Carpal Fractures & Dislocations: Don't Miss These Crucial Signs
Key Takeaway
This article provides essential research regarding Carpal Fractures & Dislocations: Don't Miss These Crucial Signs. Carpal fractures and dislocations involve breaks or misalignments of the eight carpal bones in the wrist, often misdiagnosed as simple sprains. These injuries affect the scaphoid, lunate, triquetrum, and other carpal bones, frequently disrupting key ligaments like the scapholunate. Such conditions can lead to significant instability, with perilunate dislocations being a common type of wrist dislocation.
As orthopedic surgeons, residents, and medical students, we are acutely aware that seemingly benign wrist injuries can harbor devastating, often elusive, carpal pathologies. Carpal fractures and dislocations, frequently masquerading as simple sprains, represent a critical diagnostic challenge. A missed or delayed diagnosis carries profound implications, often leading to chronic pain, instability, avascular necrosis, post-traumatic arthritis, and functional impairment, necessitating complex reconstructive procedures or salvage arthrodesis. Our objective is to delineate the critical signs, diagnostic pathways, and surgical principles essential for effective management of these nuanced injuries.
Introduction and Epidemiology
Carpal fractures and dislocations constitute a significant portion of upper extremity trauma, with a prevalence that often belies their potential for severe long-term morbidity. Despite advances in imaging and surgical techniques, these injuries remain a diagnostic pitfall, frequently overlooked in initial assessments. The intricate anatomy and complex kinematics of the wrist render accurate diagnosis and timely intervention paramount. The cumulative incidence of carpal fractures, excluding the distal radius, is approximately 10-15% of all hand and wrist fractures, with scaphoid fractures alone accounting for 60-70% of all carpal fractures. Perilunate dislocations, while less common, represent the second most frequent carpal injury pattern requiring surgical intervention and are often associated with high-energy trauma. The misdiagnosis rate for carpal injuries, particularly scaphoid fractures and perilunate dislocations, can be as high as 25-50% in initial presentations, highlighting the need for a high index of suspicion and meticulous diagnostic protocols. This comprehensive review aims to serve as a high-yield reference for navigating the complexities of carpal trauma.
Surgical Anatomy and Biomechanics
The carpus is a complex articulation of eight distinct carpal bones, meticulously arranged into two rows, functioning as an intercalated segment between the distal forearm and the metacarpals. This architectural design facilitates a remarkable range of motion while simultaneously providing stability for force transmission.
Fractures and dislocations involving the carpus can be easily misdiagnosed as wrist sprains due to the often subtle initial clinical presentation and radiographic findings. A thorough understanding of carpal anatomy and biomechanics is fundamental to avoid these diagnostic pitfalls.
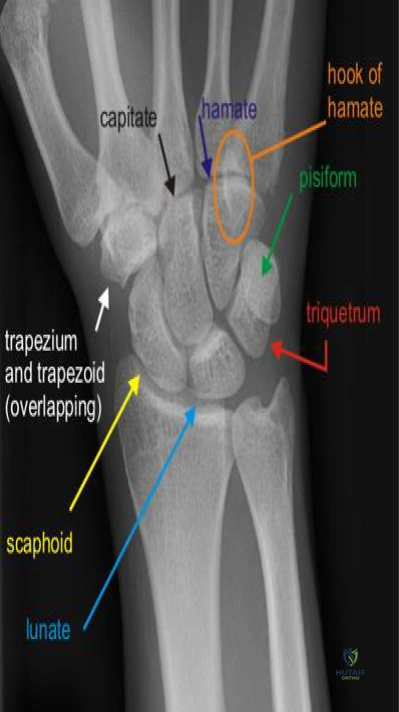
Carpal Bone Architecture
The carpus comprises eight bones grouped into two distinct rows:
- Distal Carpal Row: This row consists of the trapezium, trapezoid, capitate, and hamate. These bones are characterized by strong ligamentous connections both within the row and with the bases of the metacarpals (MCs), forming a rigid transverse arch. This structural rigidity allows the distal carpal row to function largely as a single unit, providing a stable base for the metacarpals.
- Trapezium: Articulates primarily with the base of the first metacarpal, critical for thumb mobility.
- Trapezoid: Articulates with the base of the second metacarpal.
- Capitate: The largest carpal bone, it forms the central pillar of the carpus and articulates with the third metacarpal. Its head is the primary axis of rotation for wrist motion.
- Hamate: Articulates with the bases of the fourth and fifth metacarpals, featuring a prominent hook (hook of hamate) that serves as an attachment point for various ligaments and intrinsic hand muscles.

* Proximal Carpal Row: This row includes the scaphoid, lunate, and triquetrum. Unlike the distal row, the proximal carpal row lacks direct tendinous attachments and is considered an intercalated segment. It articulates proximally with the radius and ulna, and distally with the distal carpal row.
* Scaphoid: Boat-shaped, it bridges both carpal rows, making it crucial for carpal stability and kinematics. Its precarious blood supply (retrograde from distal pole) renders it susceptible to avascular necrosis (AVN) following fracture, particularly in the proximal pole.
* Lunate: Moon-shaped, centrally positioned in the proximal row, articulating with the radius proximally and the capitate distally. Its central location makes it a fulcrum for wrist motion, but also vulnerable to instability and AVN (Kienböck's disease).
* Triquetrum: Pyramid-shaped, articulating with the lunate, hamate, and distally with the ulna via the triangular fibrocartilage complex (TFCC).
* Pisiform: A sesamoid bone embedded within the flexor carpi ulnaris (FCU) tendon, articulating solely with the palmar surface of the triquetrum. It enhances the mechanical advantage of the FCU.
The carpus is made up of 8 bones grouped into 2 rows.
Carpal Kinematics and Ligamentous Structures
The primary axis of wrist rotation passes through the head of the capitate. The carpus does not move as a simple hinge; rather, complex coupled motions occur:
* In radial deviation, the scaphoid flexes, driving the entire proximal carpal row into flexion.
* In ulnar deviation, the scaphoid extends, causing the proximal row to extend.
These motions are governed by a complex network of intrinsic and extrinsic ligaments.
