiving step of the entire procedure. The elbow must be rigidly maintained at exactly 60 degrees of flexion during tensioning. Slightly more tension is applied to the EDC than to the EPL, anticipating that subsequent elbow extension will naturally reduce the tension on the EDC due to the proximal origin of the BR. The tension is deemed optimal when full passive finger flexion can be obtained with maximal wrist extension and the elbow at 60 degrees of flexion.

If the digital MCP joints exhibit a tendency to claw (hyperextend), the Zancolli lasso procedure is integrated into this first step. Through a transverse palmar incision, the flexor digitorum sublimis (FDS) tendons are divided distally, routed out through the distal margins of the A1 pulleys, looped back, and sutured to themselves. This intrinsic tenodesis prevents MCP hyperextension, ensuring that the extensor force is transmitted to the interphalangeal joints.
Second Step: The Flexion Phase
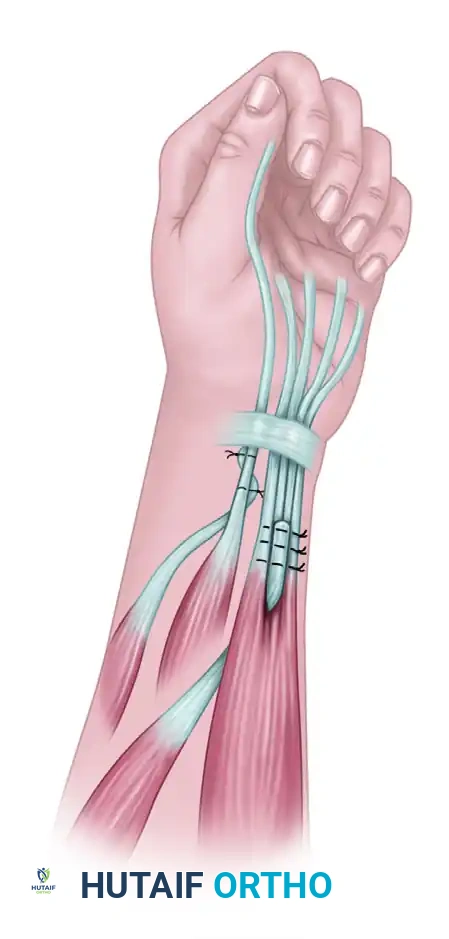
Four to six months later, once active extension is cortically mastered, the second step is performed to restore grasp and key pinch. The extensor carpi radialis longus (ECRL) is harvested, routed volarly through the interosseous membrane or around the radial border of the forearm, and woven into the flexor digitorum profundus (FDP) tendons. Tensioning must recreate the natural cascade of the hand, with slightly more tension applied to the ulnar digits to ensure a powerful, synchronous grip.
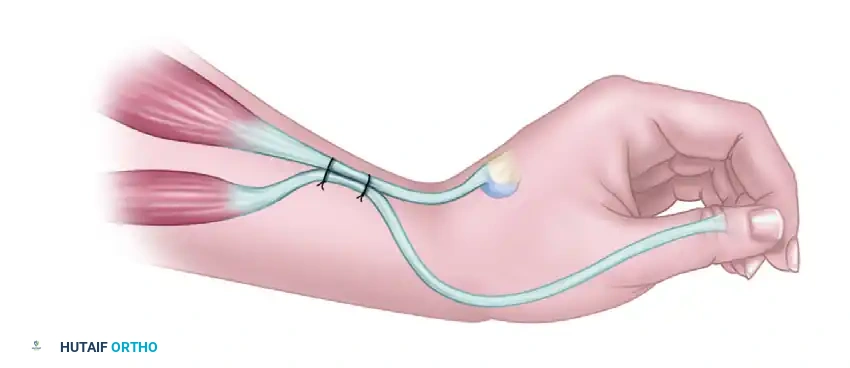
Restoring thumb flexion for key pinch is the final objective. If a supernumerary extensor carpi radialis tertius is present, it is transferred directly to the flexor pollicis longus (FPL). If absent, the FPL is activated by suturing it side-to-side to the active extensor carpi radialis brevis (ECRB). This ingenious tenodesis ensures that thumb flexion occurs automatically with active wrist extension, creating a powerful key pinch.
With the wrist placed in complete passive extension, the FPL tendon is pulled until the thumb firmly rests against the lateral aspect of the index finger. The FPL is sutured to the ECRB at this exact, maximal tension to ensure a rigid pinch mechanism.
Complications, Incidence Rates, and Salvage Management
The Zancolli reconstruction, while highly effective, is fraught with potential complications that can compromise the functional outcome. The surgeon must be intimately familiar with these pitfalls, their incidence rates, and the appropriate salvage maneuvers. The tetraplegic forearm is highly prone to severe scarring, making meticulous tissue handling and hemostasis absolute prerequisites.
Adhesion formation at the tendon transfer site is the most frequent complication, leading to a loss of excursion and subsequent failure of active motion. This is particularly common when the Pulvertaft weaves are placed directly beneath the extensor retinaculum. Over-tensioning of the BR to the EDC is a catastrophic error; if the EDC is excessively tight, the patient will lose the ability to passively flex the fingers, permanently destroying the grasp that is meant to be reconstructed in the second stage. Conversely, under-tensioning results in an extensor lag that prevents the hand from opening sufficiently to grasp large objects.
