Unlock Wrist & Hand Secrets: The Ultimate Atlas of Anatomy
Key Takeaway
Learn more about Unlock Wrist & Hand Secrets: The Ultimate Atlas of Anatomy and how to manage it. Wrist and hand anatomy comprises intricate osteology of carpal bones, metacarpals, and phalanges. Arthrology details joints like the radiocarpal, distal radioulnar, and various intercarpal articulations, stabilized by essential ligaments such as the palmar/volar radiocarpal and the TFCC. Understanding these complex structures is vital, as thoroughly documented in a specialized atlas of anatomy.
Introduction and Epidemiology
The human wrist and hand comprise a highly complex, intricately balanced biomechanical system essential for upper extremity function. Mastery of the osseous architecture, ligamentous restraints, and dynamic muscular forces is a prerequisite for any orthopedic surgeon managing traumatic or degenerative conditions of the upper extremity. Carpal injuries, ranging from occult ligamentous sprains to devastating fracture-dislocations, represent a significant proportion of orthopedic trauma. Scaphoid fractures alone account for approximately 60% to 70% of all carpal fractures, while scapholunate ligament injuries are the most common cause of carpal instability.
Despite advances in advanced imaging modalities, a profound understanding of applied surgical anatomy remains the cornerstone of accurate diagnosis and effective operative intervention. Missed injuries, particularly perilunate dislocations and subtle dynamic instabilities, inevitably lead to progressive articular degeneration, manifesting as predictable patterns of radiocarpal and midcarpal arthrosis (e.g., Scapholunate Advanced Collapse).
This comprehensive reference delineates the critical surgical anatomy, biomechanics, and operative strategies required to navigate the wrist and hand. By deconstructing the osteology, arthrology, and complex intercarpal relationships, the orthopedic surgeon can optimize surgical approaches, restore native kinematics, and mitigate the long-term sequelae of carpal derangement.

Surgical Anatomy and Biomechanics
Osteology of the Carpus
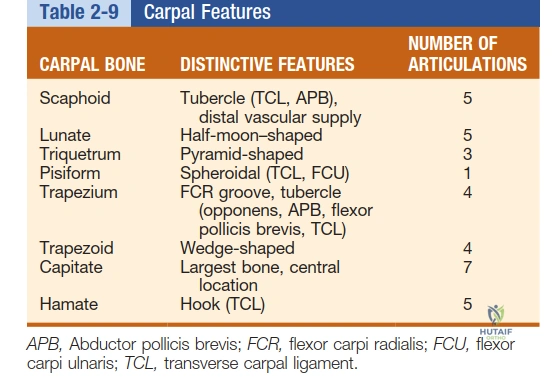
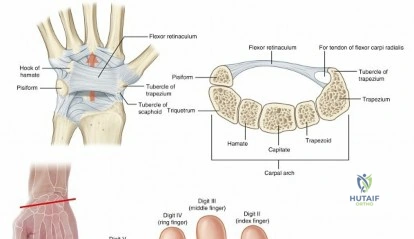
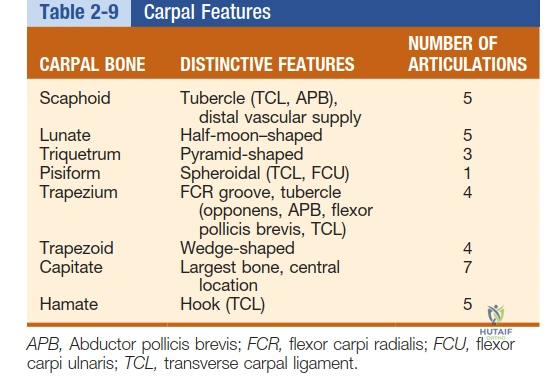
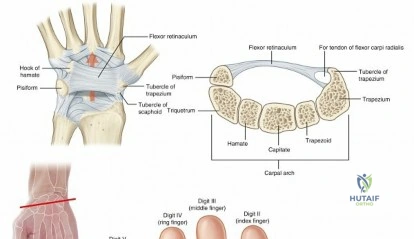
The carpus consists of eight uniquely contoured bones arranged in two distinct rows, serving as a mechanical link between the forearm and the metacarpals. Ossification of the carpal bones occurs in a predictable sequence, which is clinically highly relevant in pediatric orthopedics for determining skeletal maturity. Ossification invariably begins at the capitate, typically present at 1 year of age. From the capitate, ossification proceeds in a counterclockwise direction when viewing posteroanterior radiographs of the right hand (capitate, hamate, triquetrum, lunate, scaphoid, trapezium, trapezoid, and finally the pisiform, which is a sesamoid bone within the flexor carpi ulnaris tendon).