* Ligaments:
* Transverse Carpal Ligament (Flexor Retinaculum): Extends from the scaphoid tubercle and trapezium to the hook of the hamate and pisiform. It forms the roof of the carpal tunnel, containing the median nerve and nine flexor tendons.
* Extrinsic Ligaments: Connect the radius and ulna to the carpus, and the carpus to the metacarpals. Volar (palmar) ligaments are generally thicker and stronger than dorsal ligaments, providing the primary static stabilizers of the wrist. Key volar ligaments include the radioscaphocapitate, radiolunotriquetral, and ulnocarpal ligaments. Dorsal ligaments, such as the dorsal radiotriquetral and dorsal intercarpal ligaments, also contribute significantly to stability.
* Intrinsic Ligaments: Connect carpal bones to each other within the rows. These are critical for maintaining carpal alignment and preventing dissociation.
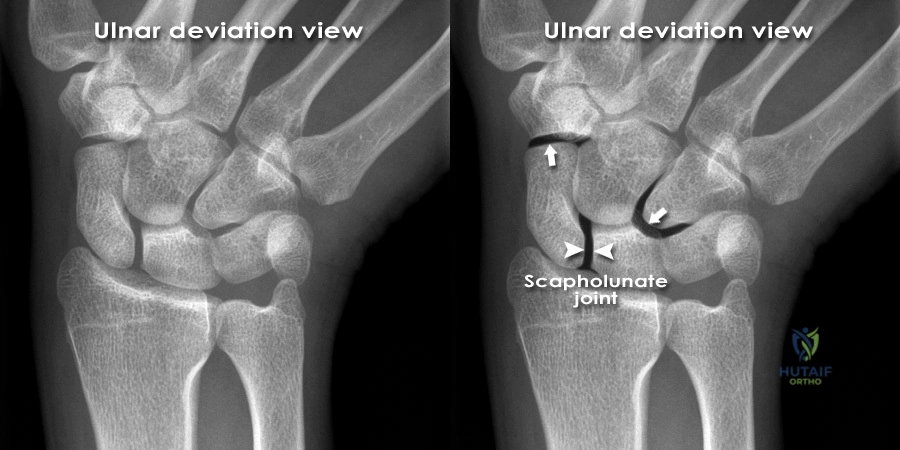
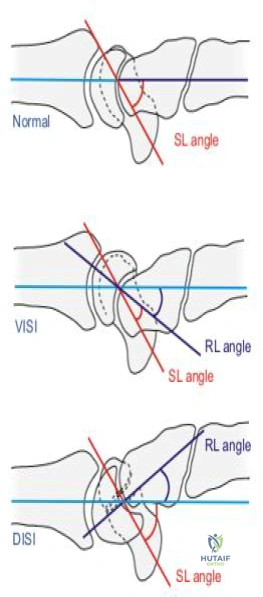
* Scapholunate Interosseous Ligament (SLIL): The most crucial intrinsic ligament, connecting the scaphoid and lunate. Injury leads to scapholunate dissociation (SLD), a common cause of dorsal intercalated segment instability (DISI).
* Lunotriquetral Interosseous Ligament (LTIL): Connects the lunate and triquetrum. Injury leads to lunotriquetral dissociation (LTD) and often palmar intercalated segment instability (PISI).
* Other interosseous ligaments: Connect bones within the distal carpal row, providing strong transverse stability.
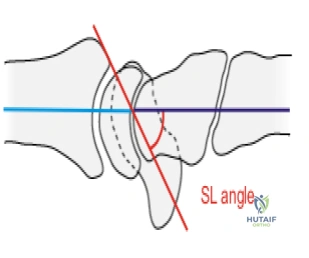
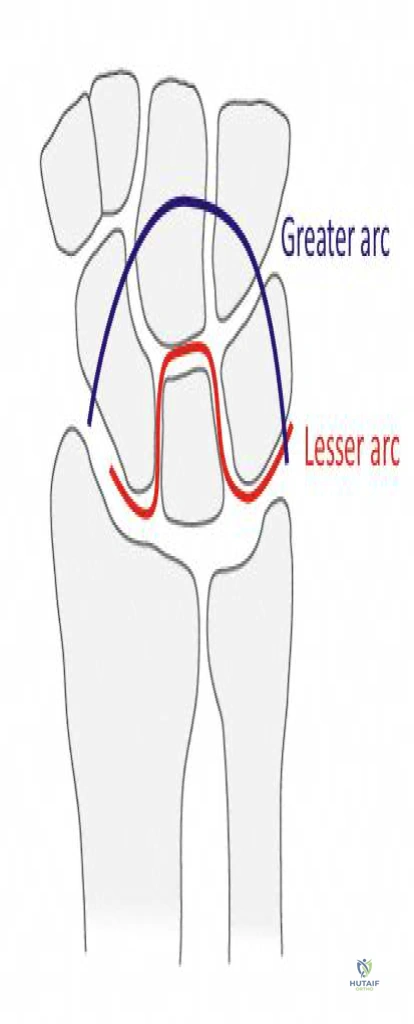
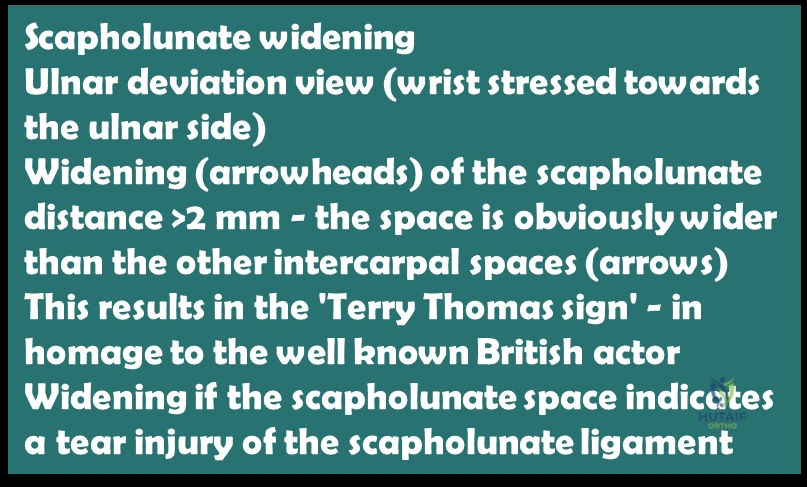
The interplay of these bones and ligaments creates a kinematic chain. Injury to a single component, especially key ligaments or bones like the scaphoid or lunate, can disrupt this chain, leading to complex instability patterns. For example, a fall on an outstretched hand with the wrist hyperextended and ulnarly deviated is a common mechanism for perilunate dislocations, representing a sequential failure of these critical ligamentous restraints. Early recognition of subtle radiographic signs, such as widening of the scapholunate gap (Terry Thomas sign) or changes in carpal arcs (Gilula's lines), is imperative.