Failure of thumb stabilization is another significant pitfall. If the CMC fusion fails to unite (non-union), or if the MCP capsulodesis stretches out over time, the thumb will inevitably collapse into hyperextension during key pinch. This biomechanical collapse renders the FPL transfer entirely ineffective, as the force is dissipated at the unstable joint rather than directed into the pinch mechanism.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Revision Strategy |
|---|---|---|---|
| Tendon Adhesions | 15% - 25% | Poor hemostasis; weaving under retinaculum; delayed rehab. | Intensive therapy; surgical tenolysis after 6 months; excision of retinaculum. |
| Over-tensioned BR | 5% - 10% | Tensioning with elbow extended; failure to assess passive flexion intra-op. | Surgical lengthening of the transfer (Z-lengthening); intense prolonged passive stretching. |
| CMC Non-union | 5% - 15% | Poor bone stock; inadequate denuding of cartilage; premature pin removal. | Revision arthrodesis with autologous bone grafting and rigid plate/screw fixation. |
| MCP Capsulodesis Failure | 10% - 20% | Suture pull-out from osteopenic bone; aggressive early mobilization. | Revision capsulodesis with suture anchors; conversion to MCP arthrodesis. |
| Autonomic Dysreflexia | Variable | Tourniquet pain; inadequate anesthesia depth; bladder distension. | Immediate tourniquet let-down; deepen anesthesia; administer rapid-acting antihypertensives. |
Salvage management requires a highly individualized approach. For severe adhesions that do not respond to six months of intensive hand therapy, a surgical tenolysis may be indicated. However, the surgeon must warn the patient that tenolysis in the tetraplegic forearm carries a high risk of recurrent scarring. In cases of irreconcilable over-tensioning, formal surgical lengthening of the tendon weave is required. If a joint stabilization procedure fails, revision to a formal arthrodesis using rigid internal fixation (plates and screws, if bone stock permits) is the most reliable salvage option to restore the stable post necessary for pinch.
Phased Post-Operative Rehabilitation Protocols
The surgical execution of the Zancolli reconstruction represents only half of the therapeutic equation; the ultimate success of the procedure is entirely dependent upon a rigorous, highly specialized, and phased postoperative rehabilitation protocol. The rehabilitation must be guided by a specialized hand therapist experienced in spinal cord injury, as the principles differ significantly from standard tendon transfer protocols in neurologically intact patients.
Phase 1 encompasses the initial period of strict immobilization designed to protect the tendon transfers and joint fusions during the critical early phases of biological healing. Following the first step (Extension Phase), the hand and elbow are immobilized in a custom-fabricated, long-arm orthosis for exactly four weeks. The wrist is positioned in 45 degrees of extension to relieve tension on the ECRB, the MCP joints are held in 20 degrees of flexion to protect the Zancolli lasso, and the interphalangeal joints are maintained in full extension. The elbow must be included in the splint to protect the proximal BR dissection. Following the second step (Flexion Phase), the immobilization strategy shifts: the wrist is held in neutral, the thumb is positioned in the key pinch posture resting between the index and middle fingers, and the fingers are gently flexed to protect the volar transfers.
Phase 2 initiates early active motion and cortical remapping, typically commencing at the four-week postoperative mark. The long-arm splint is transitioned to a removable orthosis. For the extension phase, the patient is taught the counter-intuitive process of initiating active MCP extension by utilizing elbow flexion (firing the BR). Biofeedback modalities, including surface electromyography (sEMG) and mirror visual feedback, are invaluable tools during this phase to help the patient isolate the transferred muscle and overcome synergistic mass movements. Passive finger flexion exercises are absolutely mandatory during this phase to prevent extension contractures and maintain the suppleness required for the upcoming second stage.
Phase 3 focuses on strengthening and functional integration, beginning at eight to twelve weeks postoperatively. The patient begins progressive resistance exercises, carefully calibrated to avoid overloading the tendon weaves. For the flexion phase, rehabilitation focuses on synergistic muscle re-education, training the patient to actively extend the wrist to drive the tenodesis effect and flex the digits. Occupational therapy becomes paramount, focusing on integrating the newly acquired grasp and release mechanisms into activities of daily living (ADLs), such as feeding, grooming, and catheterization. The transfers must be protected from heavy, sudden resistance for a minimum of three to four months to ensure complete remodeling of the tendon weave.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical reconstruction for the tetraplegic upper extremity is chronicled in several landmark publications that form the evidence-based foundation of the Zancolli procedure. Eduardo Zancolli’s original treatises on the biomechanics of the paralyzed hand, published in the mid-20th century, remain the definitive texts on the subject. His seminal observation that simultaneous reconstruction of antagonist muscle groups in upper motor neuron lesions leads to catastrophic cortical confusion fundamentally altered the trajectory of tetraplegia surgery, establishing the absolute necessity of the staged approach.
Erik Moberg further refined the field by emphasizing the critical importance of sensory preservation and the concept of the "supple