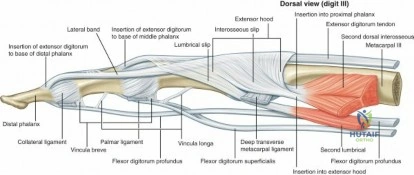
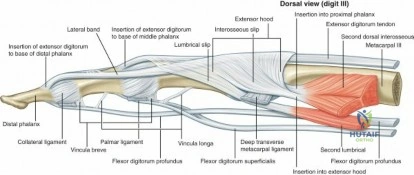
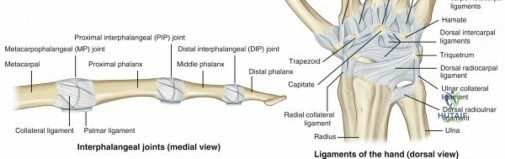
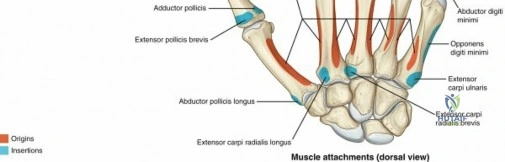
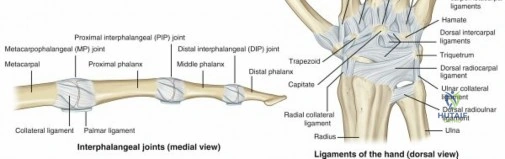
Distal to the carpus, the five metacarpals form the longitudinal arches of the hand. Several morphological characteristics allow for the precise identification of individual metacarpals, dictating the choice of internal fixation during fracture management. The phalanges complete the digital rays, with complex extensor and flexor tendon insertions dictating their dynamic balance.
Arthrology and Ligamentous Anatomy
The distal radioulnar joint (DRUJ) and the radiocarpal joint form the foundational articulations of the wrist. The radiocarpal joint is an ellipsoid articulation involving the biconcave articular surface of the distal radius and the convex proximal surfaces of the scaphoid, lunate, and triquetrum. Topographically, this joint line is located at the level of the proximal wrist flexion crease.
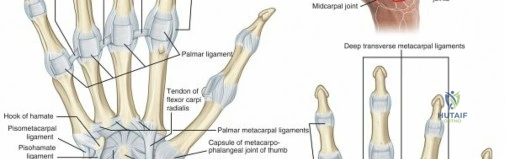
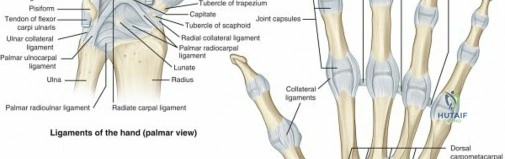
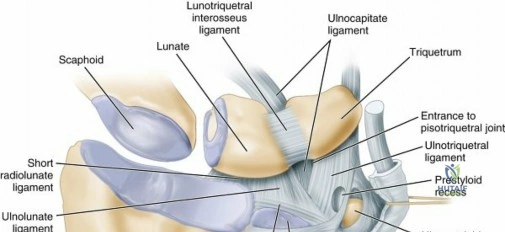
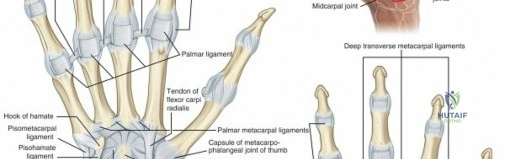
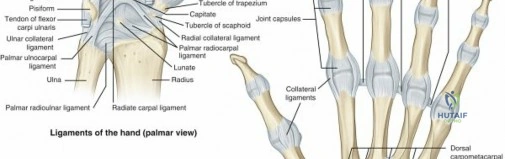
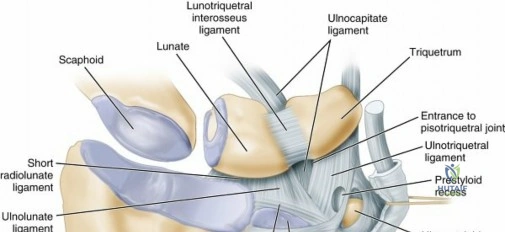
Stability of the radiocarpal and intercarpal joints relies entirely on a complex network of extrinsic and intrinsic ligaments. Extrinsic ligaments bridge the carpal bones to the radius or metacarpals. The palmar (volar) radiocarpal ligaments are significantly thicker and biomechanically stronger than their dorsal counterparts, serving as the primary stabilizers of the wrist. Key volar extrinsic ligaments include the radioscaphocapitate (RSC), long radiolunate (LRL), and short radiolunate (SRL) ligaments.