Indications and Contraindications
The decision for operative versus non-operative management of carpal fractures and dislocations is predicated on a meticulous assessment of injury characteristics, patient factors, and functional demands. The primary goals are to restore anatomical alignment, achieve stable fixation, preserve carpal kinematics, and prevent long-term sequelae such as nonunion, avascular necrosis, and post-traumatic arthritis.
General Considerations
- Injury Severity: Displaced fractures, unstable fracture patterns, and dislocations typically warrant surgical intervention.
- Vascularity: Bones with precarious blood supply, notably the scaphoid, demand prompt attention to mitigate avascular necrosis.
- Associated Injuries: Concurrent ligamentous injuries or other fractures often mandate operative stabilization to optimize overall wrist function.
- Patient Factors: Age, activity level, hand dominance, and comorbidities influence management decisions.
- Time to Presentation: Delayed presentations of unstable injuries or nonunions generally necessitate surgical reconstruction.
Operative Indications
Specific indications for surgical intervention include:
* Scaphoid Fractures:
* Displaced fractures (>1mm) or angulation (>10-15 degrees)
* Proximal pole fractures due to high risk of AVN
* Scaphoid waist fractures with instability
* Fracture-dislocations
* Established nonunions or symptomatic delayed unions
* Perilunate Dislocations and Lunate Dislocations:
* All acute perilunate and lunate dislocations require urgent closed or open reduction and stabilization due to high risk of median nerve compression, carpal instability, and AVN of the lunate.
* Ligamentous Instabilities:
* Acute, reducible scapholunate dissociation (SLD) or lunotriquetral dissociation (LTD) with carpal instability (e.g., dynamic or static DISI/PISI).
* Chronic, symptomatic carpal instabilities not amenable to conservative care.
* Other Carpal Fractures:
* Displaced lunate fractures
* Displaced triquetral body fractures
* Displaced trapezium fractures (e.g., Bennett-type fractures of the thumb base)
* Displaced hamate hook fractures (due to risk of flexor tendon rupture or ulnar nerve irritation)
* Multiple carpal bone fractures
* Irreducible Fractures/Dislocations: Failure of closed reduction.
* Open Fractures/Dislocations: Require urgent debridement and stabilization.
Non-Operative Indications
Non-operative management is typically reserved for stable, minimally displaced injuries, often with careful monitoring.
* Scaphoid Fractures:
* Minimally displaced, stable scaphoid tuberosity fractures.
* Undisplaced scaphoid waist fractures without evidence of instability (though many surgeons still advocate for early internal fixation due to high nonunion rates and prolonged immobilization).
* Other Carpal Fractures:
* Undisplaced dorsal triquetral chip fractures.
* Stable, minimally displaced fractures of the trapezoid or capitate without associated instability.
* Sprains:
* Mild carpal ligament sprains without evidence of carpal instability on clinical or radiographic examination.
Contraindications
Absolute contraindications to surgery are rare and typically relate to the patient's overall medical status rendering them unfit for anesthesia. Relative contraindications may include:
* Severe comorbidities precluding safe anesthesia or prolonged rehabilitation.
* Active infection in the surgical field.
* Extensive soft tissue compromise precluding wound closure.
* Patient refusal or non-compliance with post-operative protocols.
* Extremely comminuted fractures where stable fixation is unachievable, potentially leading to consideration of primary arthrodesis or carpectomy in select cases.
Summary of Operative vs Non-Operative Indications
| Injury Type | Operative Indications | Non-Operative Indications |
|---|---|---|
| Scaphoid Fracture | Displaced (>1mm), angulated (>10-15°), proximal pole, nonunion, instability | Undisplaced distal tuberosity, select stable waist fractures (controversial) |
| Perilunate/Lunate Dislocation | All acute dislocations, irreducible by closed means | None, all require prompt reduction (often surgical) |
| Scapholunate Dissociation (SLD) | Acute, reducible, symptomatic, dynamic/static instability | Chronic, asymptomatic (observe), degenerative (salvage) |
| Lunotriquetral Dissociation (LTD) | Acute, reducible, symptomatic, dynamic/static instability | Chronic, asymptomatic (observe) |
| Hamate Hook Fracture | Displaced, symptomatic nonunion, ulnar nerve/tendon irritation | Undisplaced, asymptomatic (rare) |
| Other Carpal Fractures (Triquetrum, Lunate, Trapezium, Capitate) | Displaced, unstable, intra-articular step-off | Undisplaced, stable, non-articular (e.g., dorsal triquetral chip) |
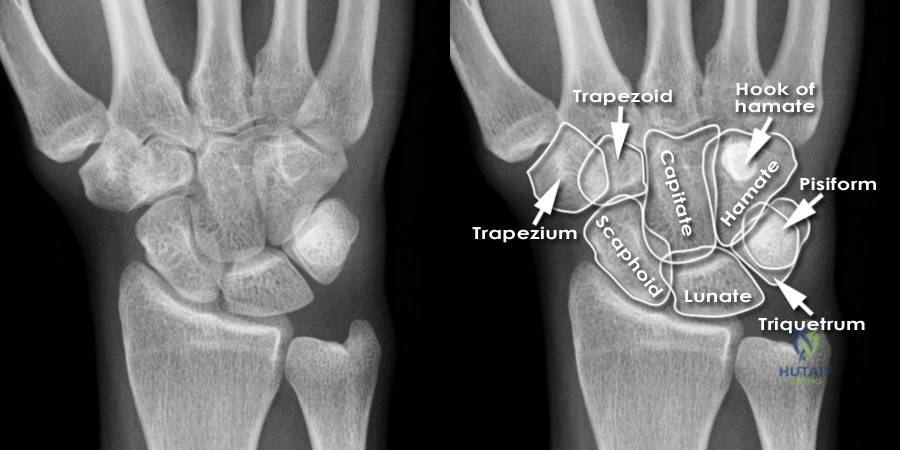
Note the image of the carpal bones.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is indispensable for successful outcomes in carpal fracture and dislocation surgery, given the intricate anatomy and potential for complications.
Diagnostic Imaging
- Standard Radiographs: A minimum of four views—posteroanterior (PA), lateral, oblique, and scaphoid views—are essential.
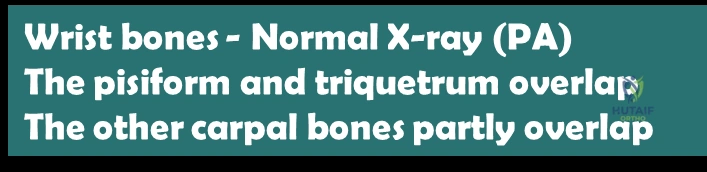
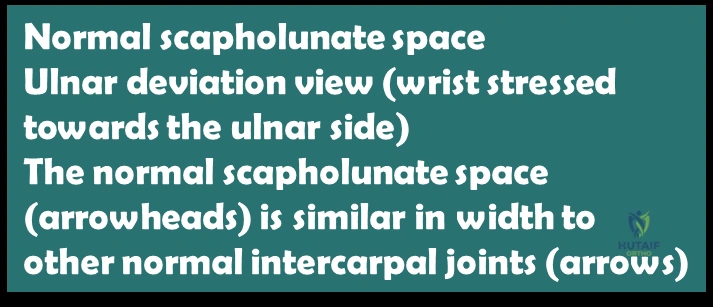
- PA View: Assess carpal alignment (Gilula's arcs), scapholunate and lunotriquetral intervals, and identify fractures.
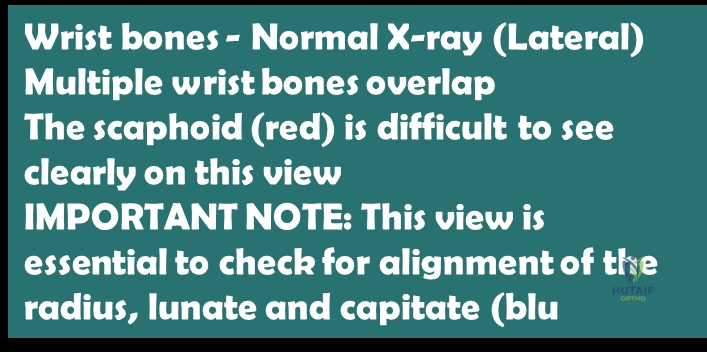
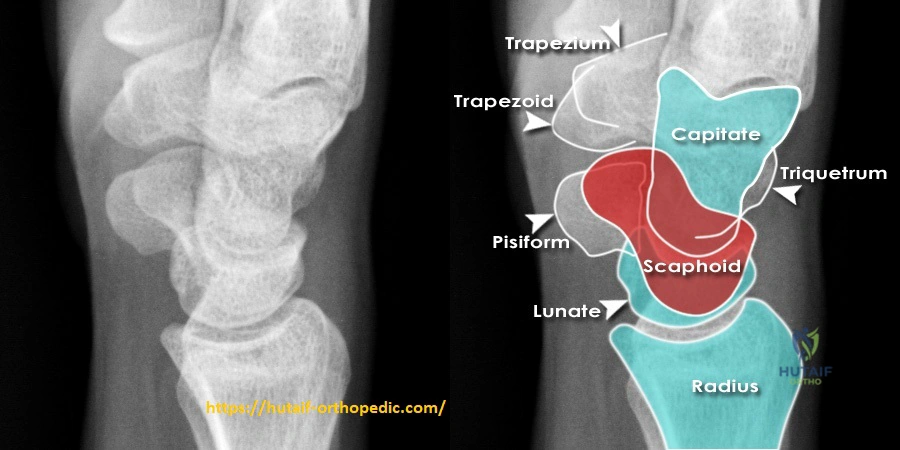
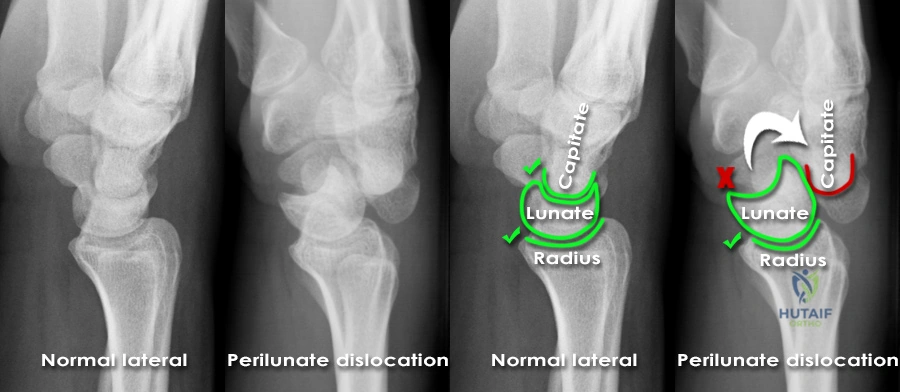
- Lateral View: Crucial for evaluating sagittal plane alignment, particularly for lunate posture (flexion in DISI, extension in PISI) and carpal malalignment in perilunate injuries (e.g., capitate dorsal to lunate).
- Oblique Views: Aid in visualizing specific carpal bones often obscured on standard views.
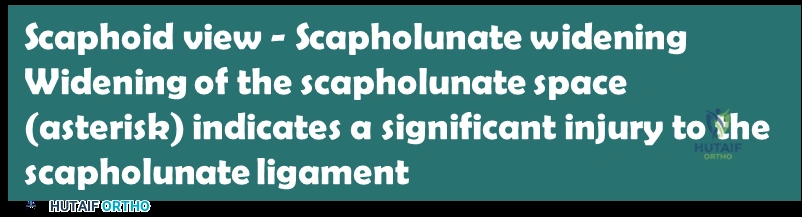
- Scaphoid Views: A specific series (PA with ulnar deviation, 30° pronated oblique, 30° supinated oblique, true lateral) helps unmask subtle scaphoid fractures.