Intrinsic ligaments originate and insert entirely within the carpus. The most critical of these are the scapholunate (SL) and lunotriquetral (LT) interosseous ligaments.

The Space of Poirier represents a central weak area in the floor of the carpal tunnel, located volarly between the capitate and lunate. This region lacks robust ligamentous support because the volar extrinsic ligaments diverge around it. The Space of Poirier is the primary site of capsular failure during a volar dislocation of the lunate in the terminal stage of a perilunate fracture-dislocation sequence.
The Ligament of Testut (radioscapholunate ligament) was historically considered a mechanical stabilizer but is now recognized primarily as a neurovascular conduit supplying the proximal pole of the scaphoid and the lunate, lacking the collagenous density to provide significant tensile resistance.

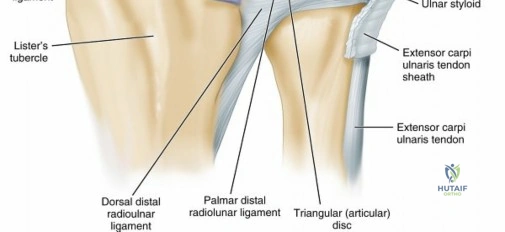
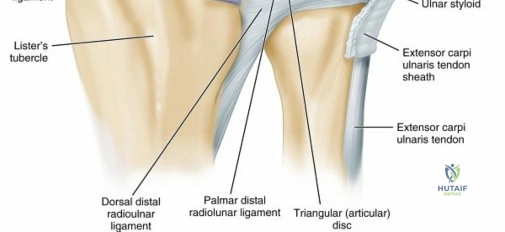
Triangular Fibrocartilage Complex
The Triangular Fibrocartilage Complex (TFCC) is the primary stabilizer of the DRUJ and the ulnar carpus. It comprises the articular disc, dorsal and volar radioulnar ligaments, meniscus homologue, ulnar collateral ligament, and the extensor carpi ulnaris (ECU) subsheath. The vascular supply to the TFCC penetrates only the peripheral 10% to 25% of the complex, rendering the central portion avascular. This anatomic reality dictates surgical decision-making: peripheral tears are amenable to surgical repair, whereas central tears generally require debridement due to an inability to heal.

Carpal Kinematics and Instability Patterns
The intercarpal joints are divided into the proximal and distal rows. The proximal row (scaphoid, lunate, triquetrum) functions as an intercalated segment; no tendons insert directly onto these bones. Their motion is entirely dictated by mechanical pressure from the surrounding articular surfaces and ligamentous tethers.
During radial deviation, the scaphoid naturally flexes. Through the intact scapholunate ligament, it pulls the lunate into flexion. Conversely, during ulnar deviation, the triquetrum extends, pulling the lunate into extension via the lunotriquetral ligament.
* Scapholunate (SL) Ligament Injury: Disruption uncouples the scaphoid and lunate. The scaphoid flexes independently, while the lunate is pulled into extension by the intact triquetrum, resulting in Dorsal Intercalated Segmental Instability (DISI).