- Computed Tomography (CT) Scan: The gold standard for assessing fracture morphology, comminution, displacement, articular involvement, and precise fragment orientation. Essential for surgical planning in scaphoid fractures, perilunate dislocations, and complex carpal injuries.
- Magnetic Resonance Imaging (MRI): Highly valuable for detecting occult fractures, assessing ligamentous integrity (e.g., SLIL, LTIL tears), and evaluating vascularity (e.g., scaphoid AVN, Kienböck's disease stages).
- Fluoroscopy: Used intraoperatively for real-time assessment of reduction and fixation.
Surgical Approach Selection
The choice of surgical approach depends on the specific injury, location, and surgeon preference.
* Volar Approach: Often preferred for scaphoid waist and distal pole fractures, providing direct access for screw fixation and vascularized bone grafting. Also used for acute perilunate dislocations for direct reduction and ligament repair.
* Dorsal Approach: Indicated for proximal pole scaphoid fractures, dorsal ganglion excisions, and certain carpal fusions. Allows good visualization of dorsal carpal ligaments and dorsal carpal instability.
* Combined Dorsal and Volar Approaches: May be necessary for complex perilunate dislocations or highly unstable carpal injuries requiring extensive reduction and ligament repair.
* Minimally Invasive Techniques: Arthroscopy-assisted reduction and fixation for select fractures or ligamentous repairs.
Implant Selection
- Screws: Cannulated Herbert-type screws are common for scaphoid fractures, providing compression and stability. Miniature headless compression screws are versatile.
- K-wires: Used for temporary fixation, adjunctive fixation, or primary fixation in certain fractures (e.g., triquetral, hamate hook) and ligament repairs.
- Plates: Mini-fragment plates may be used for complex carpal fractures or reconstructive procedures.
- Bone Grafts: Autogenous (e.g., distal radius, iliac crest) or allogenous bone grafts are often required for scaphoid nonunions or significant bone loss. Vascularized bone grafts (e.g., 1,2 intercompartmental supraretinacular artery (1,2-ICSRA) flap) are indicated for scaphoid nonunions with proximal pole AVN.
Patient Positioning
- Supine Position: Standard for most wrist surgeries.
- Arm Table: A specialized hand table is used to support the arm, providing a stable platform and allowing for unimpeded access to the wrist.
- Tourniquet: A pneumatic tourniquet on the upper arm is routinely used to provide a bloodless field, which is critical for visualizing small carpal structures and ligaments.
- Image Intensifier: Essential for intraoperative radiographic control of reduction and fixation. It should be positioned to allow for PA, lateral, and oblique views without repositioning the patient.
- Hand Prep and Drape: The entire upper extremity, from axilla to fingertips, should be prepped and draped free to allow for full range of motion of the wrist and fingers during the procedure, facilitating reduction maneuvers. Finger traps with traction may be applied for certain reduction techniques.
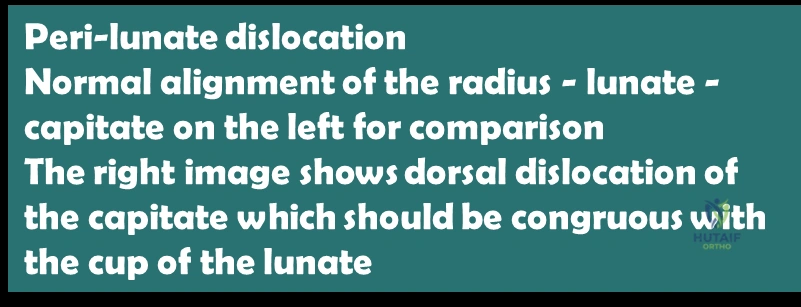
Illustration of hand and wrist anatomy.
Detailed Surgical Approach and Technique
Surgical management of carpal fractures and dislocations demands precision, an understanding of complex regional anatomy, and meticulous technique. The following outlines general principles and specific considerations for common carpal pathologies.
General Principles of Carpal Surgery
- Adequate Exposure: Obtain sufficient exposure to visualize the fracture/dislocation and surrounding ligaments while minimizing soft tissue stripping.
- Gentle Tissue Handling: Protect neurovascular structures and maintain vascularity of bone fragments.
- Anatomic Reduction: Achieve precise anatomical reduction of fracture fragments and carpal alignment. Fluoroscopy is critical.
- Stable Fixation: Provide rigid internal fixation to allow for early mobilization and prevent loss of reduction.
- Ligament Repair/Reconstruction: Address associated ligamentous injuries where appropriate to restore carpal stability.
Scaphoid Fracture Fixation (Volar Approach for Waist Fractures)
Incision and Dissection
- Incision: A curvilinear incision is made on the volar aspect of the wrist, extending from the distal forearm radial to the flexor carpi radialis (FCR) tendon, across the wrist crease, and distally towards the base of the thenar eminence.
- Superficial Dissection: Incise the skin and subcutaneous tissue. Carefully identify and protect branches of the superficial radial nerve and the palmar cutaneous branch of the median nerve.
- Deep Dissection:
- The FCR tendon sheath is opened longitudinally. The FCR tendon is retracted ulnarly.
- The radial artery lies just radial to the FCR sheath. It is identified and carefully protected, often retracted radially.
- Deep to the FCR tendon, the pronator quadratus muscle is encountered. This muscle is incised transversely or longitudinally and elevated from the radius, exposing the volar aspect of the distal radius and the radioscaphocapitate ligament.
- The radioscaphocapitate ligament and anterior capsule are incised in line with the planned approach to the scaphoid.
Fracture Exposure and Reduction
- Exposure: The volar aspect of the scaphoid is exposed, typically revealing the waist fracture.
- Reduction: Under fluoroscopic guidance, the fracture fragments are anatomically reduced using gentle manipulation, joy-sticking with K-wires inserted into the fragments, or a mini-lambar instrument. Compression of the fragments can be achieved. Ensure correct alignment in all planes.
Fixation
- Guidewire Placement: A guidewire for a headless compression screw (e.g., Herbert or Acutrak) is carefully inserted from the distal pole across the fracture site into the proximal pole. Correct trajectory is critical; it should be centrally placed in both the PA and lateral views to maximize compression and prevent articular violation.
- Measurement and Drilling: Measure the required screw length. Cannulated drill bits are used to prepare the bone tunnel.
- Screw Insertion: The headless compression screw is inserted over the guidewire. It should be fully buried beneath the articular surface at both ends. Compression across the fracture site is confirmed fluoroscopically.
- Closure: The capsule and pronator quadratus are repaired. The FCR sheath is closed. Skin and subcutaneous tissues are closed in layers.
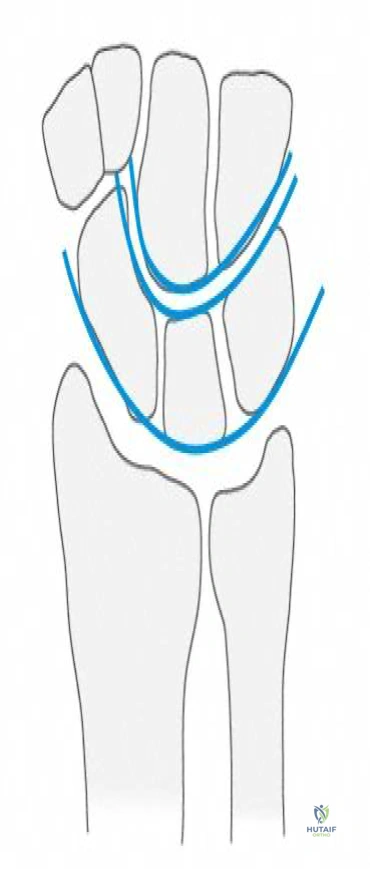
Illustration of scaphoid anatomy.
Perilunate Dislocation Reduction and Stabilization (Dorsal Approach)
Acute perilunate dislocations require prompt reduction and stabilization to prevent median nerve compression and long-term instability. Open reduction is often necessary, especially if closed reduction fails or if soft tissue interposition is suspected.
Incision and Dissection
- Incision: A longitudinal dorsal midline incision is made over the wrist, extending from the distal forearm across the wrist joint.
- Superficial Dissection: Identify and protect dorsal sensory nerves, particularly the dorsal cutaneous branch of the ulnar nerve and radial nerve branches.
- Deep Dissection: The extensor retinaculum is incised longitudinally, typically between the third (extensor pollicis longus, EPL) and fourth (extensor digitorum communis, EDC) compartments. The extensor tendons are retracted.
- Capsule Incision: A dorsal capsulotomy is performed, often T-shaped or U-shaped, to expose the dorsal carpus. The dorsal radiocarpal and dorsal intercarpal ligaments are carefully inspected for injury.
Reduction and Assessment
- Reduction Maneuver: If closed reduction was unsuccessful, open reduction is performed. Often, traction, wrist flexion, and direct manipulation of the capitate (which is typically dorsally displaced) are used to "seat" it back into the lunate concavity. A Freer elevator can assist.
- Lunate Assessment: Confirm the lunate remains correctly aligned with the radius (not dislocated into the carpal tunnel).
- Ligament Inspection: Critically inspect the scapholunate interosseous ligament (SLIL) and lunotriquetral interosseous ligament (LTIL) for tears. The radioscaphocapitate ligament and the dorsal radiolunotriquetral ligament (dorsal intrinsic) are often torn.
Fixation and Ligament Repair
- K-wire Stabilization: Once anatomic reduction of the carpus is achieved, temporary K-wires are placed to maintain alignment:
- Scapholunate K-wires: Typically, two K-wires across the scapholunate joint (e.g., scaphoid to lunate, scaphoid to capitate, lunate to radius) to maintain SL interval and lunate position.
- Lunotriquetral K-wire: One K-wire may be placed from the triquetrum to the lunate if LTIL injury is suspected.
- Radioscaphoid/Radiolunate K-wires: Wires from the scaphoid to the radius and lunate to the radius may be used for additional stability, particularly if initial reduction is tenuous.
- Ligament Repair:
- SLIL Repair: Direct repair of the scapholunate interosseous ligament (SLIL) is performed with non-absorbable sutures (e.g., 2-0 FiberWire) if the tissue quality allows. Suture anchors may be used into the scaphoid or lunate if avulsed from bone.
- Dorsal Capsulodesis: Reinforce the repair with a dorsal capsulodesis, advancing the dorsal radiotriquetral ligament or a portion of the dorsal capsule to reinforce the scapholunate interval. This acts as a tenodesis, restricting scaphoid flexion.
- LTIL Repair: Direct repair of the LTIL if torn.
- Closure: The capsule is repaired with strong sutures. The extensor retinaculum is repaired or left open if swelling is anticipated. Skin and subcutaneous tissues are closed in layers.

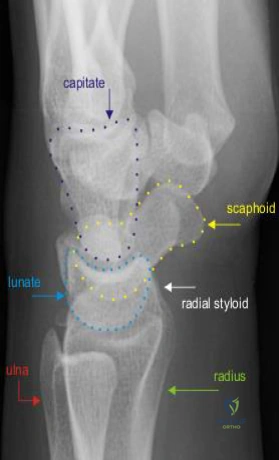
These images illustrate various aspects of wrist anatomy and surgical approaches, often used in documentation.
Other Carpal Fracture Fixation (Brief)
- Hamate Hook Fractures: Usually excised if nonunion is painful or causing ulnar nerve/flexor tendon irritation. Small screws can be used for fixation in acute, displaced fractures.
- Triquetral Fractures: Dorsal avulsion fractures are often treated non-operatively. Displaced body fractures may require open reduction and K-wire or screw fixation.
- Lunate Fractures: Rare, but displaced intra-articular fractures require meticulous open reduction and K-wire or small screw fixation.
Complications and Management
Despite optimal surgical technique, carpal fractures and dislocations are associated with a notable incidence of complications, often secondary to the challenging anatomy, precarious blood supply, and high-energy trauma mechanisms. Proactive recognition and appropriate management are crucial for salvage and functional restoration.