* Lunotriquetral (LT) Ligament Injury: Disruption uncouples the lunate and triquetrum. The lunate is pulled into flexion by the intact scaphoid, resulting in Volar Intercalated Segmental Instability (VISI).
Unlike the proximal row, the distal carpal row (trapezium, trapezoid, capitate, hamate) functions as a rigid, tightly bound unit. The interosseous ligaments in the distal row are remarkably thick, with the capitate-hamate ligament being the strongest and the trapezium-trapezoid being the weakest.
The midcarpal joint represents the transverse articulations between the proximal and distal rows. These are reinforced by palmar and dorsal intercarpal ligaments and carpal collateral ligaments, with the radial-sided ligaments demonstrating greater tensile strength.
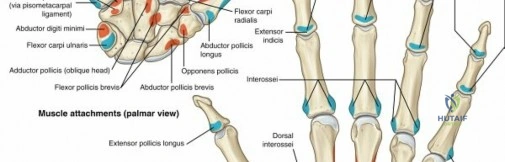
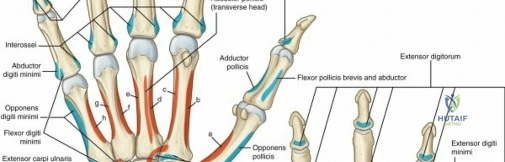
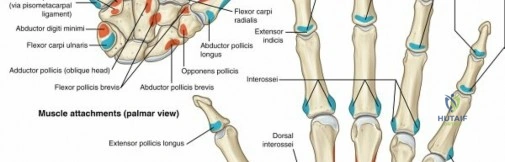
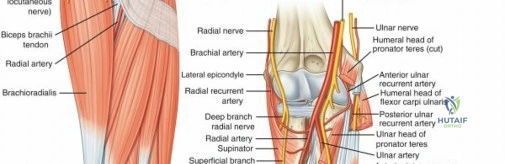
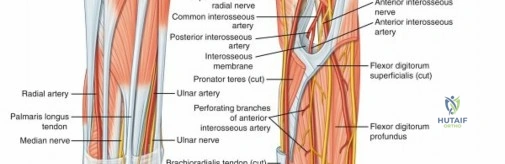
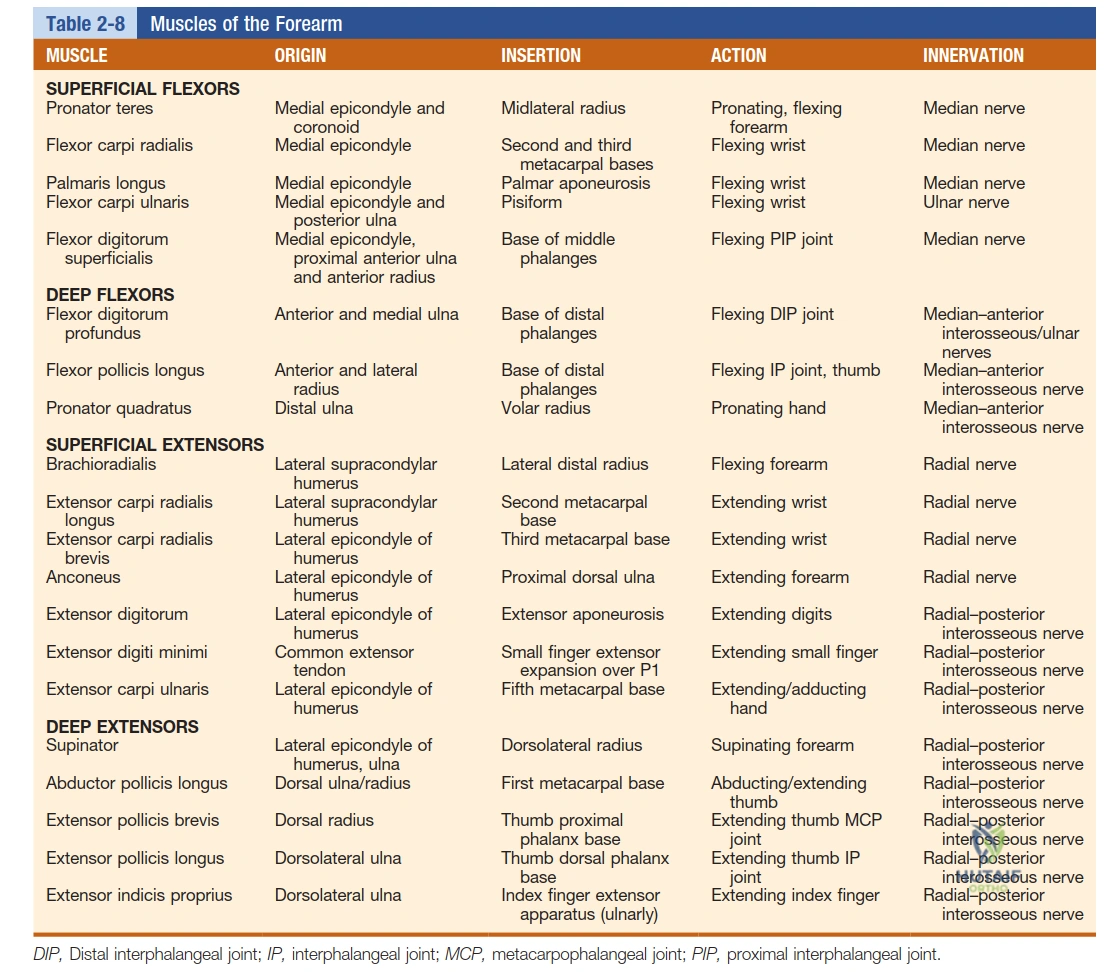
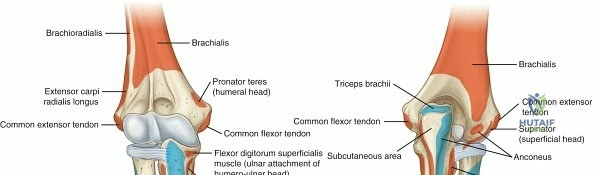
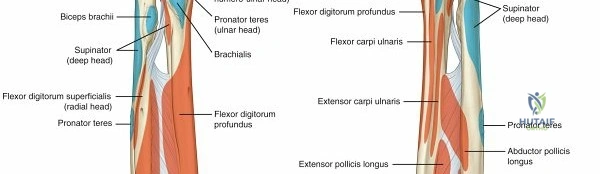
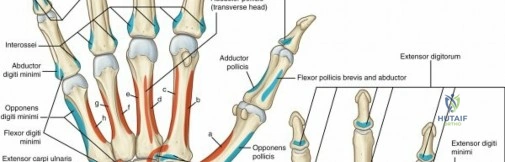
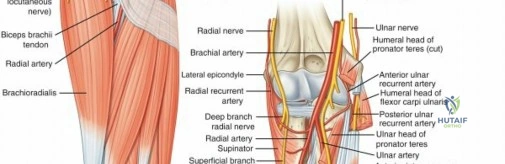
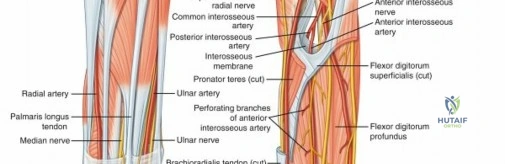
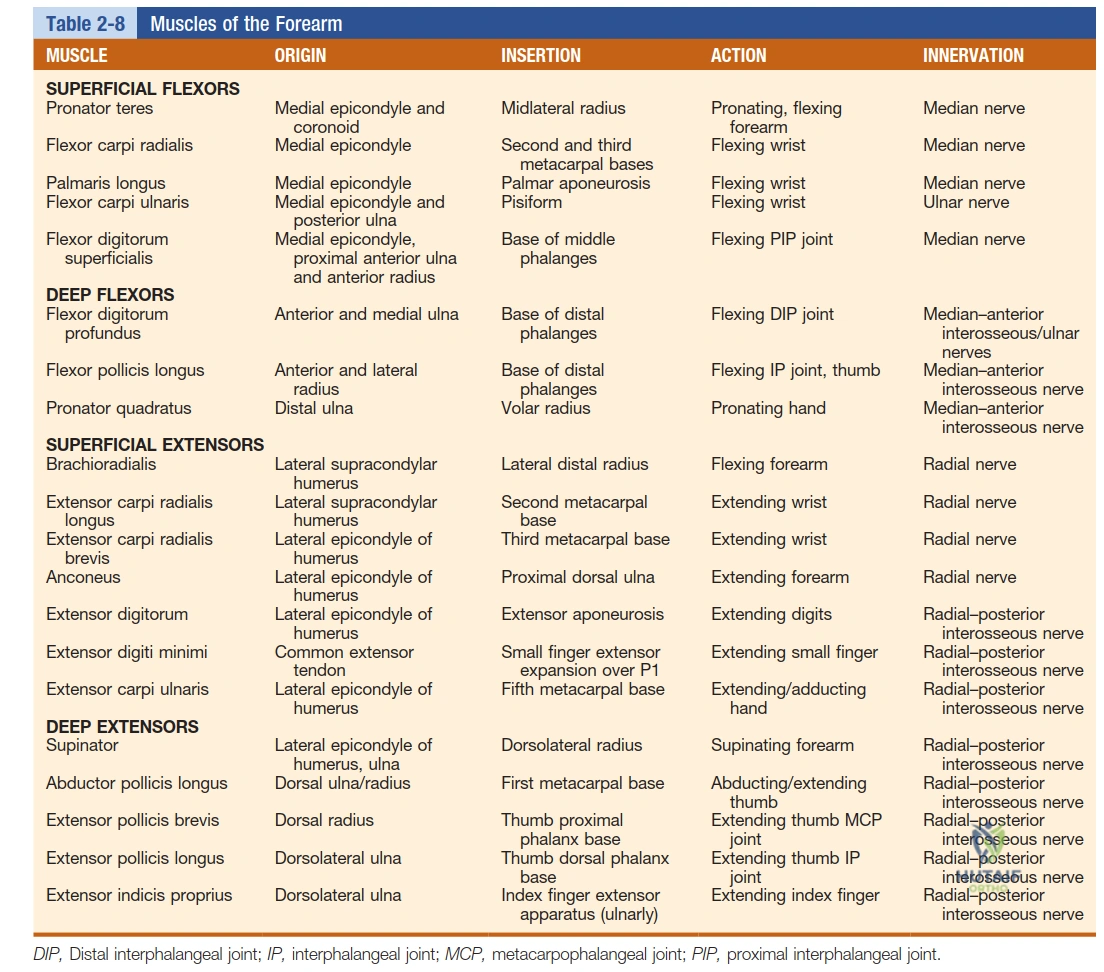
Musculotendinous Anatomy of the Forearm
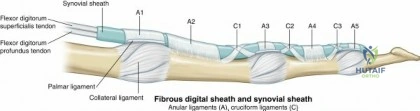
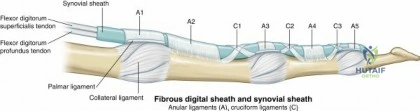
Understanding the dynamic forces crossing the wrist is critical. The superficial flexors of the forearm originate primarily from the medial epicondyle. The pronator teres inserts on the midlateral radius, facilitating pronation. The flexor carpi radialis (FCR) and flexor carpi ulnaris (FCU) provide powerful wrist flexion and deviation, acting as dynamic stabilizers that must be accounted for during rehabilitation and tendon transfer procedures.
Indications and Contraindications
Surgical intervention in the wrist and hand is dictated by the severity of the anatomic disruption, the patient's functional demands, and the presence of progressive instability. The decision matrix relies heavily on identifying whether the pathology involves an isolated ligamentous tear, an axial dislocation, or an osteochondral defect.
| Condition | Operative Indications | Non-Operative Indications | Contraindications to Surgery |
|---|---|---|---|
| Scapholunate Ligament Tear | Acute tears (<4 weeks); Geissler Grade III/IV; DISI deformity; symptomatic chronic tears without arthritis. | Partial tears (Geissler I/II); asymptomatic incidental findings; low-demand patients. | Advanced SLAC arthritis (requires salvage, not repair); active infection. |
| Perilunate Dislocation | ALL acute perilunate and lunate dislocations require urgent open reduction and internal fixation (ORIF). | None. Closed reduction is only a temporizing measure prior to surgery. | Severe soft tissue compromise precluding immediate definitive fixation (temporize with spanning ex-fix). |
| TFCC Tear | Peripheral tears (Palmer 1B) failing conservative care; DRUJ instability. | Central avascular tears (Palmer 1A) initially; asymptomatic degenerative tears. | Fixed DRUJ arthritis (consider Darrach or Sauvé-Kapandji instead of repair). |
| Scaphoid Fracture | Proximal pole fractures; displacement >1mm; intrasubstance comminution; delayed union. | Stable, non-displaced distal pole or waist fractures in compliant patients. | Uncorrectable AVN with advanced radiocarpal collapse. |
Pre Operative Planning and Patient Positioning
Imaging Modalities
Meticulous preoperative imaging is non-negotiable. Standard zero-rotation posteroanterior (PA), true lateral, and oblique radiographs are standard. On the PA view, Gilula’s three carpal arcs must be evaluated; disruption of any arc indicates a severe ligamentous injury or fracture. The lateral radiograph is critical for assessing sagittal plane alignment, specifically measuring the scapholunate angle (normal 30-60 degrees) and the capitolunate angle (normal <15 degrees) to identify DISI or VISI deformities.

Advanced imaging, specifically high-resolution MRI or MR arthrography, is utilized to evaluate the intrinsic ligaments (SL and LT) and the TFCC. Computed Tomography (CT) is invaluable for assessing fracture morphology, particularly in complex intra-articular distal radius fractures or scaphoid nonunions, allowing for precise preoperative templating for screw trajectory and graft placement.
Positioning and Setup
The patient is positioned supine with the operative extremity extended on a radiolucent hand table. A well-padded proximal tourniquet is applied to ensure a bloodless field, which is critical for identifying delicate carpal ligaments and neurovascular structures. The fluoroscopy unit (C-arm) is positioned either parallel or perpendicular to the hand table, depending on surgeon preference, ensuring unimpeded access for dynamic intraoperative imaging. Regional anesthesia (supraclavicular or axillary block) is generally preferred to provide excellent intraoperative muscle relaxation and prolonged postoperative analgesia.
Detailed Surgical Approach and Technique
Dorsal Approach to the Wrist
The dorsal approach provides unparalleled exposure to the proximal carpal row, the midcarpal joint, and the dorsal intrinsic ligaments. It is the workhorse approach for scapholunate ligament repair, proximal row carpectomy, and dorsal perilunate dislocation management.

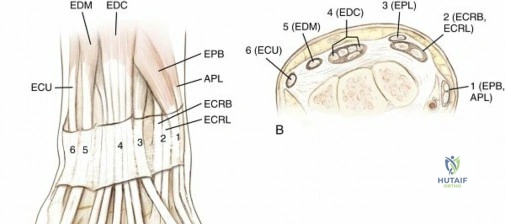
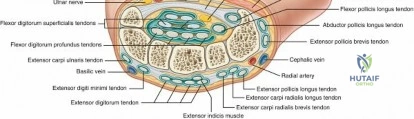
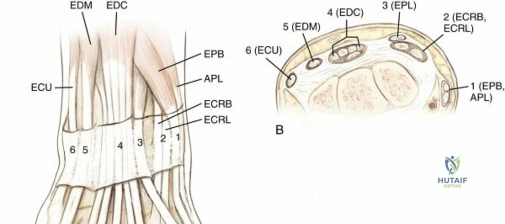
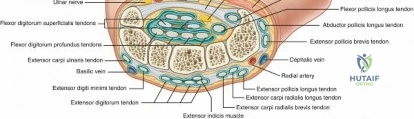
A longitudinal incision is made centered over Lister's tubercle. The extensor retinaculum is exposed, and the third extensor compartment is opened longitudinally. The extensor pollicis longus (EPL) tendon is mobilized and retracted radially. The floor of the third compartment is incised, and subperiosteal elevation of the second and fourth compartments is performed to expose the dorsal wrist capsule.