Common Complications
| Complication | Incidence | Management Strategy |
|---|---|---|
| Scaphoid Nonunion | 5-15% (up to 50% for proximal pole/displaced) | Symptomatic: Bone grafting (non-vascularized, vascularized), internal fixation (screws), often with revision. Consider partial wrist fusion (e.g., four-corner fusion) or scaphoidectomy for nonunions with advanced carpal collapse (SNAC wrist). Asymptomatic: Observe, monitor for SNAC progression. |
| Avascular Necrosis (AVN) | High for proximal pole scaphoid, lunate | Scaphoid: Vascularized bone graft (e.g., 1,2-ICSRA flap) in early stages. For advanced collapse (SNAC), salvage procedures (fusion, scaphoidectomy). Lunate (Kienböck's): Radial shortening, capitate lengthening, revascularization procedures, proximal row carpectomy, or fusion. |
| Post-Traumatic Arthritis (PTA) | Common, especially after instability/nonunion | Conservative management initially (NSAIDs, injections, bracing). Surgical options: partial wrist fusion (e.g., four-corner fusion, radioscapholunate fusion), proximal row carpectomy (PRC), total wrist arthrodesis, wrist arthroplasty (less common). |
| Carpal Instability (Residual) | Significant risk post-dislocation/ligament injury | Symptomatic: Ligament reconstruction (e.g., SLIL reconstruction, dorsal capsulodesis), salvage procedures (fusion, PRC). Asymptomatic/Mild: Activity modification, bracing. |
| Malunion | Variable | Symptomatic: Corrective osteotomy (rare), salvage procedures (e.g., fusion, PRC) if functional impairment and pain are significant. |
| Infection | <1% (acute surgery) | IV antibiotics (culture-directed), surgical debridement, implant removal if necessary. |
| Nerve Impingement/Injury | Median nerve (carpal tunnel syndrome post-dislocation) | Acute: Urgent reduction. If symptoms persist, carpal tunnel release. Chronic: Carpal tunnel release. Direct nerve repair/grafting if transected (rare). |
| Hardware-Related Complications | Screw prominence, K-wire migration, breakage | Removal of symptomatic hardware. Revision fixation if stability is compromised. |
| Stiffness/Loss of Motion | Common after prolonged immobilization or severe trauma | Intensive hand therapy, dynamic splinting, consider tenolysis/arthrolysis in severe cases after bony healing. |
| Complex Regional Pain Syndrome (CRPS) | 2-5% | Multidisciplinary approach: physical therapy, pain management (neuropathic medications, nerve blocks), psychological support. Early diagnosis and aggressive treatment are key. |
Management Principles
- Early Recognition: High index of suspicion for developing complications based on clinical symptoms (persistent pain, swelling, altered sensation) and radiographic findings.
- Conservative Measures: Prioritize non-operative treatments for mild or early-stage complications (e.g., rehabilitation for stiffness, NSAIDs for mild arthritis).
- Surgical Intervention: Employ surgical strategies when conservative measures fail, when complications are progressive, or when functional impairment is significant. These can range from revision fixation, bone grafting, ligament reconstruction, to partial or total wrist fusions, or proximal row carpectomy.
- Multidisciplinary Approach: Involve hand therapists, pain management specialists, and neurologists, especially for conditions like CRPS or chronic nerve issues.
- Patient Education: Thoroughly counsel patients on the potential for complications and the realistic expectations for recovery and functional outcomes.
Post Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical procedure itself in optimizing outcomes following carpal fracture and dislocation repair. Protocols must be tailored to the specific injury, surgical technique, and individual patient factors, balancing the need for protection and early motion.
General Principles
- Protection of Repair: The primary goal in the early phase is to protect the surgical repair and allow for initial soft tissue and bone healing.
- Controlled Motion: Gradually introduce controlled active and passive range of motion to prevent stiffness and promote articular cartilage health, without compromising fixation.
- Strength Restoration: Progress to strengthening exercises once adequate healing and pain control are achieved.
- Functional Return: Facilitate a return to activities of daily living (ADLs), occupational tasks, and sport-specific activities.
Phased Rehabilitation Approach
Phase I: Immobilization and Early Protection (0-6 weeks post-op)
- Goals: Protect surgical repair, minimize pain and swelling, maintain uninvolved joint motion.
- Immobilization:
- Scaphoid Fractures (ORIF): Often immobilized in a thumb spica splint or cast for 6-12 weeks, depending on fracture stability, healing progression, and bone graft use. Some surgeons advocate for early gentle protected range of motion (ROM) in very stable fixation.
- Perilunate Dislocations (ORIF/Ligament Repair): Wrist immobilized in a sugar tong or dorsal blocking splint for 4-6 weeks with K-wires in situ. Forearm neutral, wrist in slight extension.
- Therapeutic Interventions:
- Elevation, ice, compression to manage swelling.
- Active range of motion (AROM) for elbow, forearm pronation/supination, and digits (MPs, PIPs, DIPs) to prevent stiffness.
- Pain management.
- Patient education on precautions and signs of complications.
- K-wire Removal: K-wires are typically removed at 6-8 weeks for perilunate injuries, sometimes later for complex instabilities. Scaphoid K-wires are usually removed when union is radiographically confirmed, if K-wires were used for primary fixation.
Phase II: Controlled Motion and Gradual Loading (6-12 weeks post-op)
- Goals: Restore full, pain-free wrist ROM, begin gentle strengthening.
- Transition: Once adequate bony or ligamentous healing is confirmed (e.g., by radiographs/CT for scaphoid union), and K-wires are removed (if present).
- Therapeutic Interventions:
- Wrist AROM/Passive ROM (PROM): Progressively increase wrist flexion, extension, radial and ulnar deviation. Gentle joint mobilizations by therapist.
- Scar Management: Massage, silicone sheeting, desensitization.
- Gentle Strengthening: Isometrics, then light resistance exercises for wrist flexors, extensors, and grip. Focus on endurance.
- Proprioceptive Exercises: Early balance and coordination drills.
- Custom Orthoses: May be used for protection during activities or to address specific motion deficits.
Phase III: Progressive Strengthening and Functional Return (12+ weeks post-op)
- Goals: Maximize strength, power, and endurance; return to full activity.