A ligament-sparing dorsal capsulotomy is essential to preserve secondary stabilizers. The Berger dorsal capsulotomy utilizes a radially based flap, incising along the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments. This exposes the scapholunate interval. In the setting of an acute SL tear, the dorsal band of the SL ligament (the strongest and most critical component) is identified.
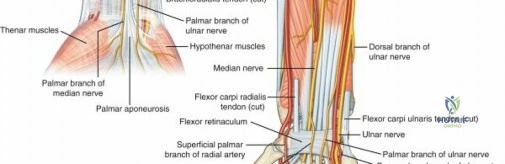
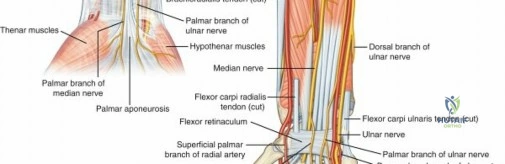
Volar Approach and Carpal Tunnel Release
The volar approach is indicated for volar lunate dislocations, repair of the volar extrinsic ligaments, and fixation of the volar rim of the distal radius. The incision incorporates a standard carpal tunnel release, extending proximally across the wrist crease in a zig-zag fashion to avoid scar contracture.
The transverse carpal ligament is divided, protecting the recurrent motor branch of the median nerve. The flexor tendons are retracted ulnarly, and the median nerve is protected radially. This exposes the volar wrist capsule and the Space of Poirier. In a perilunate dislocation, the lunate will often be found extruded volarly through this defect.

Reduction and Fixation Strategies
For perilunate fracture-dislocations, a combined dorsal and volar approach is frequently necessary. The sequence of reduction is critical:
1. The lunate is reduced back into the lunate fossa via the volar approach, repairing the volar capsule (Space of Poirier) to prevent re-extrusion.
2. Attention is turned dorsally. The scaphoid is reduced to the lunate. This often requires joysticks (Kirschner wires) placed into the scaphoid and lunate to correct the flexion of the scaphoid and the extension of the lunate.
3. Once anatomic alignment is achieved, the SL interval is stabilized with multiple 0.045-inch or 0.062-inch K-wires.
4. The SL ligament is repaired directly using suture anchors placed into the scaphoid footprint.
5. Any associated fractures (e.g., trans-scaphoid perilunate) are fixed rigidly with headless compression screws.

Complications and Management
Surgical management of the wrist is fraught with potential complications, largely due to the tenuous blood supply of the carpal bones and the unforgiving nature of carpal kinematics. Failure to restore precise anatomic relationships inevitably leads to altered contact stresses and rapid articular wear.
| Complication | Incidence | Etiology and Pathomechanics | Salvage Strategy |
|---|---|---|---|
| SLAC Wrist (Scapholunate Advanced Collapse) | High in missed SL tears. | Chronic SL dissociation leads to scaphoid flexion and lunate extension. Abnormal kinematics erode the radioscaphoid joint, progressing to the capitolunate joint. The radiolunate joint is typically spared. | Proximal Row Carpectomy (PRC) or Four-Corner Arthrodesis (scaphoid excision with capitate-hamate-lunate-triquetrum fusion). |
| Avascular Necrosis (AVN) of Scaphoid | 15-30% of proximal pole fractures. | Disruption of the retrograde intraosseous blood supply entering the distal pole of the scaphoid. | Vascularized bone grafting (e.g., 1,2-ICSRA graft, medial femoral condyle free flap). |
| Median Nerve Neuropathy | Common in acute perilunate injuries. | Volar extrusion of the lunate into the carpal tunnel directly compresses the median nerve against the transverse carpal ligament. | Urgent open reduction and concurrent prophylactic carpal tunnel release. |
| Post-Traumatic Stiffness | Nearly universal. | Capsular scarring, prolonged immobilization, and tendon adhesions. | Aggressive early therapy, dynamic splinting, and late arthroscopic or open capsular release if refractory. |
Post Operative Rehabilitation Protocols
Rehabilitation following complex carpal reconstruction must carefully balance the need for tissue
Clinical & Radiographic Imaging