- Progression: Building upon established ROM and basic strength.
- Therapeutic Interventions:
- Advanced Strengthening: Progressive resistance exercises using weights, resistance bands, and functional tools. Include eccentric loading.
- Plyometric/Sport-Specific Training: For athletes or those with high-demand occupations.
- Work Simulation: If applicable, gradually integrate work-related tasks.
- Pain Management: Address any residual pain or stiffness.
- Return to Activity: Gradual return to strenuous activities, contact sports, or heavy lifting should be guided by radiographic healing, strength, and symptom resolution. Full return may take 4-6 months, or even up to a year for complex reconstructions.
Specific Considerations
- Scaphoid Nonunion with Grafting: Immobilization may be prolonged (up to 3-4 months) until radiographic signs of union are clear. Rehabilitation often proceeds more cautiously.
- Ligament Reconstruction: The healing process for ligaments can be protracted. Protection of the repair for 3-6 months is not uncommon, with a very gradual increase in load.
- Patient Compliance: Critical for success. Regular communication with the hand therapist and surgeon is essential to manage expectations and ensure adherence to the protocol.
- Monitoring for Complications: Watch for signs of nonunion, stiffness, hardware prominence, or CRPS.
Summary of Key Literature and Guidelines
The management of carpal fractures and dislocations continues to evolve, guided by robust clinical research, biomechanical studies, and consensus guidelines. A critical understanding of the evidence base informs current best practices.
Scaphoid Fractures
- Early ORIF for Displaced/Unstable Fractures: A consensus exists that displaced scaphoid waist fractures (>1mm) or those with significant angulation (>10 degrees) benefit from early open reduction and internal fixation (ORIF) with headless compression screws. This approach reduces nonunion rates and allows for earlier rehabilitation compared to prolonged casting. Literature by Herbert and Fisher (1984) significantly popularized the use of dedicated compression screws.
- Proximal Pole Fractures: High risk of AVN due to retrograde blood supply. Vascularized bone grafts (e.g., 1,2 intercompartmental supraretinacular artery (1,2-ICSRA) flap by Mathoulin and Haerle, 1998) are increasingly utilized for nonunions with proximal pole AVN and for primary treatment in select cases.
- Undisplaced Scaphoid Waist Fractures: While traditional casting remains an option, a growing body of evidence suggests that percutaneous screw fixation may offer faster return to activity and potentially lower nonunion rates without increased complications, particularly in athletes or those with high demands. Bond et al. (2001) and Dias et al. (2010) have contributed to this discussion.
Perilunate Dislocations and Carpal Instability
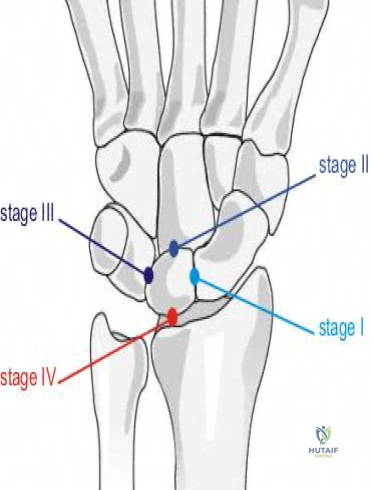
- Urgent Reduction and Stabilization: All perilunate and lunate dislocations require urgent reduction. Open reduction and internal fixation (ORIF) with associated ligament repair/reconstruction and K-wire stabilization is the gold standard, as emphasized by Mayfield et al. (1980) for the sequential failure patterns. Early intervention within days is crucial to prevent progressive stiffness, median nerve compromise, and chronic instability.
- Scapholunate Ligament Repair/Reconstruction: Acute, reducible scapholunate dissociation (SLD) is often treated with direct repair of the scapholunate interosseous ligament (SLIL), augmented by dorsal capsulodesis (e.g., Blatt's capsulodesis or modified dorsal capsulodesis techniques). For chronic, irreducible, or degenerative SLD, salvage procedures such as partial carpal fusions (e.g., four-corner fusion by Watson and Ballet, 1984) or proximal row carpectomy (PRC) are considered.
- Lunotriquetral Ligament Injuries: Less common than SLD. Acute, symptomatic injuries may warrant direct repair. Chronic, painful lunotriquetral dissociation (LTD) can be addressed with ligament reconstruction or lunotriquetral fusion.
Post-Traumatic Arthritis and Salvage Procedures
- SNAC/SLAC Wrist: Scaphoid Nonunion Advanced Collapse (SNAC) and Scapholunate Advanced Collapse (SLAC) are common patterns of post-traumatic arthritis. Management depends on the stage of arthritis.
- Stage I/II (midcarpal arthritis): Proximal row carpectomy (PRC) is a viable option for patients with intact lunate and capitate articular cartilage. Neviaser (1981) provided early descriptions.
- Stage III (radiocarpal involvement): Four-corner fusion (capitate-hamate-triquetrum-lunate fusion with scaphoid excision) is a well-established procedure, offering pain relief and preserved partial motion.
- Advanced Stages/Diffuse Arthritis: Total wrist arthrodesis remains the most reliable pain-relieving procedure, albeit at the cost of motion. Total wrist arthroplasty is an evolving option for select, low-demand patients.
General Guidelines
- Diagnostic Imaging: The role of CT and MRI in accurately diagnosing complex carpal injuries, occult fractures, and ligamentous tears is paramount, often exceeding the utility of plain radiographs alone.
- Arthroscopy: Wrist arthroscopy has emerged as a valuable tool for diagnostic assessment of carpal instability, evaluation of articular damage, and increasingly, for arthroscopically assisted reduction and internal fixation of select carpal fractures and ligament repairs.
- Rehabilitation: Evidence supports structured, phased rehabilitation protocols, emphasizing early controlled motion while protecting the repair, to optimize functional recovery and minimize stiffness.
The literature consistently highlights the importance of a high index of suspicion for carpal injuries, aggressive diagnostic workup, timely and anatomical reduction, stable fixation, and appropriate post-operative rehabilitation to prevent chronic pain and long-term disability. Continued research focuses on improving internal fixation techniques, biological augmentation for healing, and advanced reconstructive strategies.
Clinical & Radiographic Imaging